11 Instrumental diagnostic methods of the gastrointestinal tract (X-ray, esophagogastroduodenoscopy, colonoscopy, rectosigmoidoscopy). Gastric juice and stool examination. Coprogram interpretation. Interactive method: "How?"
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have enough foundational textbook content to construct a comprehensive, well-structured answer. Let me synthesize this with my medical knowledge for this topic.
Instrumental Diagnostic Methods of the GI Tract — "How?"
1. X-Ray Methods
Plain Abdominal X-Ray (Survey Radiograph)
How it works:
- Patient stands upright (or lies supine if unable to stand)
- X-rays pass through the abdomen; dense structures (bone, calcifications, metal) appear white; gas appears black
- What it shows: Free air under the diaphragm (perforation), bowel obstruction (air-fluid levels, dilated loops), ileus, calcifications (gallstones, renal stones, aortic calcification), foreign bodies
Contrast Radiography
How it works:
- Barium swallow / upper GI series: Patient drinks barium sulfate suspension; X-rays taken as barium coats mucosa. Shows esophagus, stomach, duodenum — ulcers appear as niches/craters; tumors as filling defects
- Barium enema: Barium introduced rectally via catheter; air then insufflated (double-contrast) to distend the colon. Outlines polyps, tumors, diverticula, strictures
- Contraindications: Suspected perforation (use water-soluble contrast instead), complete obstruction
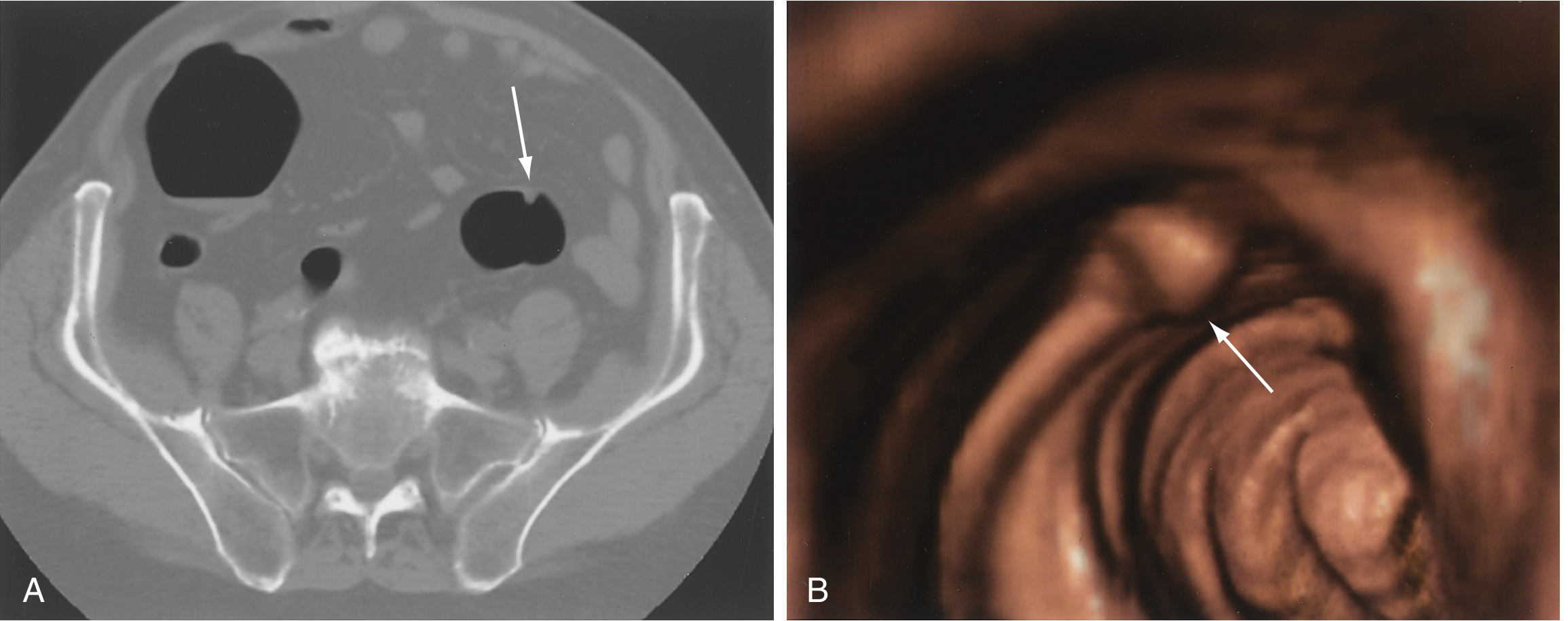
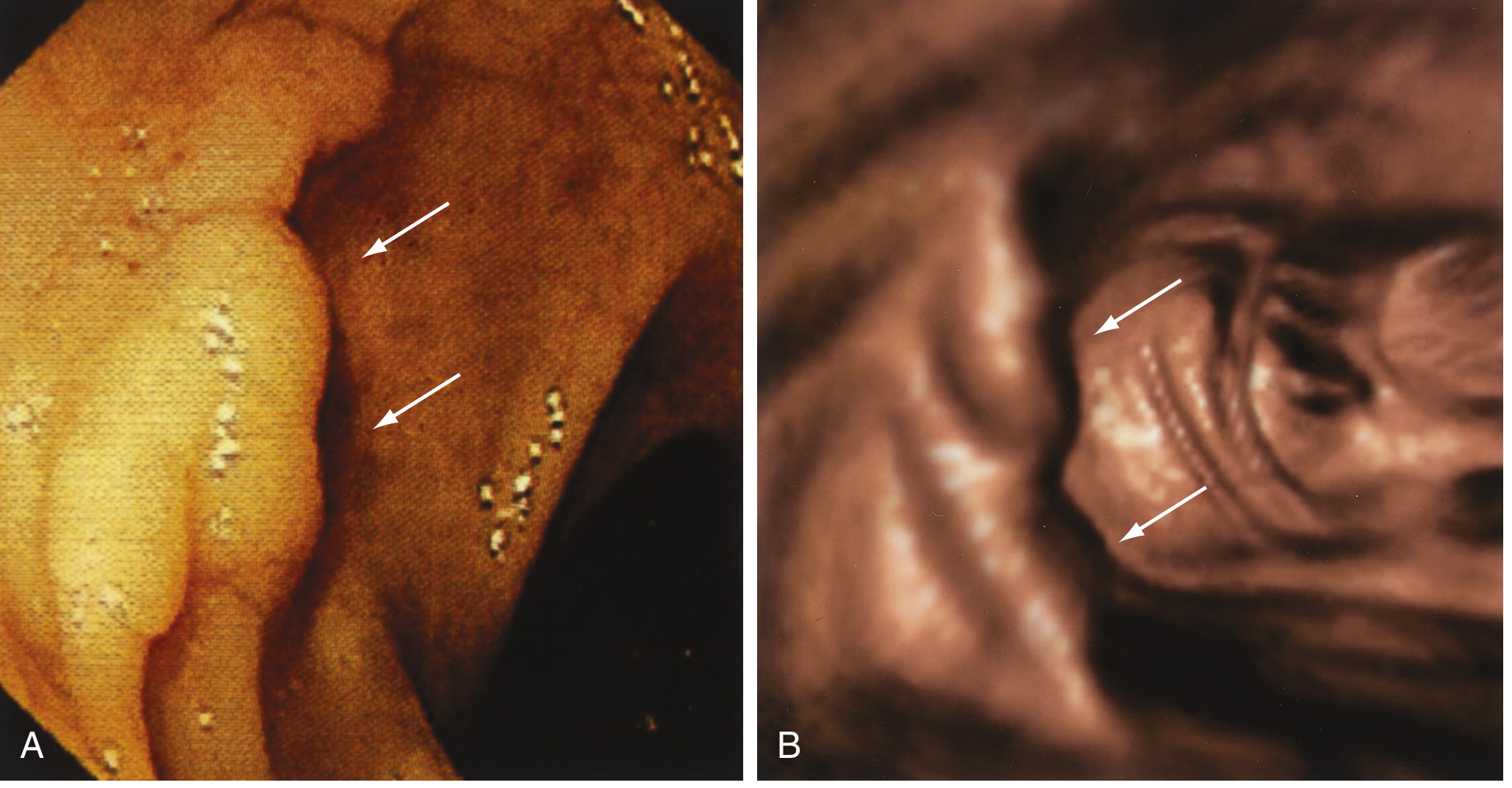
CT of the Abdomen (CT Colonography / "Virtual Colonoscopy")
How it works:
- Patient undergoes bowel prep; air insufflated into colon via rectal tube
- Helical CT creates 2D axial images + 3D endoluminal reconstruction
- Detects polyps ≥6 mm, masses, wall thickening, extraluminal disease
- Advantage: Non-invasive; Disadvantage: Cannot biopsy; radiation exposure
2. Esophagogastroduodenoscopy (EGD / Upper Endoscopy)
How it works:
- Patient fasts ≥6–8 hours; throat sprayed with local anesthetic (lidocaine); IV sedation typically given
- A flexible video endoscope (diameter ~9–12 mm) is passed through the mouth → pharynx → esophagus → stomach → duodenum (D1 and D2)
- The endoscopist insufflates air/CO₂ to distend the lumen and visualize mucosa under white-light illumination
- Advanced imaging: Narrow-band imaging (NBI) enhances vascular patterns; chromoendoscopy uses dye (e.g., indigo carmine) to highlight flat lesions
What it detects:
| Structure | Findings |
|---|---|
| Esophagus | Varices, Barrett's esophagus, strictures, tumors, esophagitis |
| Stomach | Ulcers, gastritis, polyps, carcinoma, MALT lymphoma |
| Duodenum | Duodenal ulcer, celiac disease (villous atrophy on biopsy), ampullary pathology |
Therapeutic uses: Hemostasis (injection, clipping, banding), polypectomy, foreign body removal, dilation of strictures, PEG tube placement
Contraindications: Suspected perforation, severe hemodynamic instability, uncooperative patient
Note on vascular lesions (angioectasias): Appear as cherry-red, fern-like arborizing vessels. Should be examined on insertion, not withdrawal, as suction artifacts may mimic them. Meperidine may mask lesions by reducing mucosal blood flow; naloxone reversal may enhance detection. — Clinical Gastrointestinal Endoscopy, 3e
3. Colonoscopy
How it works:
- Patient performs full bowel prep (polyethylene glycol or sodium phosphate solution) the day before
- Under IV sedation, a long flexible colonoscope (~130–160 cm) is inserted per rectum and advanced through the entire colon to the ileocecal valve (and often terminal ileum)
- Air or CO₂ insufflation distends the lumen; the endoscopist uses torque, tip deflection, and patient positioning
- Withdrawal phase (minimum 6–8 minutes) is the critical detection phase
What it detects:
- Colorectal polyps (adenomas, serrated lesions), carcinoma, IBD (ulcerative colitis, Crohn's), diverticula, angioectasias, infectious colitis
Therapeutic uses: Polypectomy (snare/forceps), hemostasis, stricture dilation, stent placement, decompression of pseudo-obstruction
Screening: Colonoscopy every 10 years starting at age 45 reduces CRC incidence by 62–88% and mortality by 79–90% (USPSTF modeling data). Polypectomy reduces CRC mortality by ~53% at 15.8 years follow-up (National Polyp Study). — Sleisenger & Fordtran's GI and Liver Disease
Enhanced imaging: Chromoendoscopy (dye spray), NBI, iScan — improve flat adenoma detection, especially in IBD/Lynch syndrome
4. Rectosigmoidoscopy (Sigmoidoscopy)
How it works:
- Rigid sigmoidoscope (25–30 cm): Patient in knee-chest or left lateral position; rigid tube inserted; primarily examines rectum and distal sigmoid. Mainly used for rectal pathology (hemorrhoids, polyps, proctitis, biopsy)
- Flexible sigmoidoscope (~60 cm): More comfortable; examines sigmoid and descending colon to splenic flexure; shorter prep (enemas only, no full bowel prep)
Advantages over colonoscopy: No sedation required, less preparation, faster, lower cost
Limitation: Only examines left colon; right-sided lesions missed. Used as a first-line screening tool where colonoscopy is unavailable, or in combination with FIT (stool test)
5. Gastric Juice Examination
How it performed:
- Patient fasts overnight
- Nasogastric tube inserted; basal gastric juice aspirated for 1 hour (BAO = basal acid output)
- Stimulated secretion: pentagastrin or histamine injected subcutaneously; gastric juice collected every 15 min × 4 (MAO = maximal acid output)
Normal values:
| Parameter | Normal |
|---|---|
| BAO | 1–5 mEq/h |
| MAO | 10–25 mEq/h |
| BAO/MAO ratio | <0.2 |
| pH | 1.5–2.5 (fasting) |
Clinical interpretation:
| Condition | Finding |
|---|---|
| Duodenal ulcer / Zollinger-Ellison | ↑↑ BAO, ↑ MAO, BAO/MAO >0.6 |
| Gastric ulcer | Normal or ↑ acid |
| Gastric carcinoma | Achlorhydria (no acid even with stimulation) |
| Pernicious anemia / Atrophic gastritis | Achlorhydria |
| Helicobacter pylori infection | May show normal or increased acidity |
Additional examination of gastric juice:
- Microscopy: Presence of blood, bile, food remnants (gastric stasis), bacteria (sarcinae in achlorhydria), tumor cells (cytology)
- Occult blood: Suggests ulcer or carcinoma
- Lactic acid (Boas-Oppler sign): Present in achlorhydric states (achlorhydria → bacterial fermentation → lactic acid accumulation) — historically a marker for gastric cancer
6. Stool Examination & Coprogram
Collection
- Fresh stool collected into clean container; examined within 1–2 hours (or refrigerated briefly)
- Patient avoids iron, bismuth, NSAIDs, beets, red meat 3 days prior (for occult blood testing)
Coprogram — Systematic Interpretation
Macroscopic (Physical Properties)
| Parameter | Normal | Abnormal Significance |
|---|---|---|
| Consistency | Soft, formed | Liquid (diarrhea), hard pellets (constipation) |
| Color | Brown (stercobilin) | Black/tarry (melena — upper GI bleed); red (hematochezia — lower GI); pale/clay (obstructive jaundice — no bile); green (rapid transit/infection) |
| Shape | Cylindrical | Ribbon-like (rectal stricture); scybala (constipation) |
| Odor | Normal | Putrid = putrefactive dyspepsia; sour = fermentative dyspepsia |
| Mucus | Absent | Present in IBD, IBS, dysentery, tumors |
| Blood | Absent | Visible = hemorrhoid, fissure, colorectal cancer, dysentery |
| Parasites | Absent | Ascaris, tapeworm segments visible macroscopically |
Microscopic (Microsopy of Stool)
| Finding | Normal | Abnormal Significance |
|---|---|---|
| Muscle fibers (creatorrhea) | None/few | Unstriated = normal; striated = pancreatic exocrine insufficiency, rapid transit |
| Fat (steatorrhea) | Absent | Neutral fat ↑ → pancreatic insufficiency (lipase deficiency); fatty acids ↑ → malabsorption (small bowel, e.g., celiac) |
| Starch (amilorrhea) | Absent | Pancreatic insufficiency, rapid transit |
| Leukocytes | None/rare | >10/hpf → inflammatory colitis, dysentery, IBD |
| Red blood cells | Absent | Colorectal inflammation, ulceration, carcinoma |
| Epithelial cells | Rare | ↑ in colitis, tumor desquamation |
| Bacteria/parasites | Normal flora | Ova, larvae, cysts (Giardia, Entamoeba, Ascaris) |
| Yeast/fungi | Absent | Candida in immunosuppressed, antibiotic use |
Chemical Tests
| Test | Purpose | Significance |
|---|---|---|
| Occult blood (guaiac / immunochemical FIT) | Detects hemoglobin peroxidase | Positive in GI bleeding, CRC screening |
| Reaction (pH) | pH strip | Acid (pH <6) = fermentative dyspepsia; Alkaline (pH >8) = putrefactive/protein malabsorption |
| Stercobilin | Bile pigment oxidation product | Absent → obstructive jaundice, complete bile duct obstruction |
| Bilirubin | Direct pigment | Present in infants (normal); in adults = rapid transit bypasses bacterial reduction |
Summary of Coprogram Patterns
| Syndrome | Key Coprogram Features |
|---|---|
| Pancreatic exocrine insufficiency | Steatorrhea (neutral fat), creatorrhea (striated fibers), amilorrhea, large bulky stool, pale |
| Small bowel malabsorption (celiac) | Fatty acids, steatorrhea, bulky, pale, alkaline |
| Obstructive jaundice | Clay/acholic stool, no stercobilin, no bilirubin |
| Ulcerative colitis/dysentery | Liquid, mucus++, RBCs, leukocytes++, bloody |
| Upper GI bleed | Black tarry (melena), occult blood positive |
| Lower GI bleed | Red blood mixed with stool or on surface |
| Fermentative dyspepsia | Foamy, yellow, sour smell, acid pH, ↑ starch, ↑ fatty acids |
| Putrefactive dyspepsia | Dark, alkaline, putrid smell, ↑ striated muscle fibers |
Quick Summary: "How?" — Method Logic
| Method | Key Principle |
|---|---|
| X-ray | Contrast differences (air vs. tissue vs. metal); barium coats/fills lumen |
| EGD | Direct mucosal visualization + biopsy via flexible scope, mouth to duodenum |
| Colonoscopy | Full colonic visualization + intervention via flexible scope, anus to cecum |
| Sigmoidoscopy | Limited (rectum/sigmoid) direct visualization; no full prep/sedation |
| Gastric juice | Quantitative acid measurement (BAO/MAO); achlorhydria vs. hyperacidity |
| Stool exam/Coprogram | Physical, microscopic, chemical analysis of digestive residues |
Sources: Clinical Gastrointestinal Endoscopy (Expert Consult, 3e); Sleisenger and Fordtran's Gastrointestinal and Liver Disease; standard internal medicine/gastroenterology reference knowledge.
This is a shared conversation. Sign in to Orris to start your own chat.