Gastrointestinal bleeding classification
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive material to construct a thorough answer on GI bleeding classification. Let me compile it.
Gastrointestinal Bleeding: Classification
1. Classification by Acuity
| Type | Definition |
|---|---|
| Overt (acute) | Clinically apparent blood loss — hematemesis, melena, or hematochezia |
| Occult | Slow, low-volume loss not visible to the patient; detectable only by fecal occult blood testing; may cause iron deficiency anemia |
| Obscure | Recurrent bleeding with no source identified on upper and lower endoscopy; requires capsule endoscopy, CT enterography, or enteroscopy to identify a small bowel source |
— Goldman-Cecil Medicine, p. 1374
2. Classification by Anatomical Location
The ligament of Treitz (distal duodenum) divides GI bleeding into upper and lower, with a third category — small bowel (mid-GI) — now recognized separately.
Upper GI Bleeding (UGIB)
Source is proximal to the ligament of Treitz. UGIB is approximately 3× more common than LGIB.
Presentation: Hematemesis (red blood or coffee-ground emesis), melena. Hematochezia can occur with massive UGIB.
Causes:
- Peptic ulcer disease (excess gastric acid, H. pylori, NSAIDs, physiologic stress) — most common
- Esophagitis
- Gastritis and duodenitis
- Esophagogastric varices
- Portal hypertensive gastropathy
- Angiodysplasia / vascular ectasias
- Dieulafoy lesion (dilated submucosal artery eroding through epithelium without primary ulceration)
- Gastric antral vascular ectasia (GAVE/"watermelon stomach")
- Mallory-Weiss tears
- Cameron lesions (ulcers at a hiatal hernia)
- Aortoenteric fistulas
- Upper GI tumors
- Hemobilia (bleeding from the biliary tract)
- Hemosuccus pancreaticus (bleeding from the pancreatic duct)
- Postsurgical bleeds (anastomotic, post-polypectomy, post-sphincterotomy)
Lower GI Bleeding (LGIB)
Source is distal to the ligament of Treitz; ~95% arises from the colon, ~5% from the small intestine.
Presentation: Hematochezia (bright red or maroon blood per rectum). ~80–90% of hematochezia is from a lower source; massive UGIB can also cause hematochezia.
Causes:
- Diverticulosis — accounts for 60% of LGIB in patients >50 years
- Angiodysplasia
- Infectious colitis
- Ischemic colitis
- Inflammatory bowel disease
- Colorectal cancer
- Hemorrhoids
- Anal fissures
- Rectal varices
- Radiation-induced damage
- Postsurgical (post-polypectomy, post-biopsy)
In patients <50 years, IBD, hemorrhoids, and infectious colitis predominate; however, colonic neoplasia is increasingly seen in the 40–50 age group.
Small Bowel (Mid-GI) Bleeding
Accounts for approximately 5% of all GI bleeding. Sources include vascular ectasias, ulcers (NSAIDs, Crohn's), and neoplasms.
— Sabiston Textbook of Surgery, pp. 2183–2185; Goldman-Cecil Medicine, p. 1374
3. Endoscopic Classification — Forrest Classification (for Peptic Ulcer Bleeding)
Used in Europe, the UK, Asia, and internationally to stratify the risk of rebleeding from peptic ulcers. Interobserver agreement is only fair-to-moderate for some categories.
| Class | Description | Risk of Rebleeding (no treatment) |
|---|---|---|
| Ia | Spurting (active arterial) hemorrhage | ~90% |
| Ib | Oozing hemorrhage | ~10–27% |
| IIa | Non-bleeding visible vessel (NBVV) | ~50% |
| IIb | Adherent clot | ~33% |
| IIc | Flat pigmented spot | ~7–10% |
| III | Clean-based ulcer | ~3–5% |
High-risk stigmata (classes Ia, Ib, IIa, IIb) — benefit from endoscopic hemostasis.
Low-risk stigmata (classes IIc, III) — do not require endoscopic therapy.
A translucent NBVV carries a higher rebleeding risk than a darkly pigmented protuberance because it likely represents exposed arterial wall rather than a clot.
— Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1580; Yamada's Textbook of Gastroenterology; Sabiston Textbook of Surgery, p. 2186
4. Clinical Severity / Risk Stratification Scores
Rockall Score (Nonvariceal UGIB)
A pre- and post-endoscopy scoring system predicting rebleeding and mortality. Maximum score = 11.
| Variable | Score 0 | Score 1 | Score 2 | Score 3 |
|---|---|---|---|---|
| Age | <60 yr | 60–79 yr | ≥80 yr | — |
| Shock | None | HR >100 bpm | SBP <100 mmHg | — |
| Comorbidity | None | — | CHF, IHD, other major illness | Renal failure, liver failure, metastatic cancer |
| Endoscopic diagnosis | Mallory-Weiss / no lesion | Peptic ulcer, esophagitis, erosions | UGI malignancy | — |
| Stigmata of hemorrhage | Clean base / flat spot | — | Blood in tract, active bleeding, visible vessel, adherent clot | — |
- Clinical Rockall score = 0 (pre-endoscopy: age, shock, comorbidity only) → low risk; consider outpatient management
- Complete Rockall score ≤ 2 → low risk of rebleeding
Glasgow-Blatchford Score (GBS)
A pre-endoscopy triage tool; incorporates BUN, hemoglobin, SBP, heart rate, presence of melena, syncope, hepatic disease, and cardiac failure.
- Score of 0 identifies patients safe for outpatient management
- Higher scores predict need for intervention (transfusion, endoscopy, surgery)
— Yamada's Textbook of Gastroenterology, p. 780; Goldman-Cecil Medicine
5. Classification by Clinical Presentation
| Presentation | Likely Source |
|---|---|
| Hematemesis (red blood or coffee-ground) | Proximal to ligament of Treitz |
| Melena (black, tarry stool) | Usually proximal (upper GI or small bowel); requires as little as 50 mL blood |
| Hematochezia (bright red/maroon rectal blood) | Usually distal colon; massive UGIB if accompanied by hemodynamic instability |
Blood clots in stool make an upper GI source less likely (LR 0.05), whereas melenic stool on examination makes it more likely (LR 25).
— Sabiston Textbook of Surgery, p. 2183
Management Algorithm
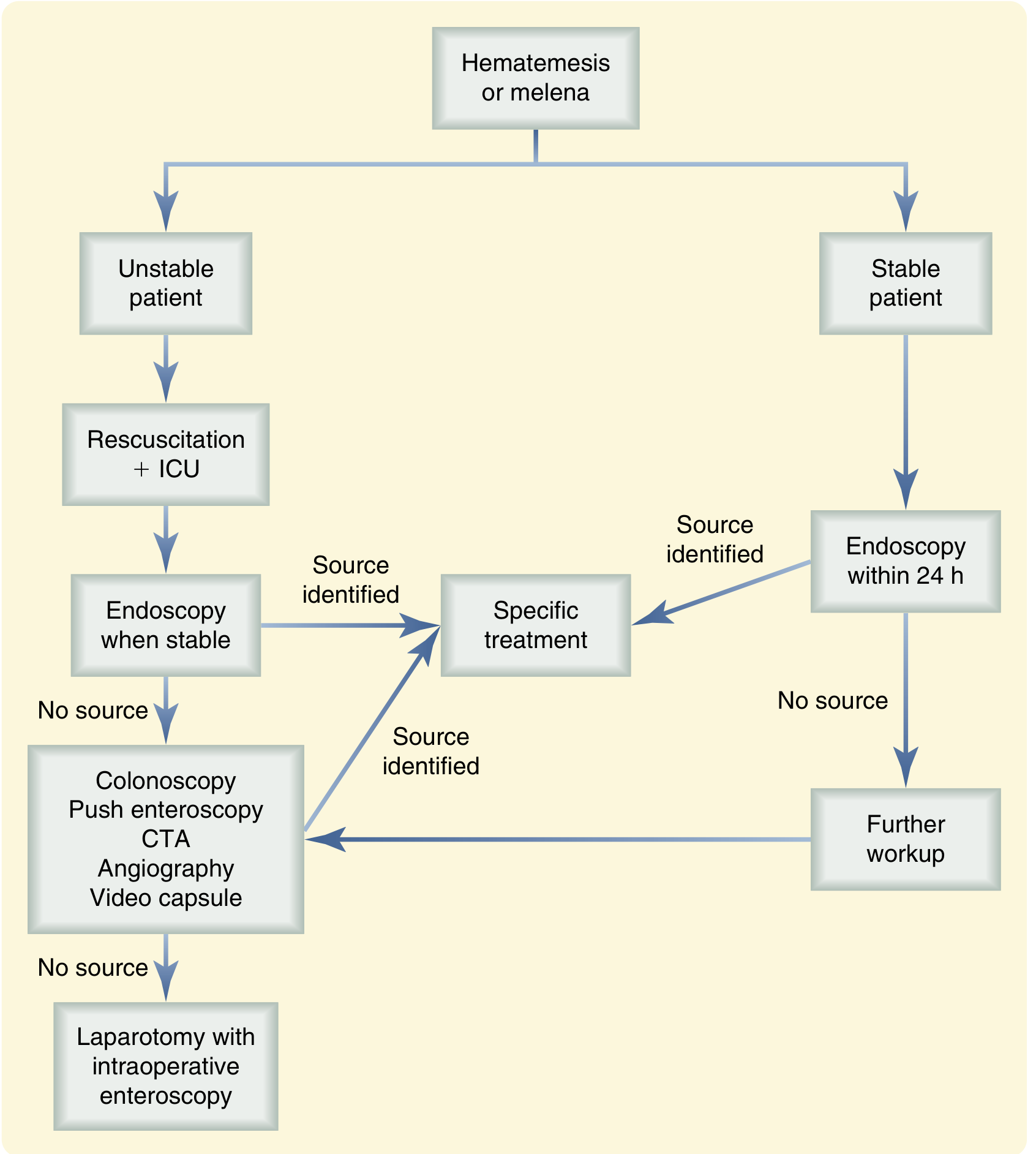
Diagnostic and management algorithm for hematemesis or melena — Sabiston Textbook of Surgery
Summary
| Classification Dimension | Categories |
|---|---|
| Acuity | Overt / Occult / Obscure |
| Location | Upper GI / Small bowel (mid-GI) / Lower GI |
| Endoscopic appearance (ulcer) | Forrest Ia → III |
| Risk stratification | Rockall Score / Glasgow-Blatchford Score |
| Hemodynamic severity | Class I (<15% volume loss) → Class IV (>40% volume loss) |
This is a shared conversation. Sign in to Orris to start your own chat.