Renal trauma in detail with reference to standard textbooks
Reading File
Finding Sources
Finding Sources
Searching Images
renal trauma classification CT scan grading
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have now gathered comprehensive information from five major textbooks. Here is the detailed review of renal trauma:
Renal Trauma — A Detailed Review
1. Epidemiology and Incidence
The kidney is the most commonly injured genitourinary organ, sustaining injury in approximately 10% of all abdominal and pelvic trauma cases. Isolated urologic injuries are uncommon because the genitourinary tract is well sheltered within the retroperitoneum. Approximately 80% of renal trauma results from blunt mechanisms, with the remainder from penetrating injuries. In the setting of penetrating trauma to the flank and back, renal injuries occur in about 5% of cases. — Sabiston Textbook of Surgery, p. 748
The paediatric kidney is more vulnerable to injury than the adult kidney, being larger, more mobile, with less perirenal fat and less ossified ribs for protection. Patients with pre-existing renal anomalies — horseshoe kidney, renal cyst, hydronephrosis, renal neoplasm, or transplant — are at especially high risk, and an underlying lesion should be suspected when CT findings are disproportionate to the mechanism. — Grainger & Allison's Diagnostic Radiology, p. 920
2. Mechanisms of Injury
Blunt Trauma
- Direct blow to the flank: Compresses the kidney against the ribs and vertebrae, causing contusion or laceration.
- Rapid deceleration (road traffic accidents, falls from height): Displaces the kidneys, which are tethered only at the renal pelvis. Shearing forces lacerate the parenchyma or tear the collecting system at the pelvioureteric junction (PUJ).
- Stretching of accessory or intrarenal branches of the renal artery causes segmental infarction.
- Lateral displacement stretches the renal vasculature → intimal tears → dissection → partial or complete thrombosis of the main renal pedicle. The artery typically occludes between its proximal and middle thirds. Complete avulsion of the vein or artery is the end result of overstretching. — Grainger & Allison's Diagnostic Radiology, p. 920
Penetrating Trauma
- Gunshot wounds and stab wounds. Bullets impart large energy transfer, and damage can extend 2 cm beyond the point of transection. Soft tissue and bone alter the bullet trajectory. — Campbell-Walsh-Wein Urology, p. 2642
- Previously, all penetrating injuries necessitated surgical exploration; however, contrast-enhanced MDCT now permits conservative management in stable patients. Penetrating trauma carries a higher incidence of ancillary injuries (up to 80% of patients) and increased risk of infection. — Grainger & Allison's Diagnostic Radiology, p. 920
3. Classification — AAST Organ Injury Scale (OIS)
The American Association for the Surgery of Trauma (AAST) grading system, originally devised in 1989, is the most widely used and accepted classification of renal injury. The scale was validated in multiple series as a predictive tool for clinical outcomes, including the need for surgery, angiographic intervention, and nephrectomy rate. The system was updated in 2018 by Kozar et al. to incorporate radiological findings and contemporary management data. — Campbell-Walsh-Wein Urology, p. 2642–2643
| Grade | Description | AIS Severity |
|---|---|---|
| I | Subcapsular haematoma or parenchymal contusion without laceration | 2 |
| II | Perirenal haematoma confined to Gerota fascia; renal laceration ≤1 cm depth without urinary extravasation | 2 |
| III | Renal laceration >1 cm depth without urinary extravasation; any injury with vascular injury or active bleeding contained within Gerota fascia | 3 |
| IV | Parenchymal laceration with urinary extravasation; renal pelvis laceration and/or UPJ disruption; active bleeding beyond Gerota fascia into retroperitoneum or peritoneum; segmental or complete kidney infarction caused by vessel thrombosis without active bleeding | 4 |
| V | Main renal artery or vein laceration or avulsion of hilum; devascularized kidney with active bleeding; shattered kidney with loss of identifiable parenchymal anatomy | 5 |
Bilateral injuries: advance one grade for bilateral injuries up to Grade III.
— Sabiston Textbook of Surgery, Table 39.1, p. 748
Key update (2018): Grade IV now explicitly includes AV malformation and pseudoaneurysm. Grade V now includes devascularized kidney with active bleeding and shattered kidney. About a third of Grade III injuries were upstaged to Grade IV under the revised system, increasing heterogeneity within Grade IV. — Sabiston Textbook of Surgery, p. 748–749
Outcomes by grade:
- Grades I–III (75–98% of all renal injuries): no intervention usually required
- Most Grade IV injuries: managed with interventional angiography and active surveillance
- Grade V injuries: highest incidence of exploration and lowest renal salvage rate
- If surgical exploration is performed: 64% nephrectomy rate regardless of operative intent
- Surgery is currently required in less than 10% of blunt renal injuries — Grainger & Allison's Diagnostic Radiology, p. 921
4. Clinical Presentation
Hematuria
Hematuria is the cardinal sign of renal trauma; however, its absence does not exclude significant injury.
- Hematuria was absent in 7% of 420 Grade IV renal injuries, in 11% of patients with renal gunshot wounds, and in 36% of renal vascular injuries from blunt trauma.
- Approximately 50% of UPJ injuries have no hematuria.
- In blunt trauma, microscopic hematuria + hypotension significantly increases the incidence of severe renal injury (Mee & McAninch, 1989).
- The first voided or catheterized urine aliquot should be used — later samples may be diluted by resuscitation. — Campbell-Walsh-Wein Urology, p. 2642
Physical Examination
- Flank pain, flank ecchymosis or bruising ("Grey Turner's" pattern)
- Rib fractures, lower rib tenderness
- Palpable flank mass (haematoma)
- Signs of haemodynamic compromise
- For penetrating injuries: identify entry and exit wounds — Sabiston Textbook of Surgery, p. 748
5. Imaging
Indications for CT Imaging (AUA/EAU Guidelines)
| Indication |
|---|
| All haemodynamically stable patients with gross haematuria |
| Microscopic haematuria with hypotension (SBP <90 mmHg) |
| Significant acceleration/deceleration mechanism (high-speed MVA, fall from height) |
| Penetrating abdominal, flank, or lower thoracic trauma (with or without haematuria) |
| Physical examination findings consistent with renal injury |
| All paediatric patients with >5 RBCs/HPF |
— Campbell-Walsh-Wein Urology, p. 2643; Grainger & Allison's Diagnostic Radiology, Table 36.1, p. 921
Patients with microscopic haematuria without hypotension can be observed clinically without imaging, as significant injury in this group is rare (<0.0016%). — Campbell-Walsh-Wein Urology, p. 2643
CT Protocol
The preferred study is contrast-enhanced MDCT (CE-MDCT) with:
- Unenhanced phase: baseline density assessment
- Arterial phase: demonstrates parenchymal enhancement, symmetry, and active bleeding (high-attenuation contrast extravasation outside the renal vasculature)
- Portal venous phase (70 seconds): parenchymal assessment, perirenal collections
- Delayed phase (5–10 minutes): assessment of the opacified collecting system for urinary extravasation — Grainger & Allison's Diagnostic Radiology, p. 921
Key CT Findings Requiring Intervention
| CT Finding | Significance |
|---|---|
| Medial haematoma | Vascular pedicle injury |
| Medial urinary extravasation | Renal pelvis or UPJ injury |
| Lack of parenchymal contrast enhancement | Main renal arterial occlusion |
| Active intravascular contrast extravasation (blush) | Arterial injury with brisk bleeding |
| Perirenal haematoma >4 cm | Associated with 66% increased likelihood of intervention per cm increase |
| Intravascular contrast extravasation | Threefold increase in odds of requiring haemorrhage intervention |
— Campbell-Walsh-Wein Urology (Key Points); Sabiston Textbook of Surgery, p. 749
CT Appearance by Grade
- Grade I: Ill-defined low-attenuation areas within parenchyma (contusion); non-enlarging subcapsular haematoma crescentic in shape
- Grade II: Cortical laceration <1 cm; small perirenal haematoma contained in Gerota fascia
- Grade III: Laceration >1 cm into medulla, larger perirenal haematoma still within Gerota fascia
- Grade IV: Laceration extending into collecting system with urinary extravasation; segmental renal infarction
- Grade V: Shattered kidney; avulsion of hilar vessels; devascularized kidney
— Grainger & Allison's Diagnostic Radiology, Table 36.2, p. 921
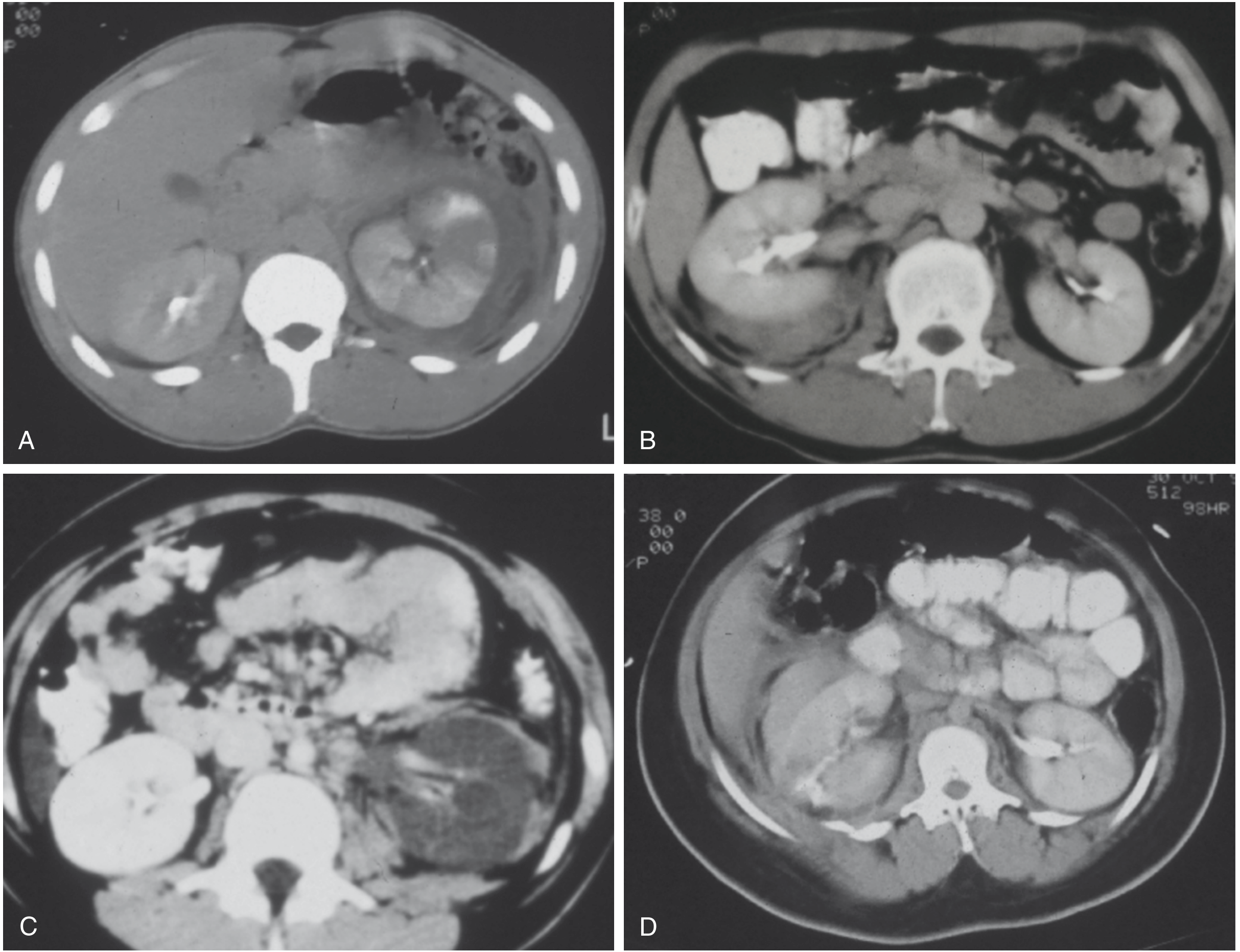
CT scans showing renal trauma grades: (A) Grade I — left renal contusion with heterogeneous enhancement; (B) Grade II — small right posterior perirenal haematoma; (C) Grade IV — left renal artery thrombosis without active bleeding; (D) Grade IV laceration with posterolateral contrast extravasation. — Sabiston Textbook of Surgery, Fig. 39.1

Axial contrast-enhanced CT demonstrating Grade III renal injury — left kidney surrounded by massive heterogeneous perirenal haematoma with parenchymal disruption.
One-Shot IVP (Intraoperative)
In haemodynamically unstable patients going directly to the operating room without prior CT, a one-shot intraoperative IVP (2 mL/kg IV contrast, single abdominal radiograph at 10 minutes) can confirm presence of a contralateral kidney before nephrectomy. — Sabiston Textbook of Surgery, p. 748
Ultrasound
Ultrasound has limited sensitivity for detecting renal lacerations but can identify perirenal collections. FAST examination does not reliably exclude renal injury. — Grainger & Allison's Diagnostic Radiology
6. Management
General Principle
The prime goal is preservation of renal function. Renal trauma management has become largely non-operative in modern times, especially for low- to intermediate-grade injuries. — Schwartz's Principles of Surgery, p. 1799
Haemodynamic Status Guides Decision-Making
Haemodynamically Unstable Patients:
- Require immediate intervention: surgery or, in select cases, angioembolization
- Those with critical CT findings (perirenal haematoma >4 cm and/or intravascular contrast extravasation) require immediate intervention — Sabiston Textbook of Surgery, p. 749
Haemodynamically Stable Patients:
- Non-operative management (NOM) is first-line
- Serial haematocrit monitoring; bed rest (though bed rest has fallen out of favour as a mandatory adjunct)
- Patients with Grade IV injury (especially urinary extravasation) require repeat CT to ensure resolution of extravasation, failing which a ureteral stent or nephrostomy tube is placed — Schwartz's Principles of Surgery, p. 1801
Non-Operative Management (NOM)
NOM is appropriate for:
- All haemodynamically stable patients, regardless of injury grade
- Even high-grade (IV–V) injuries in selected stable patients: recent data show that a subset of Grade V injuries can be managed non-operatively without increased hospital stay
Protocol:
- Bed rest until gross haematuria resolves and blood counts are stable
- Grade I–II: no interval imaging if asymptomatic
- Grade IV–V: repeat CT imaging to assess for urinoma, haematoma expansion, or abscess
- Indications to reassess with repeat CT: fever, worsening flank pain, ongoing blood loss, abdominal distention
- Urinary extravasation: often resolves spontaneously; if persistent or expanding urinoma, drain with ureteral stent ± percutaneous drain — Sabiston Textbook of Surgery, p. 749; Schwartz's Principles of Surgery, p. 1801
Angioembolization
- Selective angioembolization is an effective, minimally invasive method to stop active bleeding from parenchymal lacerations and segmental arterial injuries
- Preferred over open surgery for Grade IV injuries in haemodynamically stable patients
- Indicated when CT shows active contrast extravasation (blush) in a patient who can tolerate the procedure — Campbell-Walsh-Wein Urology (Key Points)
Absolute Indications for Surgical/Radiological Intervention
- Expanding, pulsatile retroperitoneal haematoma
- Renal pedicle avulsion
- Haemodynamic instability unresponsive to resuscitation
- Ureteropelvic junction (UPJ) avulsion
Relative Indications for Intervention
- Urinary extravasation in a devascularized renal unit
- Renal injury with concomitant colon or pancreatic injury
- Urinary extravasation from parenchymal injury (persistent) — Sabiston Textbook of Surgery, p. 749
7. Surgical Approach
Access
- Transabdominal (midline laparotomy): preferred — allows complete visceral inspection
- The small bowel is eviscerated and an incision is made medial to the inferior mesenteric vein, extended to the Ligament of Treitz, creating a window over the aorta at the level of the renal arteries
- Renal vessels are isolated with individual vessel loops to achieve vascular control before entering the perirenal haematoma (McAninch's approach — early vascular control)
Vascular Control
- Renal veins are retracted cephalad to expose the renal arteries below
- If landmarks are obscured by haematoma, dissect through haematoma to the anterior aorta
- Kidney is exposed by incising the white line of Toldt, lateralizing the colon, then entering Gerota fascia
- Splenic (left) or hepatic (right) attachments are freed for kidney mobility — Sabiston Textbook of Surgery, p. 749–750
Renal Reconstruction (Renorrhaphy)
Steps:
- Complete kidney exposure
- Temporary vascular occlusion (warm ischaemia time ≤30 minutes)
- Debridement of non-viable tissue
- Haemostasis (individual vessel ligation)
- Closure of collecting system (if entered), with absorbable sutures
- Reapproximation of parenchymal defect with 3-0 Vicryl sutures over a bolster of absorbable haemostatic agent (Surgicel/Nu-Knit)
- Cover repair with omentum or Gerota fascia flap
- Place closed suction drain around the repair site — Sabiston Textbook of Surgery, p. 750
Nephrectomy
- Performed for Grade V injury (shattered kidney, hilar avulsion) or when renorrhaphy is not possible
- Most common renal surgery performed in the context of trauma in modern times — Schwartz's Principles of Surgery, p. 1803
- Early vascular control (before opening the haematoma) minimizes nephrectomy rates
- Grade V injuries have the highest nephrectomy rates; overall trauma nephrectomy rate at exploration is ~64%
8. Complications
| Complication | Details |
|---|---|
| Urinoma | Urinary extravasation forming a perirenal collection; treat with ureteral stent ± percutaneous drain |
| Perinephric abscess | Secondary infection of haematoma or urinoma |
| Delayed haemorrhage | From pseudoaneurysm or AV fistula; manage with angioembolization |
| Hypertension | "Page kidney" — compression by haematoma causes renin-mediated hypertension |
| Renal artery thrombosis | Results in segmental or complete infarction; revascularization rarely successful beyond 4–6 hours |
| Arteriovenous fistula | May present weeks after injury with haematuria, hypertension, heart failure |
9. Penetrating Renal Trauma
- Accounts for ~20% of all renal injuries
- Higher rate of associated organ injuries (up to 80%)
- Higher infection risk than blunt trauma
- Penetrating injuries with retroperitoneal haematoma + haemodynamic instability → surgical exploration
- Selected isolated penetrating renal injuries in stable patients → conservative management is a viable option
- Stab wounds causing superficial lacerations without collecting system involvement can often be observed — Sabiston Textbook of Surgery, p. 749; Grainger & Allison's Diagnostic Radiology, p. 920
10. Special Situations
Pre-existing Renal Pathology
Patients with hydronephrosis, renal cysts, renal tumours, horseshoe kidney, or transplant kidneys sustain injury disproportionate to the mechanism. A ruptured angiomyolipoma can mimic traumatic renal injury. These patients should have a lower threshold for imaging. — Grainger & Allison's Diagnostic Radiology, p. 920
Paediatric Renal Trauma
- Children are more susceptible due to anatomical differences (larger kidneys, less perirenal fat, less ossified ribs)
- Criteria for imaging in children: >5 RBCs/HPF (lower threshold than adults)
- Conservative management is preferred; outcomes are excellent with NOM — Campbell-Walsh-Wein Urology, p. 2643
11. Key Points Summary (Campbell-Walsh-Wein Urology)
- Expectant management strategies allow maximal renal preservation
- The degree of haematuria and the severity of renal injury do not consistently correlate
- Contrast-enhanced CT is the gold standard imaging modality
- Patients with microscopic haematuria without shock can be observed without imaging
- Haemodynamically stable, well-staged renal injuries can be conservatively managed even at high grades
- Selective angioembolization provides effective minimally invasive haemorrhage control
- Critical CT predictors of intervention: medial haematoma, medial urinary extravasation, absent parenchymal enhancement, active contrast blush
- Haemodynamic instability despite resuscitation → immediate intervention
- Urinary extravasation often resolves spontaneously; renal pelvis/proximal ureteral avulsion demands prompt intervention
Sources:
- Sabiston Textbook of Surgery, 21st ed. (pp. 747–750)
- Campbell-Walsh-Wein Urology, 12th ed. (pp. 2642–2645)
- Schwartz's Principles of Surgery, 11th ed. (pp. 1799–1803)
- Grainger & Allison's Diagnostic Radiology (pp. 920–922)
- Smith & Tanagho's General Urology, 19th ed.
This is a shared conversation. Sign in to Orris to start your own chat.