Genital fistula in detail post graduate level for exam with detail management from barek and novak
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from Berek & Novak's Gynecology. Let me compile the complete, detailed postgraduate-level answer.
Genital Fistula - Postgraduate Level (Berek & Novak's Gynecology)
Definition
A genital fistula is an acquired abnormal communication between the genital tract and adjacent hollow viscera - the urinary tract (urinary fistula) or gastrointestinal tract (intestinal fistula). It results in involuntary loss of urine, flatus, or feces through the vagina, representing one of the most devastating and socially disabling conditions in gynecology.
Classification
By Adjacent Organ
| Type | Communication |
|---|---|
| Vesicovaginal (VVF) | Bladder - Vagina (most common) |
| Urethrovaginal | Urethra - Vagina |
| Ureterovaginal | Ureter - Vagina |
| Vesicocervical/Vesicouterine | Bladder - Cervix/Uterus |
| Rectovaginal (RVF) | Rectum - Vagina |
| Colovaginal | Colon - Vagina |
| Enterovaginal | Small bowel - Vagina |
| Combined | Bladder + rectum - Vagina |
By Etiology
- Obstetric (most common worldwide - developing countries)
- Surgical/Iatrogenic (most common in developed countries)
- Radiation-induced
- Malignancy-related
- Inflammatory (Crohn disease, PID, endometriosis)
- Congenital (rare)
Epidemiology and Etiology
Global Perspective
-
Developing countries: The predominant cause worldwide is prolonged obstructed labor. With malpresentation or an inadequately sized pelvis, the lower urinary tract and vagina are compressed between the fetal head and the maternal pelvic bones, sometimes for days. This leads to ischemic injury, tissue necrosis, and fistula formation. This predominantly affects young, poorly developed women in rural, underdeveloped regions.
-
Developed countries: Genitourinary fistulas usually arise from:
- Gynecologic surgery - hysterectomy (vaginal, laparoscopic, or abdominal) is the most common cause; incidence of VVF after hysterectomy is as low as 0.2%
- Pelvic malignancies
- Pelvic irradiation - bowel and bladder fistula rate after pelvic radiation therapy for cervical cancer is 1.4% to 5.3%
Specific Iatrogenic Mechanisms
- Undiagnosed bladder or ureteral trauma during hysterectomy - results in fistula typically within the first 2 weeks after surgery
- Occult thermal/energy injury during laparoscopic hysterectomy - latent spread of energy to the genitourinary system can cause delayed fistula formation
- Surgical trauma in scarred tissue - extensive adhesions or scarring from endometriosis, PID, or prior surgery predispose to RVF
Youssef Syndrome
A special condition: fistulous tract between the uterus and vagina, commonly after repeated cesarean sections. Patients present with the classic triad of cyclic hematuria, urinary incontinence, and amenorrhea.
Vesicovaginal Fistula (VVF)
Clinical Features
- Watery vaginal discharge (most characteristic presentation) - develops 10 to 14 days after surgery
- Some fistulas present as early as the first 48 to 72 hours after surgery
- Continuous, uncontrollable dribbling of urine per vaginum
- Excoriation and dermatitis of vulva and inner thighs
- Urinary tract infections
- Social isolation and psychological distress
Diagnosis
Step-by-step approach:
- Speculum examination - vaginal examination may reveal the fistulous opening at the vaginal apex after hysterectomy
- Three-swab test (Tampon test):
- Insert a cotton tampon into the vagina
- Instill methylene blue dye through a transurethral catheter into the bladder
- If the tampon stains blue → vesicovaginal fistula confirmed
- If no staining → proceed to step 3
- Pyridium test for ureterovaginal fistula:
- Administer oral pyridium (phenazopyridine)
- Within 20 minutes, the tampon stains orange if an ureterovaginal fistula is present
- CT urogram - mandatory in all suspected VVF/ureterovaginal fistula cases to fully evaluate ureteral integrity and rule out obstruction
Surgical Anatomy of the Fistula Site
- After hysterectomy: fistula site is above the bladder trigone and away from the ureters - this makes vaginal repair feasible in most patients
Vesicovaginal Fistula - Management
Conservative Management
- Foley catheter insertion for prolonged continuous bladder drainage
- Up to 15% of fistulas close spontaneously with 4 to 6 weeks of continuous bladder drainage
- This is most applicable to small, early post-surgical fistulas
- For very small "pinpoint" fistulas: attempt 10 to 14 days of transurethral catheterization first
Surgical Management (when conservative fails)
Timing:
- If closure has not occurred by 6 weeks, operative correction is necessary
- Wait 3 to 4 months from the time of diagnosis before operative repair - this allows reduction of inflammation and improvement of vascular supply
- Some authorities advocate earlier repair (within 48-72 hours) if the fistula is identified very early, before edema and inflammation set in
Approach:
- Genitourinary fistula repair is most commonly performed vaginally
- Can also be repaired through abdominal access - open, laparoscopic, or robotically
- Robotic surgery is particularly useful for fistula repair given its precision and suturing capability
Principles of Surgical Repair (Berek & Novak's Step-by-Step Technique):
- (a) Identification of the fistula site(s)
- (b) Adequate access and exposure - a pediatric Foley catheter can be placed vaginally with the balloon inflated to put downward traction on the fistula for better visualization
- (c) Debridement of all nonviable tissue
- (d) Mobilization of fresh, viable tissue (1 to 2 cm) around and all along the fistulous tract
- (e) Layered closure starting at the bladder and going out to the vagina
- (f) Minimal tension on all repaired layers
- (g) Postoperative catheterization for 7 to 14 days
- (h) Tissue grafts (e.g., Martius labial fat-pad flap) as needed for larger or recurrent fistulas
Four-Layer Closure (Vaginal Approach):
- Bladder mucosa
- Seromuscular layer
- Endopelvic fascia
- Vaginal epithelium
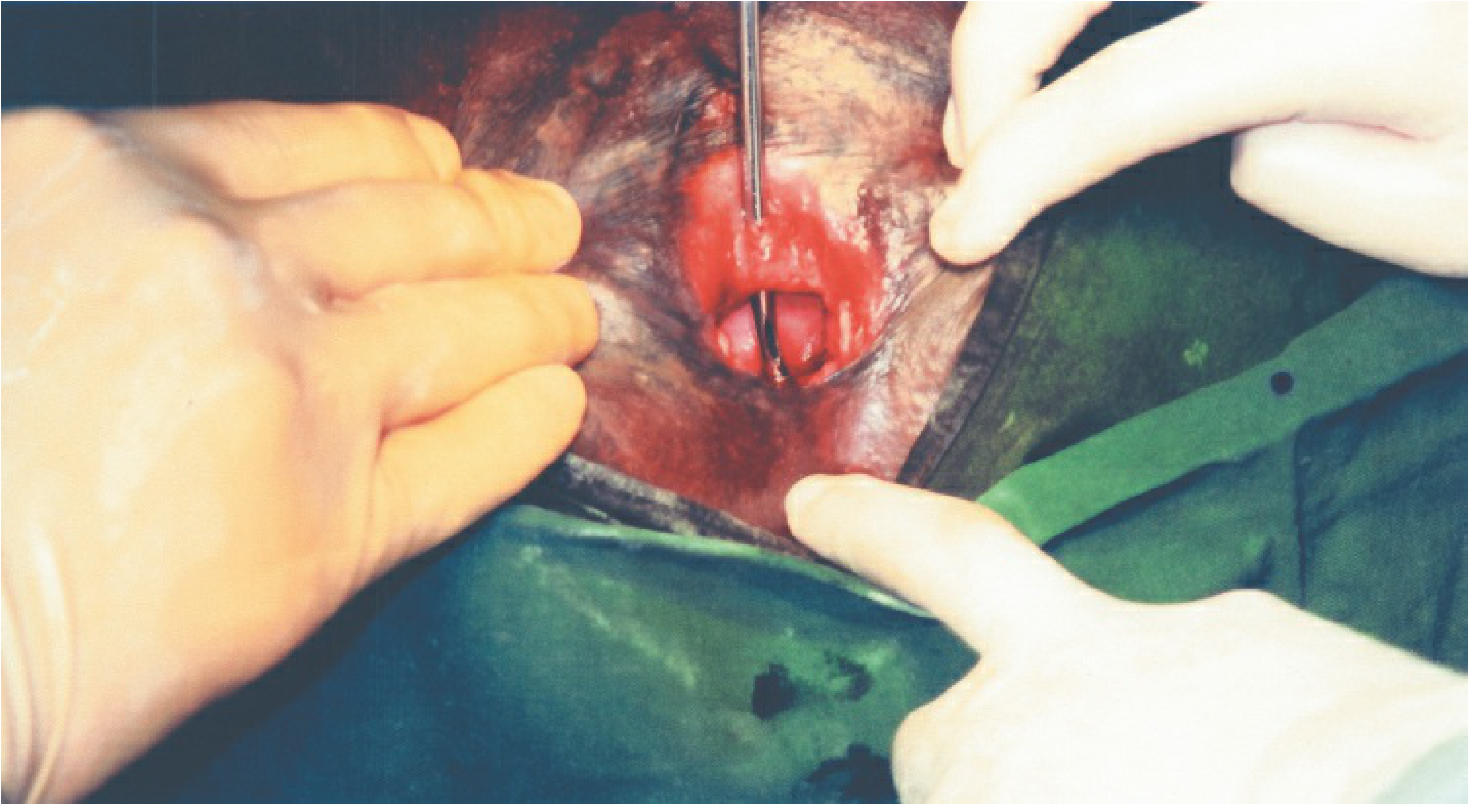
FIGURE: Vesicovaginal fistula - intraoperative exposure (Berek & Novak's Gynecology)
Martius Labial Fat-Pad Flap
- Harvested from the labium majus (contains the bulbocavernosus muscle and surrounding fat)
- Interposed between the bladder repair and vaginal closure
- Provides new vascular supply to the repair site - especially important for radiation-induced or recurrent fistulas
- Standard for large fistulas, radiation fistulas, and failed previous repairs
Ureterovaginal Fistula
Etiology
- Occurs after ureteral injury during hysterectomy or other pelvic surgery
- Ureteral obstruction presents with flank pain after surgery
- Incidence: 1% to 2% in radical hysterectomy for cervical carcinoma
Diagnosis
- CT urogram is the investigation of choice
- Obstruction usually present near the ureterovesical junction on CT scan
- Pyridium test: tampon stains orange
Management
- Attempted stent passage through ureter under cystoscopic guidance as the immediate first step
- If a catheter can pass: leave in place for at least 4 to 6 weeks (allows sutures to absorb and kinking to release)
- If catheter cannot pass: exploratory surgery and ureteral repair at the site of obstruction
- If surgery cannot be performed immediately: temporary percutaneous nephrostomy tube
Urethrovaginal Fistula
- Communication between the urethra and vagina
- Usually results from obstetric injury, urethral surgery, or trauma
- Presents with stress-type urinary incontinence (continuous dribbling)
- Management: surgical repair with layered closure; Martius flap for complex cases
Rectovaginal Fistula (RVF)
Etiology
- Obstetric trauma - difficult delivery, episiotomy extension, fourth-degree perineal laceration
- Surgical trauma after gynecologic surgery - predisposed by extensive adhesions/scarring from endometriosis, PID, or pelvic malignancy
- Radiation-induced - occurs in fewer than 2% after pelvic radiotherapy
- Crohn disease, diverticular disease, carcinoma
Clinical Features
- Passage of flatus and feces per vaginum
- Fecal-smelling vaginal discharge
- Recurrent vaginitis
- Social isolation
Diagnosis
- Speculum and digital examination - most low RVFs visible on posterior vaginal wall
- Flat Tire Test (for suspected RVF not visible on routine exam or MRI):
- Patient in Trendelenburg position
- Saline/water placed in the vagina
- Air instilled into the rectum using proctoscope or rigid sigmoidoscope
- Observation of bubbling into vaginal fluid confirms the diagnosis and location
- The rectal site of the fistula is usually also visible
- Can be performed in office or under anesthesia
- MRI pelvis - best for delineating complex or high fistulas
- Fistulography + barium enema - used especially to exclude combined large and small bowel fistulas
- Proctoscopy - detects associated anorectal pathology
Management of Rectovaginal Fistula
Conservative (for small fistulas):
- Decrease fecal stream (low-residue diet, laxatives)
- A small fistula that allows continence except for occasional flatus leak may be managed conservatively until the pelvic inflammatory process resolves (several months)
- After inflammation resolves: elective surgical repair
Surgical:
- Small RVF: transvaginal or transanal layered repair
- Large RVF (no hope of spontaneous closure): diverting colostomy first → repair the fistula after inflammation resolves → colostomy reversal after confirmed fistula healing
- Radiation-induced RVF: Successful closure reported with:
- Bulbocavernosus flaps (Martius procedure)
- Sigmoid colon transposition
- Occasionally: resection with anastomosis
- Diversion with colostomy - optimal in patients with poor pelvic vascular supply or history of anastomotic breakdown
Radiation-Induced Fistulas
Incidence
- Bowel fistula rate after pelvic radiation for cervical cancer: 1.4% to 5.3%
- VVF (vesicovaginal) is the most common urinary complication: 1% to 5% of patients
- Chronic effects result from radiation-induced vasculitis and fibrosis
- Occur months to years after radiotherapy is completed
Management Principles
- VVF after radiation: usually requires supravesical urinary diversion; occasionally a small fistula can be repaired with bulbocavernosus flap or omental pedicle
- Small bowel fistulas after radiation: rarely close spontaneously; manage with:
- Aggressive fluid replacement
- Nasogastric suction
- Wound care
- Fistulography + barium enema to exclude combined fistula
- Surgical: the fistula-containing loop of bowel may be resected or isolated in situ (acting as its own mucous fistula)
- Before any repair: always exclude recurrent cancer (especially ureteral strictures, which are usually a sign of recurrent cancer - require FNA-CT guided cytology)
Gastrointestinal Fistulas after Gynecologic Surgery
Risk Factors
- Malignancy
- Prior radiation therapy
- Intestinal resection with anastomosis
- Surgical injury improperly repaired or unrecognized
Clinical Features
- Similar to small bowel obstruction or ileus
- Fever is usually a more prominent component
- Gastrointestinal dysfunction postoperatively + fever = evaluate GI tract continuity
Diagnosis
- Water-soluble contrast (NOT barium - risk of barium peritonitis) for fistula evaluation
- Abdominal-pelvic CT scan - identifies fistula and associated abscess
Management
- Intraperitoneal fistula (peritoneal leak): requires immediate surgery
- Enterocutaneous fistula draining spontaneously through abdominal wall (no peritonitis): medical management
- Nasogastric decompression
- IV fluids replacement
- TPN (Total Parenteral Nutrition)
- Appropriate antibiotics (mixed bacterial infection)
- Somatostatin analogs - decrease intestinal secretion, allow earlier fistula healing
- Allow spontaneous closure over up to 2 weeks
- If fails: surgical correction - resection, bypass, or reanastomosis
- Rectovaginal fistula post-gynecologic surgery: manage as above (conservative first, then surgical)
Surgical Principles - Summary Table
| Parameter | Recommendation |
|---|---|
| Timing of repair (VVF) | 3-4 months after diagnosis (allow inflammation to resolve) |
| Conservative trial | 4-6 weeks catheter drainage (VVF); 15% close spontaneously |
| Surgical approach | Vaginal preferred; abdominal/laparoscopic/robotic also feasible |
| Layers of vaginal repair | 4 layers: bladder mucosa, seromuscular, endopelvic fascia, vaginal epithelium |
| Postoperative catheterization | 7-14 days |
| Large/recurrent/radiation fistulas | Martius labial fat-pad flap interpositioning |
| Large RVF | Diverting colostomy first, then repair |
| Failed VVF repair / radiation VVF | Martius flap or omental pedicle or urinary diversion |
Exam High-Yield Points
- Most common genitourinary fistula: Vesicovaginal fistula
- Most common cause worldwide: Prolonged obstructed labor (obstetric)
- Most common cause in developed countries: Hysterectomy (incidence 0.2%)
- Diagnosis of VVF: Methylene blue dye instilled into bladder; tampon stains blue
- Diagnosis of ureterovaginal fistula: Oral pyridium; tampon stains orange within 20 minutes
- Conservative treatment: Foley catheterization - 15% close spontaneously in 4-6 weeks
- Timing of surgical repair: 3-4 months (allows vascularization and reduced inflammation)
- Technique for surgical repair: 4-layer closure; minimal tension; 7-14 days postoperative catheterization
- Martius flap: Labial fat-pad/bulbocavernosus - used for large, radiation-induced, or recurrent fistulas
- Flat tire test: Air insufflated into rectum, saline in vagina - bubbling confirms RVF
- Youssef syndrome: Vesicouterine fistula after repeat cesarean section - cyclic hematuria + incontinence + amenorrhea
- Radiation fistula rate (cervical cancer): Bowel 1.4-5.3%; Urinary 1-5%
- Contrast for suspected bowel fistula: Water-soluble only (NOT barium - avoid barium peritonitis)
- TPN + somatostatin: Role in enterocutaneous fistula conservative management
- Robotic surgery: Particularly useful for VVF and RVF repair (precision, superior suturing capability)
Source: Berek & Novak's Gynecology (ISBN: 9781496380357) - Chapters on Postoperative Complications, Urogynecology, Radiation Complications, Anorectal Disorders, and Pelvic Floor Surgery
This is a shared conversation. Sign in to Orris to start your own chat.