Non steroidal contraceptive
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I have comprehensive content. Now I'll compile the full, detailed answer on non-steroidal (non-hormonal) contraceptives.
Non-Steroidal (Non-Hormonal) Contraceptives
Non-steroidal contraceptives are methods that prevent pregnancy without using synthetic steroids (estrogens or progestins). They fall into several categories: barrier methods, intrauterine devices (copper-based), spermicides, fertility awareness-based methods (FABMs), and surgical sterilization.
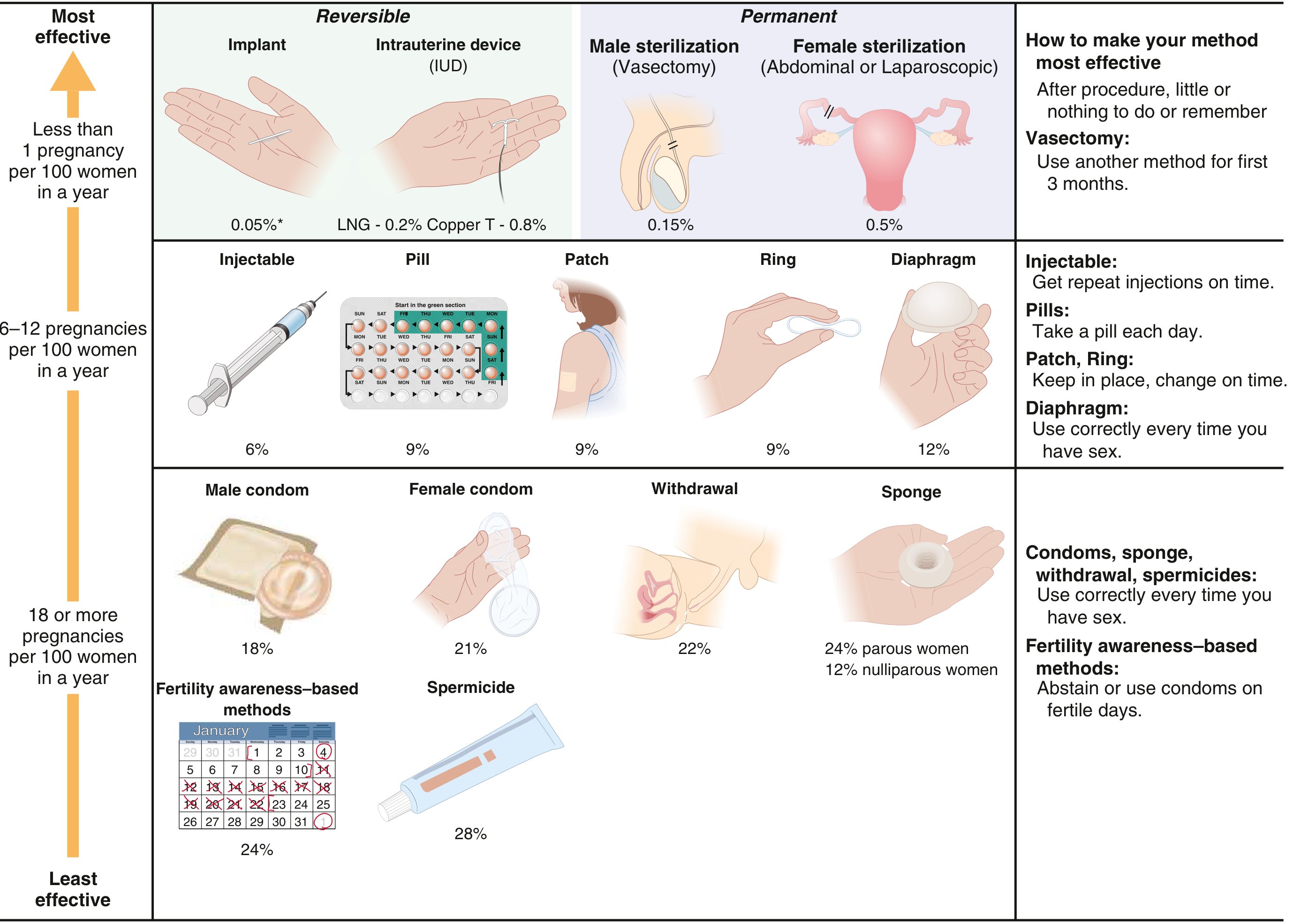
Figure: Effectiveness of contraceptive methods - Goldman-Cecil Medicine, 22e
1. Copper Intrauterine Device (Cu-IUD)
The copper T380A IUD (Paragard) is the most effective non-hormonal reversible contraceptive available.
Mechanism of action:
- Creates a local inflammatory/foreign body reaction in the uterus that is toxic to sperm
- Copper ions exert a direct spermatocidal effect, impairing sperm motility and function
- Alters uterine and tubal fluid, impeding sperm transport
- May impair fertilization and implantation
Efficacy:
- Failure rate: ~0.8% typical use (as low as 0.6% perfect use)
- Cumulative 10-year pregnancy rate: ~1.7%
- Also the most effective form of emergency contraception if inserted within 120 hours of unprotected intercourse
Duration: Approved for up to 10-12 years (some evidence supports 12+ years)
Advantages:
- Immediately reversible (fertility returns promptly after removal)
- No hormonal side effects
- Suitable for women with contraindications to estrogen (e.g., migraine with aura, thrombophilia, cardiovascular disease)
Disadvantages/Side effects:
-
Increased menstrual bleeding and dysmenorrhea
-
Risk of insertion-related complications: uterine perforation, expulsion, infection (highest in first month post-insertion, especially in women exposed to STIs)
-
Contraindicated in unexplained uterine bleeding, uterine anomalies, active pelvic inflammatory disease
-
Ganong's Review of Medical Physiology, 26e, p. 415
-
Goldman-Cecil Medicine, 22e, Chapter 220
2. Barrier Methods
Barrier methods physically prevent sperm from reaching the ovum. They are used at the time of coitus and have higher failure rates than long-acting methods.
Male Condom (External Condom)
- One of the oldest known contraceptives; made of latex or polyurethane
- Typical use failure rate: ~18% per year
- Perfect use failure rate: ~2% (Ganong's: 3.6 failures per 100 woman-years)
- Only contraceptive method that also protects against STIs including HIV
- Polyurethane condoms are suitable for latex allergy and are less likely to rupture
- Easy to use, widely available, no prescription required
Female Condom (Internal Condom)
- Soft, loose-fitting polyurethane pouch with two flexible rings
- The inner (smaller) ring is inserted into the vagina; the outer (larger) ring remains outside
- Typical use failure rate: ~21%
- Can be inserted before sexual activity
- Less likely to rupture than latex male condoms
- Protects against HIV and STIs (both polyurethane and latex prevent viral transmission)
Diaphragm
- A soft latex or silicone dome inserted to cover the cervix before intercourse, used with spermicide
- Typical use failure rate: ~12% (Ganong's: 1.9 per 100 woman-years)
- Must remain in place for at least 6 hours after intercourse
- Requires fitting by a clinician
- Reusable; does not protect against STIs
- Risk: increased urinary tract infections; contraindicated with allergy to latex/spermicide
Cervical Cap and Sponge
-
Cervical cap: fits over the cervix; used with spermicide; less effective in parous women
-
Contraceptive sponge: soft foam device containing spermicide; inserted before intercourse
- Failure rate: 24% in parous women, 12% in nulliparous women (typical use)
-
Goldman-Cecil Medicine, 22e, Chapter 220
-
Kaplan & Sadock's Comprehensive Textbook of Psychiatry, Table 30.1-6
3. Spermicides
Spermicides are chemical agents that kill or immobilize sperm. They are available as gels, creams, foams, suppositories, and films.
Mechanism: Most contain nonoxynol-9, a surfactant that disrupts the sperm cell membrane
Efficacy:
- Typical use failure rate: ~28% (highest among all standard contraceptive methods)
- Ganong's: 11.9 per 100 woman-years
- More effective when combined with a barrier method (condom or diaphragm)
Phexxi (vaginal pH modulator - newer non-hormonal option):
-
A newer FDA-approved contraceptive vaginal gel containing L-lactic acid, citric acid, and potassium bitartrate
-
Mechanism: maintains a low, spermicidal vaginal pH to inactivate sperm (sperm require an alkaline environment to survive)
-
Associated with a 7-cycle pregnancy rate of ~18% in clinical trials (typical use)
-
Used on-demand, applied immediately before each act of intercourse
-
Provides an alternative for women who cannot use or prefer to avoid nonoxynol-9
-
Goldman-Cecil Medicine, 22e (Spermicides section)
4. Fertility Awareness-Based Methods (FABMs)
These methods involve identifying and avoiding the fertile window of the menstrual cycle. No devices or chemicals are used.
Types:
- Calendar/rhythm method: Predicts fertile days based on past cycle length history
- Basal body temperature (BBT) method: Temperature rises ~0.2-0.5°C after ovulation (progesterone effect)
- Cervical mucus (Billings ovulation) method: Monitors changes in cervical secretions (thin, clear, stretchy "egg-white" mucus indicates ovulation)
- Symptothermal method: Combines BBT + cervical mucus monitoring (most reliable FABM)
- Standard Days Method (SDM): Avoids intercourse on days 8-19 of a 26-32 day cycle
- Lactational Amenorrhea Method (LAM): Exclusive breastfeeding suppresses ovulation; highly effective for the first 6 months postpartum if the woman is amenorrheic and exclusively breastfeeding (>98% effective under these conditions)
Efficacy (typical use):
- Rhythm method: ~24% failure rate per year
- Ganong's: 15.5 per 100 woman-years
- Symptothermal method (perfect use): ~0.4-2% failure rate
Limitations: Requires regular cycles, education, consistent tracking, and partner cooperation. Higher failure rates with irregular cycles.
- Pfenninger and Fowler's Procedures for Primary Care, 3e
- Ganong's Review of Medical Physiology, 26e
5. Surgical Sterilization (Permanent Methods)
Though surgical, these are inherently non-steroidal.
| Method | Typical Use Failure Rate |
|---|---|
| Vasectomy (male) | 0.15% |
| Tubal ligation/occlusion (female) | 0.5% |
-
Vasectomy: occlusion or excision of the vas deferens; outpatient procedure; requires backup contraception for first 3 months until azoospermia confirmed
-
Female sterilization: tubal ligation, fulguration, salpingectomy, or mechanical occlusion (clips/rings); laparoscopic or hysteroscopic approaches
-
Cumulative failure: 1.31% at 5 years, 1.85% at 10 years (varies by technique; segmental resection has lowest rates)
-
Goldman-Cecil Medicine, 22e
-
Ganong's Review of Medical Physiology, 26e
6. Withdrawal (Coitus Interruptus)
- Man withdraws before ejaculation
- Typical use failure rate: ~22% (Ganong's: 6.7 per 100 woman-years)
- No side effects or devices needed
- Effectiveness is highly user-dependent; pre-ejaculatory fluid may contain sperm
Comparative Efficacy Summary
| Method | Typical Use (pregnancies/100 women/year) |
|---|---|
| Copper IUD | 0.8% |
| Female sterilization | 0.5% |
| Vasectomy | 0.15% |
| Diaphragm + spermicide | 12% |
| Male condom | 18% |
| Female condom | 21% |
| Withdrawal | 22% |
| Fertility awareness methods | 24% |
| Spermicide alone | 28% |
Key Points
- Non-hormonal contraceptives are preferred in women with contraindications to estrogen or progestins (e.g., thrombophilia, cardiovascular disease, estrogen-sensitive tumors, migraine with aura, breastfeeding)
- The copper IUD is the most effective non-hormonal reversible contraceptive and doubles as emergency contraception
- Condoms are the only method offering dual protection against both pregnancy and STIs
- Spermicide alone has the highest typical use failure rate and should ideally be combined with a barrier method
- Phexxi (L-lactic acid/citric acid/potassium bitartrate gel) is a new FDA-approved on-demand non-hormonal option
- The CDC Medical Eligibility Criteria (MEC) provides evidence-based guidance on contraceptive use for women with specific medical conditions (CDC MEC Guidelines)
This is a shared conversation. Sign in to Orris to start your own chat.