Wernickes aphasia
Reading File
Finding Sources
Finding Sources
Searching Images
Wernicke's aphasia brain lesion temporal lobe
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of Wernicke's aphasia drawn from multiple neurology textbooks:
Wernicke's Aphasia
Definition & Overview
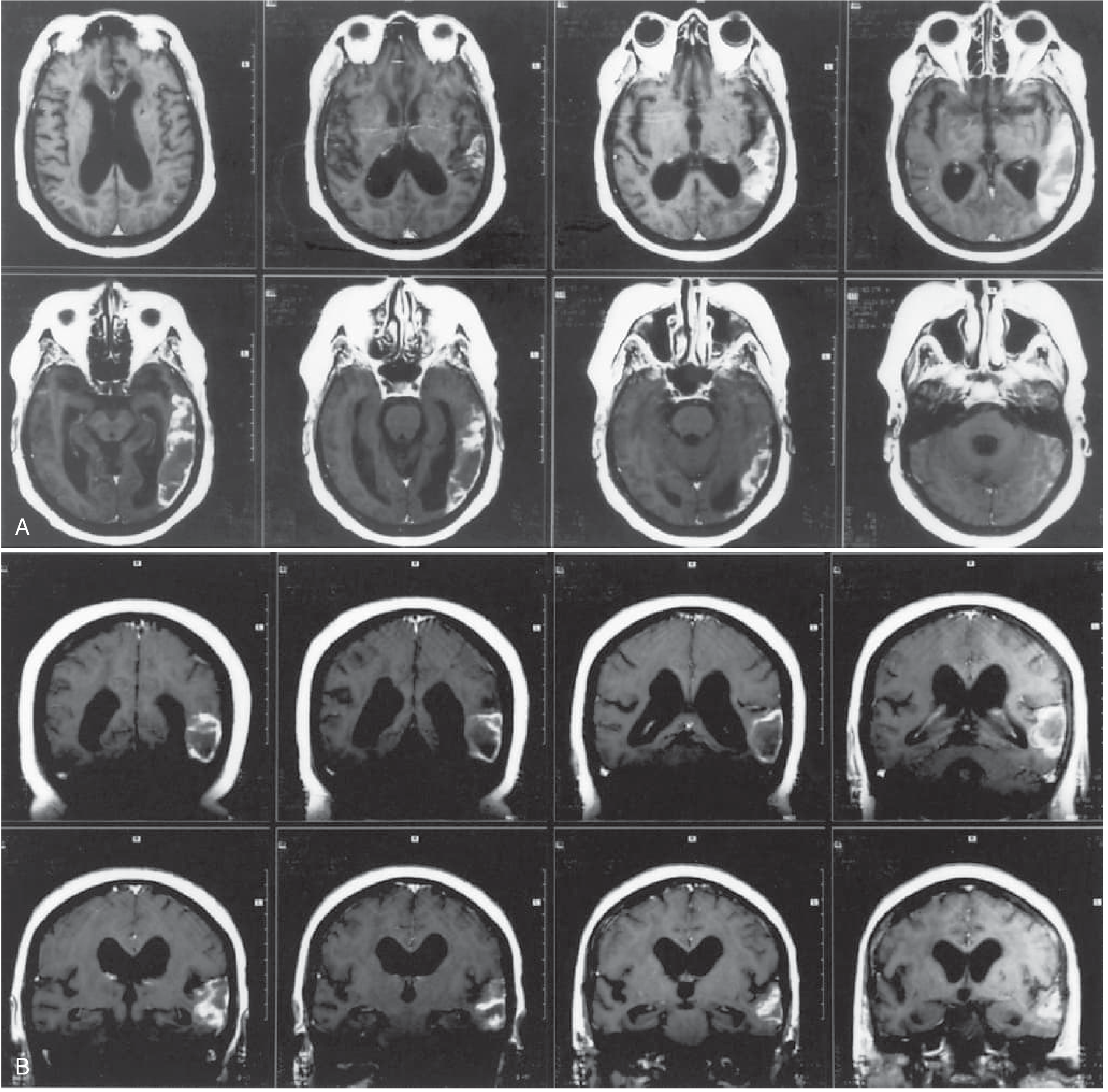
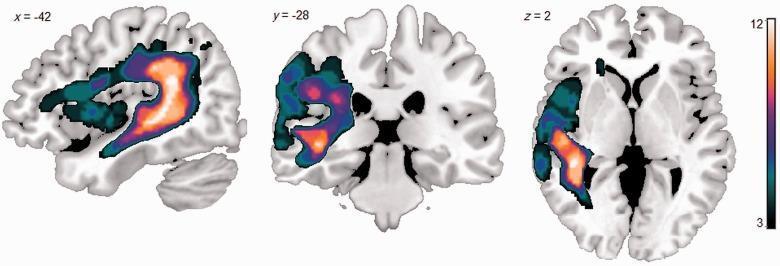
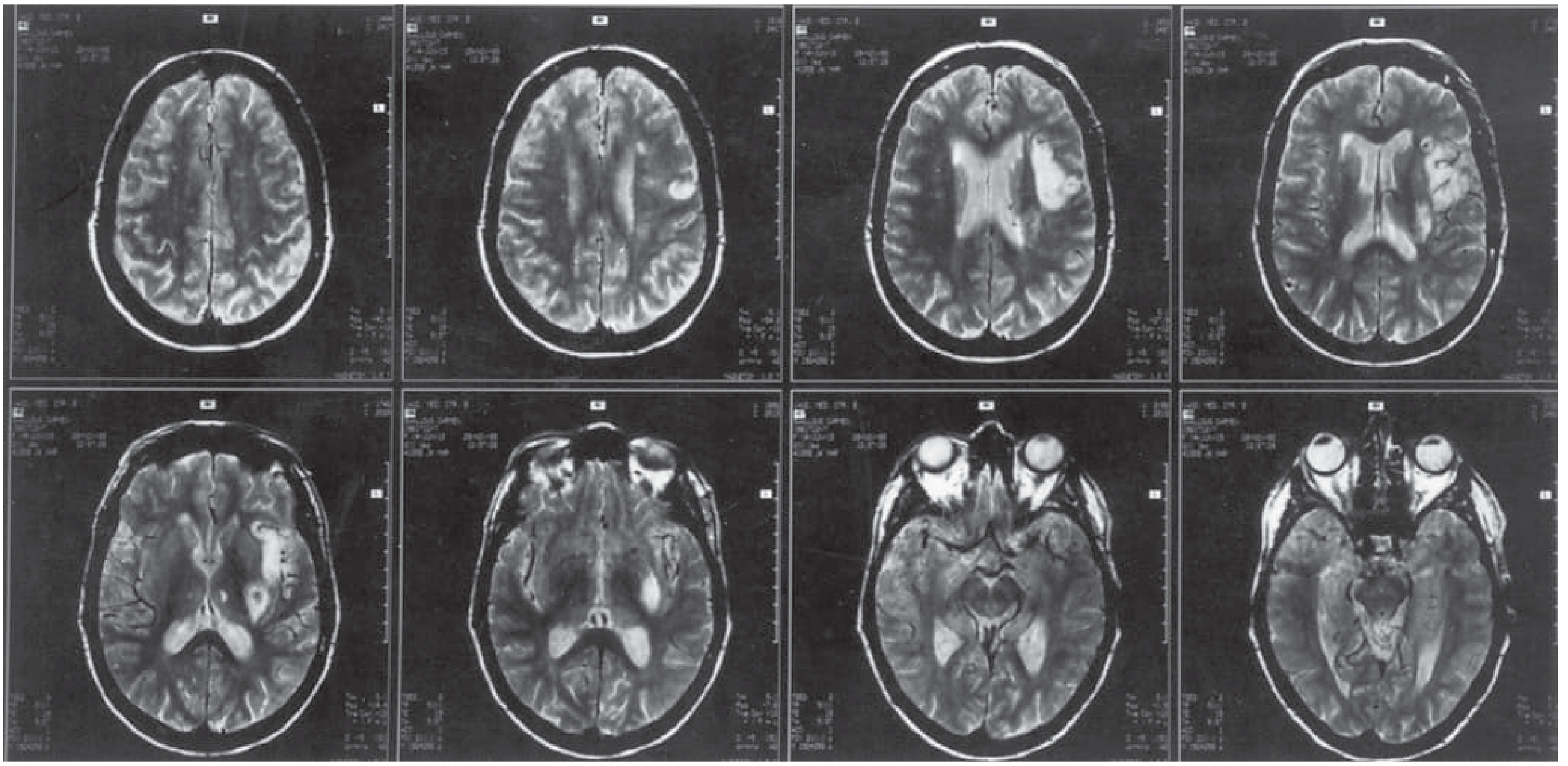
Wernicke's aphasia is a fluent aphasia caused by damage to Wernicke's area — the posterior superior temporal gyrus of the dominant (left) hemisphere. It is characterized by impaired language comprehension with preserved speech fluency, resulting in speech that sounds normal in rhythm and articulation but is largely devoid of meaning.
It is the syndromic opposite of Broca's aphasia: where Broca's is non-fluent with good comprehension, Wernicke's is fluent with poor comprehension.
Anatomical Basis
Lesion location: Posterior portion of the left superior temporal gyrus (Wernicke's area), extending into the inferior parietal lobule and middle temporal gyrus. The most common cause is infarction in the inferior division of the left middle cerebral artery (MCA).
Clinical Features
Bedside Profile
| Feature | Finding |
|---|---|
| Spontaneous speech | Fluent, normal prosody and articulation; paraphasic errors; may be logorrheic |
| Comprehension | Impaired — even for simple commands |
| Repetition | Impaired |
| Naming | Impaired — bizarre paraphasic substitutions |
| Reading | Impaired — both aloud and for comprehension |
| Writing | Fluent but meaningless; paragraphic with spelling errors |
| Motor/sensory deficits | Usually absent |
| Visual field | ± Right homonymous hemianopia (upper quadrant most common — temporal optic radiation involvement) |
Speech Characteristics
Speech is empty of meaning despite sounding superficially fluent. Several types of errors occur:
- Verbal (semantic) paraphasias: substituting a wrong word (e.g., "bus" for "taxi"; "The grass is blue")
- Literal (phonemic) paraphasias: substituting sounds within a word (e.g., "pish" for "fish")
- Neologisms: completely novel non-words (e.g., "grumps")
- Jargon aphasia: in severe cases, speech becomes entirely incomprehensible gibberish
Comprehension
Patients fail to understand spoken and written language. They may execute a few simple commands involving axial muscles (e.g., "close your eyes," "stick out your tongue") even in severe cases, which is a clinically useful distinguishing point.
Behavioral/Psychiatric Features
Strikingly, patients are often anosognosic — unaware of or unconcerned about their deficit. They may appear to believe they are communicating normally. Over time, some become angry or paranoid when others cannot understand them. This contrasts with Broca's aphasia, where patients are typically frustrated and depressed.
This anosognosia can lead to misdiagnosis as a psychotic disorder — the paraphasic speech of severe Wernicke's aphasia can superficially resemble schizophrenic thought disorder.
Pathophysiology
Wernicke's area sits adjacent to the primary auditory cortex (Heschl's gyri). It serves as the cortical hub for:
- Decoding auditory language — matching sound patterns to word meaning
- Generating meaningful language — selecting correct words during speech production
When damaged, the lexical-semantic system breaks down: incoming speech cannot be matched to meaning, and outgoing speech cannot retrieve the correct words, resulting in the characteristic fluent-but-meaningless output.
Lesions also disconnect Wernicke's area from Broca's area (via the arcuate fasciculus), which explains the associated impairment in repetition.
Wernicke–Geschwind Model
Wernicke's aphasia is central to the Wernicke–Geschwind model of language:
- Broca's area (left inferior frontal): speech production/articulation
- Wernicke's area (left posterior superior temporal): language comprehension and word selection
- Arcuate fasciculus: white matter tract connecting both areas
- Damage to Wernicke's area → Wernicke's aphasia
- Damage to the arcuate fasciculus alone → Conduction aphasia (fluent, good comprehension, poor repetition)
Etiology
| Cause | Notes |
|---|---|
| Ischemic stroke | Left MCA inferior division — most common |
| Hemorrhagic stroke | Left temporal lobe hematoma |
| Tumor | Less abrupt onset |
| Encephalitis | Herpes simplex encephalitis may affect temporal lobes |
| Trauma | Penetrating injury to posterior temporal region |
Other Names (and Their Limitations)
Wernicke's aphasia is sometimes called receptive, sensory, posterior, or fluent aphasia. These terms are imprecise — Wernicke's aphasia is not purely a receptive deficit, as expression is also severely paraphasic. The eponymic name is preferred.
— Bradley and Daroff's Neurology in Clinical Practice, p. 209; Adams and Victor's Principles of Neurology, 12th ed., p. 509; Neuroanatomy through Clinical Cases, 3rd ed.
Brocas aphasia
Finding Sources
Searching Images
Broca's aphasia brain lesion frontal lobe MRI
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of Broca's aphasia:
Broca's Aphasia
Historical Background
In 1861, the French physician Paul Broca described a non-fluent speech disorder in two patients — one of whom could say only the syllable "tan." He initially called the condition aphemia, though the term aphasia was later adopted. The responsible cortical region (left inferior frontal gyrus) became known as Broca's area.
Anatomical Basis
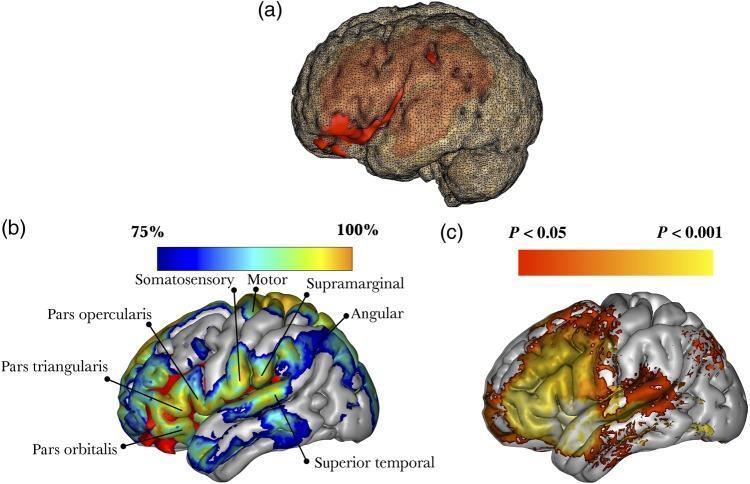
Lesion location: Posterior part of the left inferior frontal gyrus (Brodmann areas 44 and 45), typically extending into adjacent prerolandic cortex, the insula, and subcortical white matter. The full syndrome requires damage to:
- The cortical Broca area (BA 44/45)
- The lower precentral gyrus
- Subcortical white matter (rostral subcallosal fasciculus + periventricular white matter)
Lesions restricted to cortical Broca's area alone usually produce only a mild, transient deficit ("mini-Broca"). Most patients with lasting Broca's aphasia have larger lesions involving the surrounding operculum and insula.
Most common cause: Infarction in the superior division of the left MCA.
Clinical Features
Bedside Profile
| Feature | Finding |
|---|---|
| Spontaneous speech | Non-fluent — mute, telegraphic, or agrammatic; often dysarthric |
| Naming | Impaired — tip-of-the-tongue phenomenon; literal paraphasias |
| Comprehension | Relatively intact (mild difficulty with complex syntax) |
| Repetition | Impaired — mirrors effortful spontaneous speech |
| Reading | Often impaired (especially syntax-dependent reading) |
| Writing | Impaired — dysmorphic, dysgrammatic |
| Associated signs | Right hemiparesis, hemisensory loss, ± oral/limb apraxia |
Speech Characteristics
The defining feature is non-fluency — speech is halting, effortful, and poorly prosodic (monotonous). The classic pattern is agrammatism (telegraphic speech): content words (nouns, verbs) are preserved but grammatical function words and morphemes are dropped.
Example: instead of "My wife came to the hospital," the patient says "wife... come... hospital."
In severe cases:
- Complete mutism — no words at all
- Verbal stereotypy/automatisms — a single syllable or word repeated compulsively (as with Broca's patient "Tan")
- Overlearned speech is relatively spared — patients can often sing familiar songs, count, or say greetings ("hi," "fine, thank you") better than produce novel utterances
- Emotional speech (expletives when frustrated) may be preserved, highlighting the distinction between propositional and automatic speech
In milder cases ("mini-Broca"):
- Reduced phrase length (<5 words)
- Content words predominate over function words
- Abnormal prosody with preserved basic syntax
Comprehension
Comprehension is relatively preserved but not entirely intact. Patients fail on syntactically complex sentences that depend on grammatical structure rather than word meaning — for example, sentences with embedded clauses:
"The rug that Bill gave to Betty tripped the visitor." This likely reflects frontal lobe demands on working memory and syntactic processing.
Associated Neurological Signs
- Right hemiparesis (arm > leg) — from adjacent precentral gyrus involvement
- Right hemisensory loss
- Oral and limb apraxia — inability to perform purposeful orofacial movements on command (e.g., "blow a kiss," "lick your lips") despite intact motor function. This can be mistaken for comprehension failure; testing with yes/no questions or pointing confirms comprehension is intact.
- Buccofacial apraxia — reflects damage to the anterior insular cortex, which coordinates the orolingual movements of articulation
Behavioral/Psychiatric Features
Patients with Broca's aphasia are typically aware of and frustrated by their deficits, in stark contrast to Wernicke's aphasia. Depression is a frequent and clinically important association — it may limit rehabilitation and requires treatment. As deficits improve, depression usually resolves.
Pathophysiology
Broca's area (BA 44/45) serves as the cortical hub for:
- Motor programming of speech — coordinating the sequential articulatory movements needed for fluent speech
- Syntactic processing — encoding grammatical structure in both production and comprehension
- Verbal working memory — maintaining language sequences
Damage disconnects Broca's area from Wernicke's area (via the arcuate fasciculus), impairing repetition. Damage to the adjacent anterior insula disrupts the coordination of orolingual movements responsible for articulation.
Comparison with Wernicke's Aphasia
| Feature | Broca's Aphasia | Wernicke's Aphasia |
|---|---|---|
| Fluency | Non-fluent | Fluent |
| Comprehension | Relatively intact | Impaired |
| Repetition | Impaired | Impaired |
| Paraphasias | Mild; mainly literal | Prominent; verbal + neologisms |
| Motor deficits | Right hemiparesis (common) | Usually absent |
| Visual field | Usually intact | ± Right upper quadrantanopia |
| Awareness | Aware, frustrated, depressed | Unaware (anosognosia) |
| Lesion | Left inferior frontal (MCA superior) | Left posterior temporal (MCA inferior) |
Terminology Note
Broca's aphasia is also called expressive, motor, nonfluent, or anterior aphasia. These terms are imprecise — comprehension is not fully preserved, and some features overlap with other syndromes. The eponymic name Broca's aphasia is preferred.
— Bradley and Daroff's Neurology in Clinical Practice, pp. 207–208; Adams and Victor's Principles of Neurology, 12th ed.; Neuroanatomy through Clinical Cases, 3rd ed., p. 922
This is a shared conversation. Sign in to Orris to start your own chat.