How to depotash a patient
Reading File
Finding Sources
Searching PubMed
hyperkalemia management treatment
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information to give a complete answer.
How to "De-potash" a Patient (Treatment of Hyperkalemia)
"Depotashing" refers to lowering an elevated serum potassium (hyperkalemia, K+ > 5.0 mEq/L). Management follows three sequential pillars:
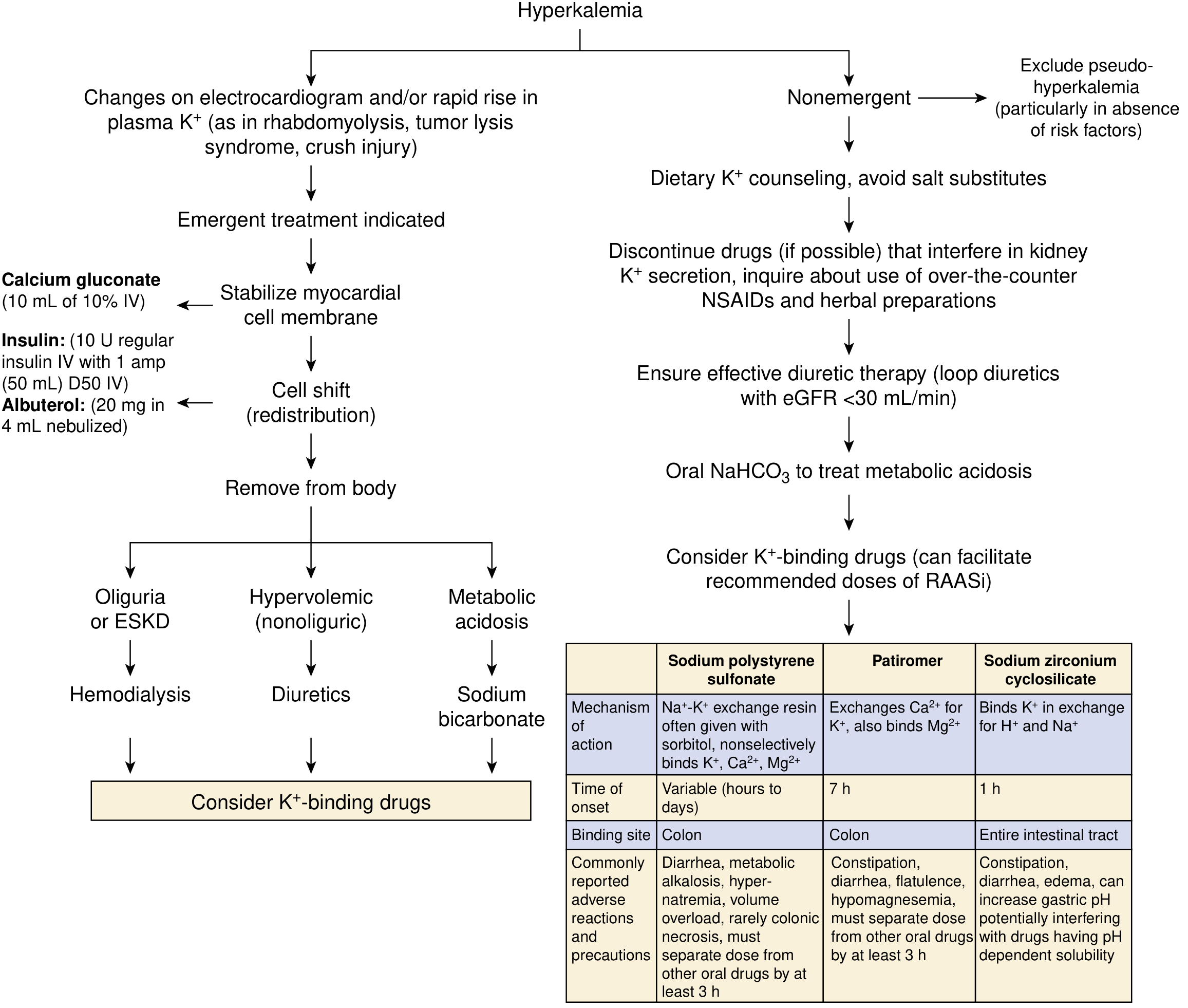
Step 0 - Immediate Assessment
- 12-lead ECG immediately - look for peaked T waves, prolonged PR, wide QRS, sine wave pattern, or VF.
- Any ECG change OR K+ ≥ 6.5-7.0 mEq/L = medical emergency requiring admission and continuous cardiac monitoring.
- Exclude pseudo-hyperkalemia (hemolyzed sample, extreme leukocytosis/thrombocytosis).
Pillar 1 - Stabilize the Heart (Membrane Protection)
Intravenous Calcium - does NOT lower K+, but protects the myocardium immediately.
| Preparation | Dose | Route | Onset | Duration |
|---|---|---|---|---|
| Calcium gluconate 10% | 10 mL (repeat if needed) | IV over 2-3 min | 1-3 min | 30-60 min |
| Calcium chloride 10% | 3-4 mL | IV over 2-3 min | 1-3 min | 30-60 min |
- Repeat if ECG changes persist or recur after initial improvement.
- Caution in digoxin toxicity: hypercalcemia potentiates digoxin toxicity. If needed, dilute in 100 mL D5W and infuse over 20-30 min.
- Do NOT mix calcium with bicarbonate (precipitates calcium carbonate).
Pillar 2 - Shift K+ Into Cells (Temporizing)
These buy time; they do not remove K+ from the body.
A. Insulin + Glucose (most reliable)
- 10 units regular insulin IV + 50 mL of 50% dextrose (D50) bolus immediately.
- Effect: starts in 10-20 min, peaks at 30-60 min, lasts 4-6 hours. Drops K+ by ~0.5-1.2 mEq/L.
- Follow with 5-10% dextrose infusion at 50-100 mL/hr to prevent hypoglycemia (occurs in up to 75% without ongoing glucose).
- If blood glucose > 200-250 mg/dL: give insulin alone, monitor glucose closely.
- Never give dextrose without insulin - may paradoxically worsen hyperkalemia in insulin-deficient patients.
B. Beta-2 Agonists (additive to insulin)
- Albuterol (salbutamol) 20 mg nebulized over 10 minutes.
- Onset ~30 min; effect is additive to insulin and also reduces risk of hypoglycemia.
- Note: the dose for hyperkalemia is far higher than asthma dosing.
- IV albuterol 0.5 mg is equivalent (available in Europe, not the US).
C. Sodium Bicarbonate (controversial)
- Useful only if severe metabolic acidosis is present (HCO3 < 10 mmol/L) or in patients with residual kidney function.
- Does NOT enhance the K+-lowering effect of insulin or albuterol.
- Little benefit in ESKD/dialysis patients without residual renal function.
- Do not give in same IV line as calcium.
Pillar 3 - Remove K+ from the Body (Definitive)
A. Loop Diuretics
- Furosemide (or bumetanide): effective if patient has adequate residual kidney function.
- Useful for hypervolemic, non-oliguric patients.
B. Dialysis
- Most effective method but cannot usually be initiated fast enough to skip the above steps.
- Indications: severe AKI, ESKD, oliguric hyperkalemia unresponsive to medical management.
- Hemodialysis preferred over peritoneal dialysis for speed.
C. Potassium Binders (adjuncts, not emergency monotherapy)
| Drug | Mechanism | Onset | Dose | Key Adverse Effects |
|---|---|---|---|---|
| Sodium polystyrene sulfonate (SPS / Kayexalate) | Na+-K+ exchange resin | Hours to days | 50 g PO or PR in sorbitol | Diarrhea, metabolic alkalosis, rare colonic necrosis (FDA black box) |
| Patiromer (Veltassa) | Binds K+ in exchange for Ca2+ in colon | ~7 hours | 8.4 g once daily PO | Constipation, hypomagnesemia; separate from other oral meds by 3 h |
| Sodium zirconium cyclosilicate (Lokelma) | Binds K+ in exchange for H+/Na+ across entire GI tract | ~1 hour | 10 g TID x 48h, then 5 g daily | Constipation, edema (high sodium content); raises gastric pH |
Patiromer and zirconium cyclosilicate are approved for chronic management and are the preferred binders for long-term use. SPS is not approved for chronic use.
Non-Emergent / Chronic Hyperkalemia Management
- Dietary counseling: restrict K+ to ~60 mEq/day; avoid salt substitutes (KCl).
- Medication review: stop/reduce ACE inhibitors, ARBs, NSAIDs, potassium-sparing diuretics, heparin if possible.
- Ensure effective diuretic therapy: loop diuretics are especially important when eGFR < 30 mL/min.
- Oral NaHCO3: corrects metabolic acidosis, enhances renal K+ excretion in patients with residual kidney function.
- Potassium binders (patiromer or zirconium cyclosilicate): can also facilitate continued use of RAASi at recommended doses in CKD/heart failure patients.
Quick Reference Summary
| Intervention | Goal | K+ Drop | Onset | Duration |
|---|---|---|---|---|
| IV Calcium | Membrane stabilization | None | 1-3 min | 30-60 min |
| Insulin + Glucose | Cell shift | 0.5-1.2 mEq/L | 10-20 min | 4-6 h |
| Nebulized Albuterol 20 mg | Cell shift | 0.5-1.0 mEq/L | 30 min | 2-4 h |
| NaHCO3 | Cell shift (+ renal excretion) | Variable | 30-60 min | Variable |
| Loop diuretics | Removal | Variable | 30-60 min | Hours |
| Dialysis | Removal | 1-2+ mEq/L/session | 1-2 h setup | Rapid |
| K+ binders | Removal (GI) | 0.5-1.0 mEq/L | Hours-days | Chronic |
Sources: Brenner & Rector's The Kidney (9th ed.), p. 773-774 | NKF Primer on Kidney Diseases, 8e, p. 128-129 | Fischer's Mastery of Surgery, 8th ed., p. 218
Recent evidence note: A 2025 network meta-analysis (PMID 40542996) confirms novel K+ binders (patiromer and zirconium cyclosilicate) are superior to SPS in CKD/heart failure patients needing RAASi, reinforcing the current shift away from SPS for chronic management.
This is a shared conversation. Sign in to Orris to start your own chat.