Everything about renal trauma in detail with reference to standard textbooks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the detailed answer.
Renal Trauma — A Comprehensive Review
1. Epidemiology
Renal injuries are the most common urologic injuries in trauma, occurring in approximately 10% of all blunt and penetrating abdominal trauma cases. The kidney is the most commonly injured genitourinary organ.
- ~80–90% of cases result from blunt trauma (motor vehicle accidents, falls, sports injuries, direct blows to the flank)
- 10–20% result from penetrating trauma (gunshot wounds, stab wounds, iatrogenic injury during renal biopsy or surgery)
- Isolated renal injuries are uncommon; co-injuries to other abdominal organs are frequent
The paediatric kidney is disproportionately vulnerable — it is larger relative to body size, more mobile, has less protective perirenal fat, and is shielded by less-ossified ribs. Patients with underlying renal anomalies (horseshoe kidney, ectopic kidney, hydronephrosis, renal cysts or neoplasms, renal transplants) are especially susceptible to injury disproportionate to the mechanism.
— Grainger & Allison's Diagnostic Radiology, p. 920
— Campbell-Walsh-Wein Urology
— Campbell-Walsh-Wein Urology
2. Anatomy & Mechanisms of Injury
Anatomy Relevant to Trauma
The kidneys are retroperitoneal organs protected by the lower ribs, vertebral column, paraspinal muscles, and perirenal fat within Gerota's fascia. Despite these protections, they are vulnerable to:
- Direct compression against the ribs and lumbar vertebrae
- Deceleration forces transmitted via the renal pedicle
Blunt Trauma Mechanisms
- Direct blow to the flank → contusion or laceration as the kidney is compressed against ribs and vertebrae
- Rapid deceleration (high-speed MVA, fall from height) → shearing forces cause:
- Parenchymal lacerations
- Tearing of the collecting system at the pelvicoureteric junction (PUJ)
- Stretching of accessory or intrarenal arteries → segmental infarction
- Lateral kidney displacement → stretching of renal vasculature → intimal tears, dissection, thrombosis of the main renal pedicle (the artery typically occludes at its proximal to middle third)
- Overstretching → complete hilar avulsion
Penetrating Trauma
- Gunshot wounds and stab wounds account for the majority
- Penetrating injuries are more likely to injure adjacent viscera (up to 80% of patients have associated injuries), increasing the need for surgical exploration
- Renal injuries occur in ~5% of penetrating flank/back wounds
— Grainger & Allison's Diagnostic Radiology, p. 920
3. Classification — AAST Organ Injury Scale
The American Association for the Surgery of Trauma (AAST) grading system is the universal standard. The scale was originally developed by Moore et al. (1989) and was subsequently updated to reflect modern management data.
| Grade | Type | Description |
|---|---|---|
| I | Contusion | Microscopic or gross hematuria; urologic studies normal |
| Hematoma | Subcapsular, non-expanding, without parenchymal laceration | |
| II | Hematoma | Non-expanding perirenal hematoma confined to renal retroperitoneum |
| Laceration | <1 cm parenchymal depth of renal cortex; no urinary extravasation | |
| III | Laceration | >1 cm parenchymal depth of renal cortex; no collecting system rupture or urinary extravasation |
| IV | Laceration | Parenchymal laceration extending through cortex, medulla, AND collecting system |
| Vascular | Main renal artery or vein injury with contained hemorrhage; also AV malformation or pseudoaneurysm (updated) | |
| V | Laceration | Completely shattered kidney; shattered kidney with loss of identifiable parenchymal anatomy (updated) |
| Vascular | Avulsion of renal hilum, devascularizing the kidney; devascularized kidney with active bleeding (updated) |
Note: Advance one grade for bilateral injuries up to Grade III.
Grades I–III account for the vast majority (~95%) of renal injuries. Only ~5% are Grade IV–V.
— Campbell-Walsh-Wein Urology, Table 90.1
— Sabiston Textbook of Surgery
— Sabiston Textbook of Surgery
4. Clinical Features
History
- Mechanism: high-energy blunt impact or direct flank blow; type of projectile for penetrating injury
- Any high-energy impact, fall from height, rapid deceleration, or direct flank/abdominal blow raises suspicion
- Accompanying injuries are common given the kidney's anatomic protection (implying significant force is required)
Symptoms & Signs
- Hematuria (gross or microscopic) — present in ~95% of renal trauma cases
- Critically, the degree of hematuria does NOT correlate with the severity of injury
- Gross hematuria may occur with minor trauma; significant injuries (including complete renal artery thrombosis, pedicle avulsion, ureteropelvic disruption) can occur with minimal or no hematuria
- Flank pain, tenderness, fullness, or ecchymosis
- Loss of flank contour
- Lower rib or vertebral fractures (associated with renal injury)
- Palpable flank/abdominal mass (expanding hematoma)
- Hemodynamic instability (hypotension, tachycardia) in severe injuries
- Abdominal tenderness or distention
— Rosen's Emergency Medicine, p. 506
— Smith and Tanagho's General Urology
— Smith and Tanagho's General Urology
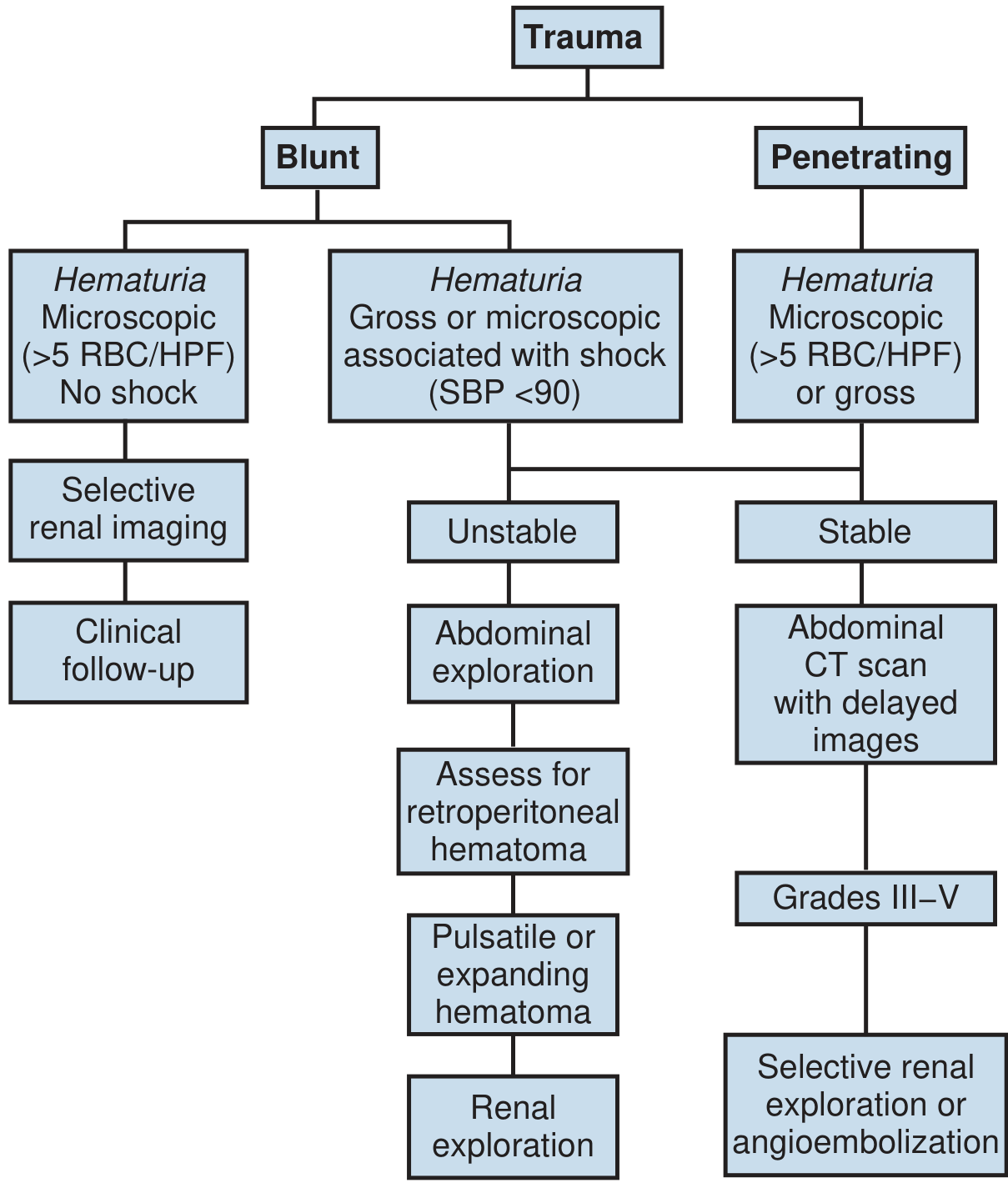
5. Indications for Imaging
Imaging is critical for grading and guiding management. Hemodynamically unstable patients who cannot be rapidly resuscitated are taken directly to the operating room.
AUA & EAU Guidelines — Indications for CT Imaging
- All penetrating trauma with likelihood of renal injury (abdomen, flank, ipsilateral rib fracture, significant flank ecchymosis, low chest entry/exit wound) — in hemodynamically stable patients
- Blunt trauma with significant acceleration/deceleration mechanism (high-speed MVA, fall from height)
- Blunt trauma with gross hematuria
- Blunt trauma with microhematuria AND hypotension (SBP <90 mmHg at any time)
- All pediatric patients with >50 RBC/HPF on urinalysis
Key principle: Microhematuria without shock in blunt trauma does NOT mandate imaging — injuries found are typically minor and rarely require intervention.
— Campbell-Walsh-Wein Urology, p. 2643
— Rosen's Emergency Medicine
— Rosen's Emergency Medicine
6. Imaging
Contrast-Enhanced CT (CECT) — Gold Standard
CECT is the best imaging modality for assessing and grading renal trauma. Multiphase imaging includes:
- Arterial phase: identify active arterial extravasation ("blush")
- Portal venous/nephrographic phase: assess parenchymal integrity and lacerations
- 10-minute delayed phase (CT urogram): identify collecting system injuries and urinary extravasation
CT Findings and Their Significance
| Finding | Significance |
|---|---|
| Medial hematoma | Vascular pedicle injury |
| Medial urinary extravasation | Renal pelvis or UPJ injury |
| Lack of contrast enhancement | Main renal arterial injury (thrombosis/occlusion) |
| Active intravascular contrast extravasation ("blush") | Arterial injury with brisk/active bleeding |
| Perirenal hematoma | Contained parenchymal injury |
| Segmental non-enhancement | Branch vessel injury/infarct |
Other Imaging Modalities
- IVP (intraoperative): Single-shot IV pyelogram (2 mL/kg contrast, 10-minute film) used intraoperatively to confirm a functioning contralateral kidney before nephrectomy
- Angiography: Diagnostic and therapeutic for embolization; used when CT shows active extravasation or pseudoaneurysm
- Ultrasound: Limited sensitivity for parenchymal injury; useful in follow-up or pregnancy
— Campbell-Walsh-Wein Urology, p. 2643–2644
— Grainger & Allison's Diagnostic Radiology, p. 920
— Grainger & Allison's Diagnostic Radiology, p. 920
7. Management
General Principles
Management is dictated by:
- Hemodynamic status
- Injury grade (AAST)
- Mechanism (blunt vs. penetrating)
- Associated injuries
- Presence/absence of active bleeding
A. Non-Operative Management (NOM)
NOM is the standard of care for hemodynamically stable, well-staged patients with AAST Grades I–IVa injuries regardless of mechanism.
- Over 90% of all renal injuries can be successfully managed without surgery
- Even select Grade IV and V injuries can be managed non-operatively with careful patient selection and monitoring
- Conservative management of high-grade injuries has not been associated with increased length of stay and may yield higher renal preservation rates
NOM for blunt trauma:
- Grade I–III: Bed rest, monitoring, serial urinalysis
- Grade IV–V (selected stable patients): Close observation, serial imaging, early angioembolization readiness
- Urinary extravasation often resolves spontaneously and does not mandate intervention per se
NOM for penetrating trauma:
- Isolated renal stab wounds: 55% successfully managed non-operatively
- Isolated low-velocity gunshot wounds: 24% (select cases) managed conservatively
- Stab wounds posterior to the posterior axillary line are more amenable to NOM (less visceral injury risk)
- Requires frequent serial abdominal exams (especially first 24 hours); new tenderness or guarding → abdominal exploration
Absolute indications for intervention (surgical or angiographic):
- Hemodynamic instability despite resuscitation
- Expanding or pulsatile retroperitoneal hematoma at exploration
- Penetrating trauma with suspicion of visceral injury
— Campbell-Walsh-Wein Urology, p. 2646
B. Angioembolization
Selective angioembolization is a minimally invasive, highly effective modality for controlling active bleeding:
- Indicated for: active arterial extravasation on CT ("blush"), traumatic pseudoaneurysm, arteriovenous fistula
- Useful for Grade IV–V injuries with evidence of arterial hemorrhage in hemodynamically stable or transiently stabilized patients
- Significant delayed renal bleeding (occurs in ~9% of NOM cases) is usually amenable to embolization
- Allows maximal renal preservation compared to surgery
— Campbell-Walsh-Wein Urology, p. 2645
C. Operative Management
Indications for Surgical Exploration
- Hemodynamic instability not responding to resuscitation (exsanguinating hemorrhage)
- Expanding pulsatile retroperitoneal hematoma found at laparotomy
- Grade V vascular injury (hilar avulsion)
- Penetrating injuries with peritoneal signs or associated visceral injury
- Uncontrolled bleeding after angioembolization fails
Surgical Approach — Operative Steps
- Midline transabdominal approach is preferred — allows access to the aorta and IVC for proximal vascular control before entering Gerota's fascia
- Proximal vascular control first: Expose the aorta at the level of the inferior mesenteric artery; identify and control the renal vessels before opening the hematoma
- Renal exploration: Incise Gerota's fascia; assess extent of parenchymal and vascular injury
- Renal reconstruction (renorrhaphy):
- Debride non-viable tissue
- Achieve hemostasis (absorbable sutures, argon beam coagulator, hemostatic agents)
- Repair collecting system with absorbable sutures (watertight closure)
- Cover with perirenal fat, omentum, or oxidized cellulose
- Nephrectomy: Reserved for:
- Unstable patients with severe injury where renorrhaphy is not feasible
- Shattered kidney with no salvageable parenchyma
- Renal pedicle avulsion
- Always confirm a functioning contralateral kidney (IVP or palpation) before nephrectomy
— Sabiston Textbook of Surgery
— Campbell-Walsh-Wein Urology
— Campbell-Walsh-Wein Urology
D. Management by Grade Summary
| Grade | Management |
|---|---|
| I–II | Conservative: bed rest, analgesics, serial UA; discharge when hematuria resolves |
| III | Conservative; observation ± repeat imaging; most resolve spontaneously |
| IV | Conservative in stable patients; angioembolization for active bleeding; surgical for unstable or collecting system avulsion |
| V | Surgical exploration usually required; angioembolization in select stable patients; nephrectomy often necessary |
8. Special Situations
Renal Pedicle Injury
- Renal artery thrombosis following deceleration injury: Typically presents with complete absence of contrast enhancement on CT with no hematoma
- Warm ischemia time is critical: revascularization within 4–6 hours offers the best chance of renal recovery
- Delayed diagnosis (>6 hours) makes successful revascularization unlikely; observation vs. nephrectomy
- Complete avulsion → immediate surgical exploration
Ureteropelvic Junction (UPJ) Disruption
- Caused by rapid deceleration with avulsion at the fixed UPJ
- CT findings: medial urinary extravasation, lack of contrast opacifying the ureter
- Management: surgical repair (pyeloplasty or primary anastomosis) in most cases
Pediatric Renal Trauma
- Children have relatively larger kidneys, less perirenal fat, more pliable ribs → greater vulnerability
- More than 50 RBC/HPF on UA in pediatric blunt trauma warrants imaging
- NOM is similarly preferred; outcomes are generally favorable
Underlying Renal Anomalies
- Horseshoe kidney, ectopic kidney, hydronephrosis → injury disproportionate to mechanism
- Should be suspected when CT findings seem "too severe" for the reported force
- An example: complete disruption of the horseshoe kidney isthmus from a fall from height (see Grainger & Allison image, Fig. 36.1)
9. Complications
| Complication | Notes |
|---|---|
| Delayed hemorrhage | Occurs in ~9% of NOM cases; typically managed with angioembolization |
| Urinary extravasation / Urinoma | Often resolves spontaneously; persistent cases: ureteral stenting ± percutaneous nephrostomy |
| Perinephric abscess | Rare; preceded by urinary extravasation; managed with percutaneous drainage |
| Hypertension (post-traumatic) | Uncommon in early period; three mechanisms: (1) Goldblatt kidney — renal artery stenosis/occlusion activating RAAS; (2) Page kidney — perirenal hematoma/urinoma compressing renal parenchyma; (3) Post-traumatic AV fistula → all stimulate renin-angiotensin axis |
| Renal function decline | Correlates with injury severity; retrospective data shows postinjury decline in renal function proportional to grade |
| Stricture / Hydronephrosis | From collecting system injury or ureteral damage |
Hypertension developing or persisting >30 days after renal injury should raise suspicion for renal trauma-related hypertension. The risk is uncommon with Grade I–II injuries but rises significantly with higher grades.
— Campbell-Walsh-Wein Urology, p. 2651
10. Key Points Summary
- ~80% blunt, ~10–20% penetrating mechanism; kidney is the most commonly injured GU organ
- Hematuria does not correlate with injury severity — significant injuries (pedicle avulsion, UPJ disruption) can occur without hematuria
- Microhematuria + no shock in blunt trauma = no mandatory imaging
- CECT is the gold standard imaging; 10-minute delayed phase is essential for collecting system evaluation
- AAST grading (I–V) guides management
- NOM is standard for Grades I–IVa in hemodynamically stable patients — over 90% are managed non-operatively
- Angioembolization is the first-line intervention for active arterial bleeding in stable patients
- Surgery for hemodynamic instability, expanding hematoma, failed embolization, or Grade V vascular injury
- Nephrectomy is a last resort; always confirm contralateral renal function before proceeding
- Complications: delayed hemorrhage (~9%), urinoma, perinephric abscess, post-traumatic hypertension (Goldblatt/Page kidney/AV fistula), chronic renal function decline
References
- Campbell-Walsh-Wein Urology, 12th Ed. — Chapter 90: Renal Trauma (Key Points, AAST Grading, Imaging Indications, Nonoperative Management, Complications)
- Sabiston Textbook of Surgery, 21st Ed. — Urologic Trauma: Renal Trauma (AAST Updated Scale, Imaging, Management, Operative Approach)
- Grainger & Allison's Diagnostic Radiology — Chapter 36: Renal Trauma (Epidemiology, Mechanisms, Imaging Technique)
- Rosen's Emergency Medicine: Concepts and Clinical Practice — Chapter 39: Renal Trauma (Clinical Features, Diagnostic Testing, Management)
- Smith and Tanagho's General Urology, 19th Ed. — Clinical Findings and Indications for Studies
- Schwartz's Principles of Surgery, 11th Ed. — Kidneys (Role of Angioembolization, Grading, Management)
This is a shared conversation. Sign in to Orris to start your own chat.