Hi
Hey! How can I help you today?
Paracetamol poisoning
Reading File
Finding Sources
Finding Sources
Searching PubMed
"paracetamol poisoning" AND "N-acetylcysteine"
Reading File
Reading File
Loading Image
Here is a full clinical overview of paracetamol poisoning, sourced from The Essentials of Forensic Medicine and Toxicology, 36th edition (2026):
Paracetamol (Acetaminophen) Poisoning
Doses
| Category | Adults | Children |
|---|---|---|
| Therapeutic dose | 500-1000 mg/dose (max 4 g/day) | 10-15 mg/kg/dose (max 60 mg/kg/day) |
| Toxic dose | ≥150 mg/kg (single ingestion) | ≥150-200 mg/kg |
| Lethal dose | >350 mg/kg | >250-350 mg/kg |
Toxicokinetics and Mechanism
- Absorbed rapidly; peak plasma levels at 30-60 minutes; plasma half-life ~2 hours
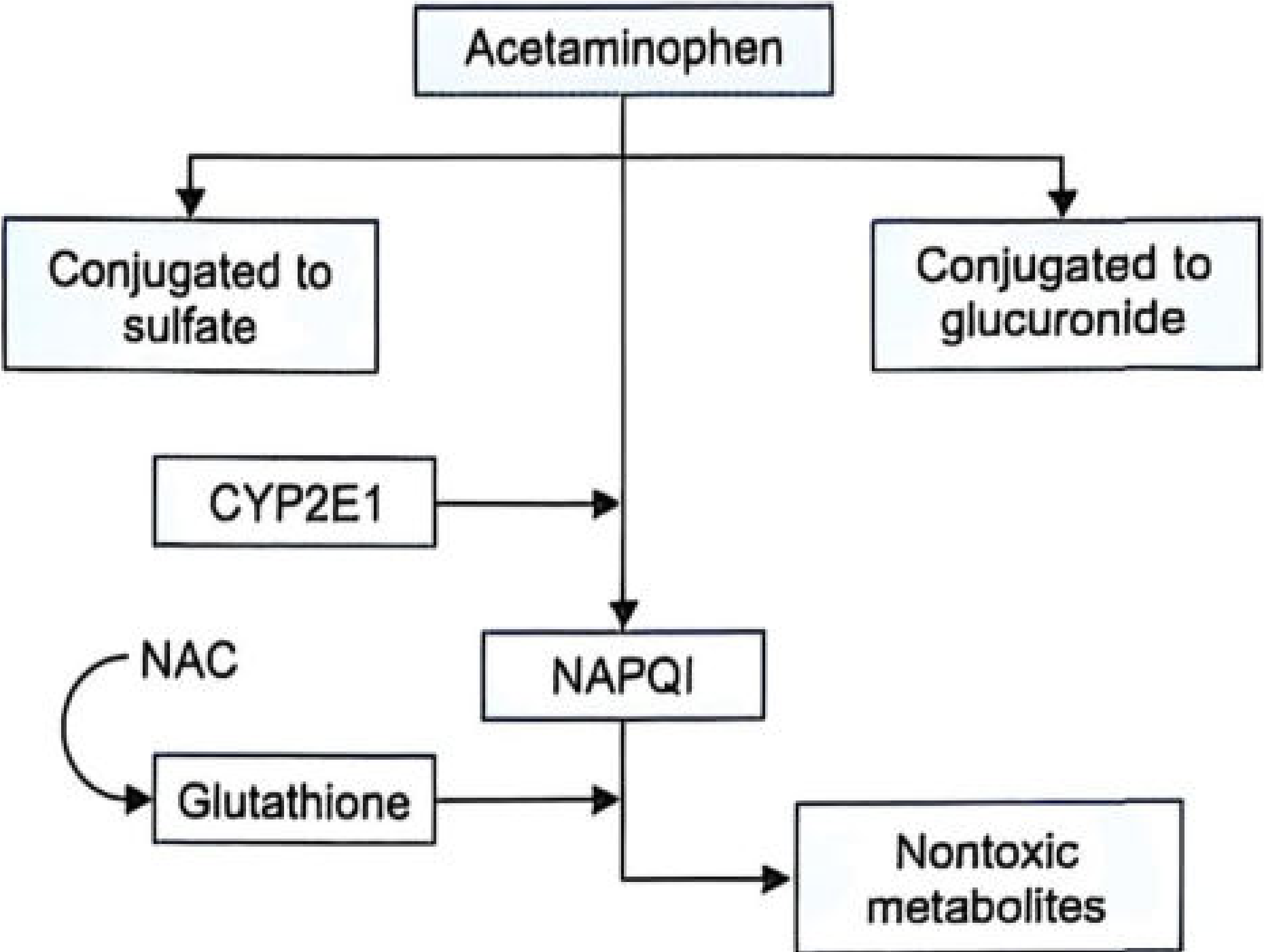
- 90% of hepatic metabolism: conjugation with glucuronide and sulfate → nontoxic metabolites
- ~10% via CYP2E1 → NAPQI (N-acetyl-p-benzoquinone imine)
Detoxification vs Toxicity:
- Normally, NAPQI is neutralized by glutathione → cysteine and mercapturic acid conjugates (safely excreted)
- In overdose, glutathione reserves are exhausted → NAPQI accumulates → binds covalently to liver cell proteins in the centrilobular region → oxidative stress + hepatocyte necrosis
Clinical Stages
| Stage | Timeframe | Clinical Features |
|---|---|---|
| Stage I | 0-24 hours | Nausea, vomiting, anorexia, malaise, pallor, diaphoresis. Often asymptomatic; LFTs usually normal |
| Stage II | 24-72 hours | Right upper quadrant pain; rising AST/ALT and bilirubin; prolonged PT; possible renal involvement |
| Stage III | 72-96 hours | Peak hepatotoxicity: jaundice, coagulopathy, hypoglycemia, hepatic encephalopathy, renal failure, metabolic acidosis, possible multi-organ failure |
| Stage IV | 4-14 days (or more) | Clinical improvement if patient survives; gradual normalization of LFTs; full recovery possible due to liver regeneration |
Management
1. Gastric Lavage
Considered if the patient presents very shortly after ingestion (ideally within the first hour).
2. Activated Charcoal
Given within 1-2 hours post-ingestion to limit absorption. Note: can reduce effectiveness of oral NAC if given together.
3. Antidote - N-Acetylcysteine (NAC)
Most beneficial when given within 8-10 hours of overdose.
Oral NAC:
- Loading dose: 140 mg/kg
- Maintenance: 70 mg/kg every 4 hours (min 24 hrs/6 doses, up to 72 hrs/18 doses)
- Dilute to ~5% using water, soda, or juice
IV NAC (FDA-approved protocol, 21-hour regimen):
- 150 mg/kg over 1 hour (loading)
- Then 50 mg/kg over 4 hours
- Then 100 mg/kg over 16 hours
- Preferred when oral route is compromised (e.g., persistent vomiting)
Methionine (alternative):
- Oral glutathione precursor: 2.5 g every 4 hours for up to 4 doses
- Useful when NAC is unavailable, especially in remote settings
4. Hemodialysis
Considered in severe overdose with extremely high serum levels or metabolic complications/organ failure.
5. Liver Transplantation
Indicated when:
- Severe metabolic acidosis
- Prothrombin time >100 seconds
- Serum creatinine >300 µmol/L
Rumack-Matthew Nomogram
Plots serum paracetamol concentration vs. time since ingestion to guide treatment decisions. Treatment is indicated when levels fall above the treatment line on the nomogram.
Postmortem Findings
- Centrilobular hepatic necrosis
- Acute tubular necrosis
- Myocardial damage
- Cerebral edema
Recent Evidence
A 2025 systematic review and meta-analysis (PMID 40013897) compared two-bag vs. three-bag acetylcysteine regimens in paracetamol poisoning treatment - the two-bag simplified regimen has been gaining evidence as a safer option with fewer anaphylactoid reactions than the traditional three-bag IV protocol.
Source: The Essentials of Forensic Medicine and Toxicology, 36th edition (2026)
This is a shared conversation. Sign in to Orris to start your own chat.