Short segment soft stricture of the bulbar urethra
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bulbar urethral stricture" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to provide a detailed, authoritative answer. Here is the full response:
Short Segment Soft Stricture of the Bulbar Urethra
Anatomy of the Bulbar Urethra
The male urethra is divided from proximal to distal into the prostatic, membranous, bulbar (bulbous), and penile segments. The bulbar urethra spans from the pelvic floor to the penoscrotal junction - it is the fixed, most proximal part of the anterior urethra. Urethral strictures are most common in this segment. (Schwartz's Principles of Surgery, 11th ed.)
Definition and Significance of "Soft" Stricture
A soft stricture refers to a narrowing caused by minimal or early fibrosis - the surrounding spongiofibrosis is limited and the scar tissue is pliable rather than densely indurated. This is an important distinction from hard/dense traumatic strictures because:
- It is more amenable to endoscopic treatment
- It carries a better prognosis with less invasive management
- The degree of spongiofibrosis is the key pathological determinant of recurrence risk
Imaging
Retrograde urethrogram (RUG) is the investigation of choice. It characterises location, length, and calibre of the stricture. Combined with voiding cystourethrogram (VCUG), the full extent can be delineated. Cystoscopy adds information about luminal diameter and density.
Below: ascending urethrogram showing stricture of the bulbar urethra (arrow, panel b) compared with a normal urethrogram (panel a):
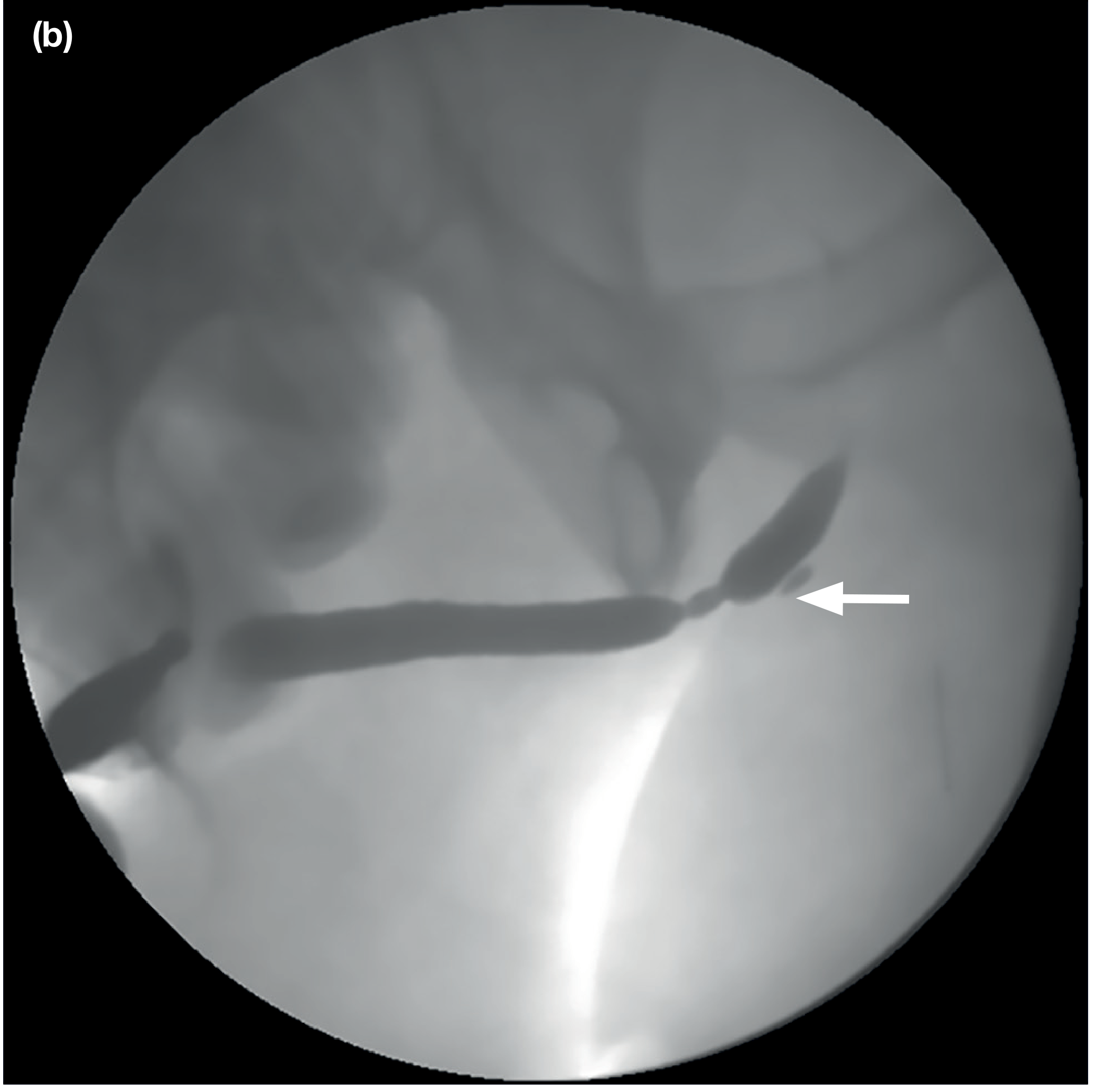
(Bailey and Love's Short Practice of Surgery, 28th ed., Fig. 85.8)
Aetiology
| Category | Examples |
|---|---|
| Iatrogenic (33%) | Prolonged catheterisation, large-bore catheters, urethroscopy, TURP resectoscope, ischemic insult during major surgery |
| Traumatic (19%) | Straddle injury to perineum (direct blunt injury to bulbar urethra - the most common site for straddle trauma) |
| Inflammatory (15%) | Lichen sclerosis, gonococcal urethritis, lichen planus |
| Idiopathic (33%) | No identifiable cause |
(Sabiston Textbook of Surgery; Schwartz's Principles of Surgery, 11th ed.)
Clinical Presentation
Patients present with lower urinary tract symptoms (LUTS):
- Weak/reduced urinary stream (most characteristic)
- Prolonged voiding, sensation of incomplete emptying
- Straining to void (Valsalva voiding)
- Urinary urgency and frequency
- Dysuria; urinary tract infections (UTIs)
- In severe cases: acute or chronic urinary retention, bladder hypertrophy, upper tract deterioration (hydronephrosis, renal impairment)
Uroflowmetry typically shows a plateau (box-shaped) flow curve, characteristic of fixed obstruction.
Management: Treatment Ladder
The approach depends on stricture length, density, and recurrence pattern. For a short (<2 cm), soft bulbar stricture specifically, the standard approach is:
1. Endoscopic Options (First-line for short, soft strictures)
a) Urethral Dilation
- Performed with filiform bougies or balloon dilators over a guidewire, progressing stepwise
- Appropriate for a soft, early stricture - gentle pressure may allow passage
- Not curative; provides temporary relief
- Suitable for patients who are poor surgical candidates or decline surgery (can be taught self-catheterisation/self-dilation with 12-14 Fr catheter)
b) Direct Vision Internal Urethrotomy (DVIU)
- Performed with an optical urethrotome (Sachse urethrotome); stricture incised under direct vision using a cold knife, typically at the 12 o'clock position
- Alternatively a holmium/thulium laser fibre can be used
- Specifically indicated for short, non-traumatic bulbar strictures - should NOT be used in the penile urethra or at the sphincter-active membranous urethra
- Success rate of a single endoscopic attempt: ~30%; drops to ~13% for repeat attempts
- Recurrent dilations risk worsening spongiofibrosis and making subsequent reconstruction more complex
- Common practice: attempt one endoscopic intervention before referral for urethroplasty
(Bailey and Love's, 28th ed.; Schwartz's Principles of Surgery; Sabiston)
2. Urethroplasty (Definitive/Gold Standard)
Indications for urethroplasty include:
- Bulbar strictures >2 cm in length
- Bulbar strictures <2 cm that recur after endoscopic management
- Any primary soft stricture in a patient preferring definitive treatment upfront
For short segment bulbar strictures specifically, urethroplasty type depends on cause:
a) Excision and Primary Anastomosis (EPA) - Anastomotic Urethroplasty
The gold standard for short (<2 cm) bulbar urethral strictures, especially traumatic ones with a gap. This is the procedure of choice for short soft strictures that have failed endoscopic management.
Technique (Hinman's Atlas / Campbell-Walsh):
- Perineal incision; bulbocavernosus muscles split in midline (or one-sided dissection if stricture is distal to the muscles - releasing the ischiocavernosus on one side to access the dorsal urethra without dividing bulbocavernosus)
- The strictured segment is excised completely between vascular clamps using a fresh scalpel - full-thickness excision of corpus spongiosum
- Distal stump: spatulated dorsally, calibrated to ≥26 Fr
- Proximal stump: spatulated ventrally, calibrated to ≥28 Fr
- Because the bulbar urethra is eccentrically positioned within the corpus spongiosum: dorsal anastomotic sutures are full-thickness; ventral sutures through urethra only
- 8-12 interrupted sutures of 4-0 or 5-0 PDS or polyglactin placed 2-3 mm apart
- Spongioplasty: preserving the most proximal corpus spongiosum protects lateral bulbar arteries, ensures blood supply, and aids haemostasis
- Success rate for EPA: >90% at long-term follow-up
(Hinman's Atlas of Urologic Surgery, Chapter 94; Sabiston Textbook of Surgery)
b) Augmentation Urethroplasty (for non-traumatic / longer strictures)
- The strictured segment is incised (not excised) and widened with a free graft patch - oral mucosal graft (OMG), either buccal (cheek) or lingual (ventral tongue)
- OMG is the gold standard tissue substitute: hairless, moist, easy to harvest, good take
- Can be placed dorsally (Barbagli technique - quilted to corpora), ventrally, or laterally
- Reserved for strictures where primary anastomosis would have tension (i.e., longer segments), or non-traumatic soft strictures
- Hair-bearing skin must never be used (risk of stone formation and UTI)
(Sabiston; Schwartz's Principles of Surgery, 11th ed.)
Decision Summary for Short Segment Soft Bulbar Stricture
Short segment (<2 cm), soft, bulbar urethra stricture
|
v
First attempt: DVIU (cold knife/laser) OR dilation
|
Success (~30%) --> Surveillance, consider self-dilation to maintain
|
Recurrence --> Urethroplasty (do NOT keep repeating DVIU)
|
v
Urethroplasty type:
- Traumatic/gap present --> Excision + Primary Anastomosis (EPA)
- Non-traumatic, soft, no gap --> Augmentation with oral mucosal graft
- EPA also applicable if short enough that tension-free anastomosis is possible
Key Points
- The bulbar urethra is the most common site for urethral stricture
- "Soft" implies minimal spongiofibrosis - more favorable for endoscopic treatment compared with dense/traumatic strictures
- One endoscopic attempt (DVIU) is appropriate first-line; success ~30%
- After recurrence, urethroplasty is the definitive treatment - do not repeatedly instrument as this worsens fibrosis
- For short bulbar strictures: EPA (excision and primary anastomosis) gives >90% long-term success
- Use RUG to characterise length/location; cystoscopy to assess density
Sources:
- Sabiston Textbook of Surgery, Biological Basis of Modern Surgical Practice
- Schwartz's Principles of Surgery, 11th Edition
- Bailey and Love's Short Practice of Surgery, 28th Edition
- Hinman's Atlas of Urologic Surgery (E-Book)
- Campbell-Walsh-Wein Urology, 3-Volume Set
- Recent meta-analysis: Oszczudlowski et al., "Outcomes of transecting versus non-transecting urethroplasty for bulbar urethral stricture," BJU Int. 2023 Sep [PMID: 37402622]
Short segment soft stricture of the bulbar urethra
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bulbar urethral stricture" AND urethroplasty
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the source material needed for a comprehensive answer. Here is the full response:
Short Segment Soft Stricture of the Bulbar Urethra
Anatomy
The male urethra is divided (distal to proximal) into: urethral meatus → fossa navicularis → pendulous (penile) urethra → bulbar urethra → membranous urethra → prostatic urethra. The bulbar urethra is the fixed segment between the pelvic floor and the penoscrotal junction - it is the most proximal part of the anterior urethra and the most common site for urethral stricture disease. (Schwartz's Principles of Surgery, 11th ed.; Sabiston Textbook of Surgery)
Pathology
A urethral stricture is a fibrotic narrowing composed of dense collagen and fibroblasts. In most cases, fibrosis extends into the surrounding corpus spongiosum causing spongiofibrosis - the extent and density of this spongiofibrosis is the most important prognostic factor determining treatment choice and recurrence risk.
A "soft" stricture specifically means:
- Minimal or early-stage spongiofibrosis
- The surrounding tissue is pliable, not indurated
- The narrowing can often be traversed or dilated more easily than a dense/traumatic stricture
- This is the most favorable type for both endoscopic and reconstructive management
Fibrosis restricts urine flow, causing proximal urethral dilation and prostatic duct dilation. Secondary complications include: prostatitis, bladder hypertrophy, increased post-void residual, urinary stasis, recurrent UTIs, and in severe/chronic cases - decompensation of the ureterovesical junction, reflux, hydronephrosis, and renal failure. (Smith and Tanagho's General Urology, 19th ed.)
Aetiology
| Category | Proportion | Examples |
|---|---|---|
| Iatrogenic | ~33% | Urethral catheterisation (especially prolonged or large-bore), cystoscopy/urethroscopy, TURP resectoscope, pelvic surgery with ischaemic insult |
| Idiopathic | ~33% | No identifiable cause |
| Traumatic | ~19% | Straddle injury - direct perineal blunt trauma is the classic cause of bulbar stricture |
| Inflammatory | ~15% | Lichen sclerosus, gonococcal urethritis, other infective urethritis |
| Other | rare | Radiation, malignancy (consider if recurrent or atypical) |
(Sabiston Textbook of Surgery; Schwartz's Principles of Surgery, 11th ed.)
Clinical Features
Symptoms:
- Weak, reduced urinary stream (most common presenting complaint)
- Spraying or split/double urinary stream
- Prolonged voiding, sensation of incomplete emptying
- Post-void dribbling
- Need for Valsalva or suprapubic pressure to void
- Urinary frequency and mild dysuria
- Chronic urethral discharge (suggests associated prostatitis)
- Urinary tract infections
- Acute urinary retention (less common unless infection or prostatic obstruction co-exists)
Signs:
- Induration palpable along the course of the urethra at the stricture site
- Tender perineal mass = periurethral abscess
- Urethrocutaneous fistula in chronic severe cases
- Palpable bladder in chronic retention
Uroflowmetry: Classic plateau (box-shaped) flow curve - a flat, low-amplitude trace indicating fixed urethral obstruction. Peak flow rate typically <10 mL/s (normal >20 mL/s). (Smith and Tanagho's General Urology, 19th ed.)
Investigations
| Investigation | Purpose |
|---|---|
| Retrograde urethrogram (RUG) | Gold standard for location and length of stricture |
| Voiding cystourethrogram (VCUG) | Delineates proximal extent; assesses bladder |
| Uroflowmetry | Objective assessment of obstruction severity |
| Flexible cystoscopy / urethroscopy | Directly visualises stricture; assesses luminal diameter and density/softness |
| Sonourethrography | Useful adjunct; detects extent of spongiofibrosis |
| Urine culture | Identifies concurrent UTI |
| Post-void residual | Quantifies bladder emptying impairment |
The location and length are best characterised by fluoroscopic RUG; the diameter and density (soft vs hard) are best characterised by direct cystoscopic visualisation. (Sabiston Textbook of Surgery)
Imaging example - ascending urethrogram showing a stricture in the bulbar urethra (arrow):
Endoscopic appearance of a urethral stricture:
Treatment
The management strategy depends on stricture length, softness/density, location, and whether it is a primary or recurrent stricture. Available options for stricture treatment are determined by these four factors. (Sabiston Textbook of Surgery)
1. Urethral Dilation
- One of the oldest urological procedures (5000-year history)
- Performed over a guidewire using serial plastic dilators (modern technique)
- Particularly effective for soft and short strictures - this is exactly the scenario where dilation is most appropriate as a first-line measure
- Also indicated for: unfit patients, patients refusing urethroplasty, multiple failed urethroplasties
- Mechanism: fractures scar tissue and temporarily enlarges the lumen; as healing occurs, scar tissue re-forms
- Rarely curative - most patients require repeated dilations
- Complications: pain, fever, bleeding, false passage creation
Self-dilation (clean intermittent catheterisation): patient inserts a small-calibre (12-14 Fr) disposable catheter at regular intervals. Not curative but maintains lumen patency. Suitable for patients unwilling to undergo urethroplasty. (Bailey and Love's Short Practice of Surgery, 28th ed.; Smith and Tanagho's General Urology, 19th ed.)
2. Direct Vision Internal Urethrotomy (DVIU)
- Performed with an optical urethrotome (Sachse type)
- The stricture is incised under direct visual control using a cold knife passed through the sheath; alternatively, a holmium or thulium laser fibre can be used
- A guidewire passed through the stricture serves as a guide to avoid false passage
- Specifically indicated for short, non-traumatic bulbar strictures - this is the archetypal indication
- NOT appropriate for: penile urethral strictures, sphincter-active membranous urethra (risk of incontinence)
- Short-term success: 70-80%; long-term success rate is much lower
- Single DVIU success rate: approximately 30%
- Repeat DVIU success rate drops to approximately 13%
- Advantages: minimal anaesthesia required (topical + sedation in many cases), easily repeated, very safe with few complications, more precise than blind dilation (Smith and Tanagho's; Bailey and Love's)
Key principle: Repeated instrumentation (repeated DVIU or dilation) worsens spongiofibrosis and makes subsequent reconstructive surgery more complex. The standard approach is one endoscopic attempt, then proceed to urethroplasty on recurrence.
3. Urethroplasty (Gold Standard / Definitive Treatment)
Indications for urethroplasty:
- Bulbar urethral strictures >2 cm in length (primary)
- Bulbar strictures <2 cm that recur after endoscopic management
- Any primary penile urethral stricture
- Meatal/fossa navicularis strictures recurrent after endoscopic management
- Patients not suitable for repeat endoscopy
For short segment soft bulbar strictures, the key choice is between:
A. Excision and Primary Anastomosis (EPA) - The Procedure of Choice for Short Bulbar Strictures
This is the definitive procedure specifically for short (≤2 cm) bulbar urethral strictures.
- The entire strictured segment is completely excised - the excision extends 1 cm beyond each end of the stricture to ensure removal of all spongiofibrosis and improve postoperative healing
- The two healthy urethral ends are directly anastomosed with wide spatulation
- Performed via a perineal incision
- The distal stump is spatulated dorsally, the proximal stump ventrally
- Because the bulbar urethra is eccentrically positioned within the corpus spongiosum: dorsal anastomotic sutures are placed full-thickness; ventral sutures through the urethra only
- 8-12 interrupted 4-0 or 5-0 absorbable sutures (PDS or polyglactin) placed 2-3 mm apart
- Spongioplasty: preserving the most proximal corpus spongiosum protects the lateral bulbar arteries and ensures adequate blood supply across the repair
- Long-term success rate: >90%
(Smith and Tanagho's General Urology, 19th ed.; Sabiston Textbook of Surgery)
"Short strictures (≤2 cm) of the bulbar urethra should be completely excised and primary anastomosis done. If possible, the segment to be excised should extend 1 cm beyond each end of the stricture to allow for removal of any existing spongiofibrosis and improve postoperative healing." - Smith and Tanagho's General Urology
B. Augmentation (Patch Graft) Urethroplasty - For Strictures >2 cm or Where Tension-Free Anastomosis is Not Possible
- The strictured segment is incised (not excised) longitudinally and widened with a free tissue graft patch
- Oral mucosal graft (OMG) - buccal (cheek) or lingual (ventral tongue) mucosa is the gold standard tissue substitute: hairless, well-vascularised, moist epithelium with excellent take rate
- Graft can be placed dorsally (Barbagli technique - quilted to corpora cavernosa) or ventrally; in the bulbar urethra, dorsal or ventral onlay both acceptable
- The urethra is incised for the full stricture length plus 0.5 cm proximal and distal; graft is tailored, all subcutaneous tissue removed, and meticulously sutured into place
- Critical: hair-bearing skin must never be used (risk of intraluminal hair - nidus for stone formation and recurrent UTI)
- For very long, densely fibrotic strictures: penile fasciocutaneous flap (e.g., McAninch flap) - success in >80% of cases; can be combined with buccal mucosa graft in pan-urethral stricture
(Smith and Tanagho's General Urology, 19th ed.; Sabiston Textbook of Surgery)
C. Two-Stage Urethroplasty (Johanson Procedure)
Reserved for complex cases: densely fibrotic strictures, failed multiple urethroplasties, lichen sclerosus affecting the urethra, or when a single-stage repair is not feasible. Seldom required for a short soft bulbar stricture.
Treatment Decision Summary
Short segment (≤2 cm), SOFT, bulbar urethral stricture
│
▼
First-line: Dilation OR DVIU (cold knife / laser)
[DVIU is specifically indicated for short, non-traumatic bulbar strictures]
│
┌───────┴────────┐
│ │
Success Recurrence
(~30%) (~70%)
│ │
Surveillance ──► URETHROPLASTY
± self-dilation │
▼
Excision + Primary Anastomosis (EPA)
[procedure of choice for short ≤2 cm bulbar strictures]
Success rate: >90%
│
If length > 2 cm OR tension-free anastomosis not possible:
▼
Augmentation urethroplasty with oral mucosal graft (OMG)
Complications of Untreated Stricture
- Chronic prostatitis (very common)
- Recurrent UTIs, cystitis
- Bladder hypertrophy and trabeculation
- Periurethral abscess
- Urethrocutaneous fistula
- Vesical calculi (urinary stasis)
- Upper tract deterioration: hydronephrosis, renal failure (severe/chronic cases)
Recent Evidence
- Oszczudlowski et al., BJU Int 2023 [PMID: 37402622] - Meta-analysis comparing transecting (excision with anastomosis) vs non-transecting urethroplasty for bulbar stricture: both approaches showed high success rates with comparable outcomes, supporting the continued role of EPA for short bulbar strictures
- Barratt et al., Eur Urol 2021 [PMID: 33875306] - Systematic review of free graft augmentation urethroplasty techniques for bulbar strictures, confirming oral mucosal graft as the tissue of choice
Sources:
- Smith and Tanagho's General Urology, 19th Edition
- Sabiston Textbook of Surgery, The Biological Basis of Modern Surgical Practice
- Schwartz's Principles of Surgery, 11th Edition
- Bailey and Love's Short Practice of Surgery, 28th Edition
- Campbell-Walsh-Wein Urology, 3-Volume Set
This is a shared conversation. Sign in to Orris to start your own chat.