Bedside tests to predict difficult intubation
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Searching Images
3-3-2 rule airway assessment difficult intubation thyromental distance
I have all the material needed for a comprehensive answer. Let me compose it now.
Bedside Tests to Predict Difficult Intubation
Pre-intubation airway assessment is a structured physical examination aimed at identifying anatomical and physiologic features that predict difficult direct laryngoscopy (DL), videolaryngoscopy (VL), bag-mask ventilation (BMV), or extraglottic device placement. No single test is sufficiently sensitive or specific — a combination is always more predictive.
The LEMON Mnemonic (Emergency/Bedside Standard)
Used widely in emergency medicine; validated for reasonable sensitivity and high negative predictive value.
| Letter | Component | Details |
|---|---|---|
| L | Look externally | Gestalt assessment: facial trauma, large incisors, beard/mustache, large tongue, burns, obesity, short/thick neck, receding mandible |
| E | Evaluate 3-3-2 rule | See below |
| M | Mallampati score | Oropharyngeal visibility (Classes I–IV) |
| O | Obstruction/Obesity | Supraglottic obstruction, OSA, neck mass, epiglottitis |
| N | Neck mobility | Ability to assume sniffing position; cervical collar or fusion |
In the ED, Mallampati scoring often cannot be performed (~50% of patients are unable to cooperate). A modified LEMON excluding Mallampati retains good predictive value for emergency intubation. — Rosen's Emergency Medicine, 10e
Individual Bedside Tests
1. Modified Mallampati Classification (Samson & Young)
The most widely known test. Patient is seated upright, head neutral, mouth fully open, tongue protruded, no phonation.
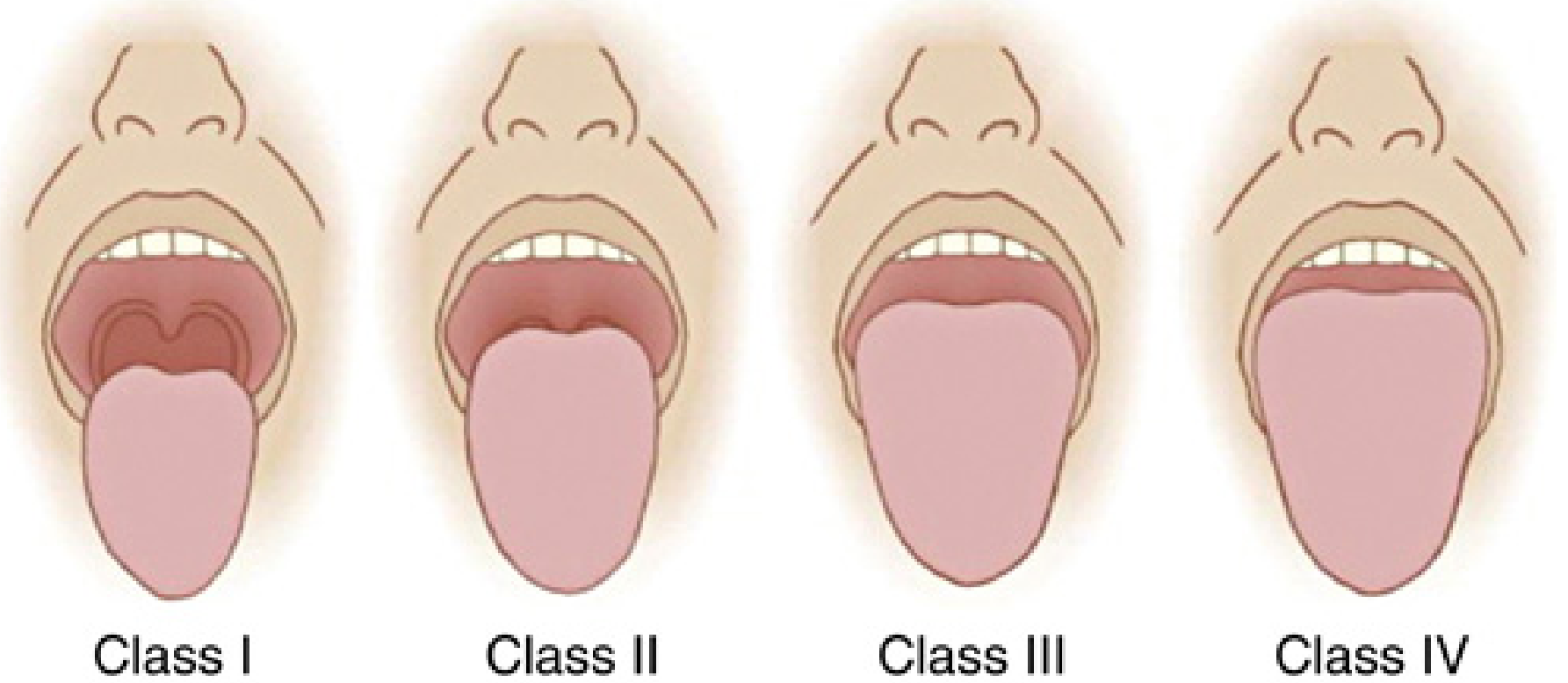
| Class | Structures Visible |
|---|---|
| I | Soft palate, fauces, uvula, tonsillar pillars |
| II | Soft palate, fauces, uvula |
| III | Soft palate, base of uvula only |
| IV | Soft palate not visible |
- Classes III–IV predict difficult DL
- Performs better as predictor of difficult laryngoscopy than of difficult intubation per se
- Predictive value improves when performed with head in full extension (Extended Mallampati Score)
- A class 0 (epiglottis visible) is usually associated with easy laryngoscopy
- Limitation: low sensitivity and PPV as a standalone test; requires cooperative, sitting patient
— Miller's Anesthesia, 10e
2. The 3-3-2 Rule (Evaluate step of LEMON)
Assesses the geometry of the oropharynx and neck for DL access:

| Measurement | Fingers | Significance |
|---|---|---|
| Inter-incisor distance (mouth opening) | ≥ 3 patient's fingers | Adequate oral access |
| Mentum to hyoid (submental space) | ≥ 3 patient's fingers | Room to displace the tongue |
| Hyoid to thyroid notch | ≥ 2 patient's fingers | Low enough larynx for DL access |
A patient with a receding mandible + high-riding larynx fails steps 2 and 3, making DL exceptionally difficult.
3. Mouth Opening (Interincisor Distance)
- Measure from upper to lower incisors at maximal mouth opening
- < 3 cm (2 fingerbreadths) → suggests possible difficult intubation
- Some studies use < 4–4.5 cm as the cutoff
- Also assess for: long upper incisors (impair blade insertion), loose/capped teeth (aspiration risk), macroglossia, high-arched palate
4. Thyromental Distance (TMD)
- Measured from the thyroid notch to the lower border of the chin, head fully extended
- < 6 cm (some sources: < 6.5 cm, or < 3 fingerbreadths) → indicates a reduced submandibular space ("anterior larynx"), predicting difficult intubation
- Reflects capacity of the submandibular space to accommodate the tongue during laryngoscopy
5. Sternomental Distance (SMD)
- Measured from the sternal notch to the point of the chin, head in full extension, mouth closed
- < 12.5 cm → associated with difficult intubation
- Indirectly assesses neck mobility and mandibular space together
6. Neck Range of Motion
- Qualitative: Can the patient assume the sniffing position (cervical flexion + atlantooccipital extension)?
- Quantitative: Angle subtended by the forehead when moving from full flexion to full extension; < 80° predicts difficult intubation
- A neck circumference > 43 cm (17 inches) is associated with difficult intubation — more predictive than BMI alone
7. Upper Lip Bite Test (ULBT)
Assessment of mandibular prognathism (jaw protrusion):
| Class | Finding |
|---|---|
| I | Lower incisors can bite the upper lip above the vermilion line |
| II | Lower incisors can bite the upper lip below the vermilion line |
| III | Lower incisors cannot reach the upper lip |
- Class III = difficult laryngoscopy
- Shown to predict difficult laryngoscopy with higher specificity and less interobserver variability than Mallampati
- Inability to extend the lower incisors beyond the upper incisors is also a similar, simpler test
8. External Visual Inspection ("Look")
Features that prompt immediate concern:
- Short, thick, or immobile neck
- Receding mandible (retrognathia)
- Large tongue / macroglossia
- Facial trauma, burns, edema
- Large or protruding upper incisors ("buck teeth")
- Beard/mustache (predicts difficult BMV from mask seal failure)
- Cervical collar, traction, or known cervical spine immobility
Multivariate Scoring Systems
Because individual tests have low standalone predictive value, multivariate tools improve accuracy:
| Score | Components |
|---|---|
| Wilson Risk Sum | Weight, head/neck movement, jaw movement, receding mandible, buck teeth |
| El-Ganzouri Risk Index | Mouth opening, TMD, Mallampati, neck movement, prognathism, weight, history of difficult intubation |
| LEMON Score | Quantified version: each feature scored 0–1; total predicts difficulty |
"Models that use several risk factors have been developed to improve predictive value of airway assessment... a computer-assisted model using BMI, mouth opening, thyromental distance, Mallampati class, and receding mandible predicted difficult intubation more accurately than simpler models." — Miller's Anesthesia, 10e
Predicting Difficult Bag-Mask Ventilation: ROMAN
Assessing BMV difficulty is equally critical (failed intubation → reliance on BMV):
| Letter | Factor |
|---|---|
| R | Resistance to ventilation (asthma, COPD, ARDS, head/neck radiation) |
| O | Obstruction, Obesity, OSA |
| M | Mallampati class III/IV, Mask seal difficulty (trauma, beard), Male sex |
| A | Age > 55 |
| N | No teeth (edentulous) |
Predicting Difficult Extraglottic Device (EGD) Placement: RODS
| Letter | Factor |
|---|---|
| R | Restricted mouth opening / Resistance to ventilation |
| O | Obstruction, Obesity, OSA |
| D | Distorted anatomy |
| S | Short thyromental distance |
Key Practical Points
- No single test is adequate alone — always use in combination
- In emergencies, a modified LEMON without Mallampati is most practical
- Mark the cricothyroid membrane (clinically or under US guidance) pre-emptively in any anticipated difficult airway
- History of a previous difficult intubation is one of the strongest independent predictors and must be elicited
- Edentulousness predicts easy intubation but difficult BMV
- The combination of Mallampati + TMD + sternomental + interincisor distance provides the best overall prediction
Sources: Miller's Anesthesia, 10e | Rosen's Emergency Medicine, 10e | Roberts & Hedges' Clinical Procedures in Emergency Medicine, 7e
This is a shared conversation. Sign in to Orris to start your own chat.