Urinary catheterization,hematuria ,bladder cancer
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
bladder cancer hematuria catheterization
Reading File
Reading File
Reading File
Finding Sources
Searching PubMed
bladder cancer diagnosis hematuria
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a thorough, integrated review of all three topics.
Urinary Catheterization, Hematuria, and Bladder Cancer
1. Urinary Catheterization
Overview
Urinary catheterization involves inserting a tube into the bladder through the urethra (or suprapubically) to drain urine. Indications include urinary retention, peri-operative monitoring, management of urinary incontinence, and bladder irrigation for hemorrhagic conditions.
Types
- Short-term indwelling (Foley) catheter - common in acute hospital settings
- Clean Intermittent Catheterization (CIC) - preferred for long-term management (e.g., neurogenic bladder); evidence shows early initiation of CIC decreases UTI rates compared to prolonged indwelling catheter use
- Suprapubic catheter - placed through the abdominal wall, used when urethral access is contraindicated
Complications
Infection - Catheter-Associated UTI (CAUTI)
- The most common complication of indwelling catheters
- Organisms form a biofilm on the catheter surface, protecting them from urine flow, host immunity, and antibiotics
- Short-term catheters (<30 days): usually single organisms - E. coli, Klebsiella, Pseudomonas, Enterobacter, staphylococci
- Long-term catheters (>30 days): usually polymicrobial - E. coli, Proteus mirabilis, Pseudomonas, Morganella morganii, Candida spp.
- Symptoms of CAUTI include fever, rigors, altered mental status, malaise, pelvic discomfort, acute hematuria, flank pain, and costovertebral angle tenderness
- Pyuria is universal in long-term catheterized patients and should NOT be used alone to diagnose symptomatic infection in the absence of clinical symptoms
CAUTI Diagnostic Criteria by Patient Group:
| Patient Group | Diagnostic Requirements |
|---|---|
| Cystitis | New fever, rigors, suprapubic tenderness, altered mental status, acute hematuria |
| Pyelonephritis | Fever, rigors, flank pain, CVA tenderness |
| Critically ill | Fever, rigors, change in mental status |
| Spinal cord injury | Increased spasticity, autonomic dysreflexia, sense of unease |
CAUTI Management:
- Remove or replace the catheter (replace if in place >14 days)
- Asymptomatic bacteriuria in short-term catheterized patients does NOT require antibiotics (unless pregnant or urologic procedure is pending)
- Empiric antibiotics for symptomatic infection; tailor based on culture results
- 7 days if prompt resolution; 10-14 days for delayed response
- Asymptomatic candiduria does not require treatment unless immunocompromised; if symptomatic, antifungal therapy for 14 days
Traumatic Complications:
A catheter can cause:
- False passages in the urethra during insertion
- Hematuria from direct urethral or bladder irritation
- Pain or erosion at the urethral meatus
- Rarely, bladder perforation (sometimes accompanied by bowel perforation with chronic indwelling catheter)
- Nontotal deflation of the balloon during removal can cause urethral trauma
Catheter-Related Risk of Bladder Cancer:
Chronic foreign bodies, including catheters, are a recognized risk factor for bladder cancer - specifically squamous cell carcinoma of the bladder. This is seen in paraplegic patients with chronic indwelling catheters. Squamous cell carcinoma accounts for 5-10% of all bladder cancers in the United States and is often associated with chronic infection, vesical calculi, or chronic catheter use.
Campbell Walsh Wein Urology and Tintinalli's Emergency Medicine
2. Hematuria
Definition
- Gross hematuria: blood visible to the patient or physician
- Microscopic hematuria: ≥3 RBCs/hpf on urinalysis in adults; >5 RBCs/hpf on two weekly samples in children
- The urine dipstick alone is insufficient - it can be positive without RBCs present (pseudohematuria from myoglobin, certain foods/medications). A midstream clean-catch microscopy is required to confirm true hematuria
Clinical Significance
- Hematuria may signal a urologic cancer in up to 25% of patients
- The most common cause of gross hematuria in patients older than 50 years is bladder cancer
- The malignancy rate in screening studies for microhematuria is approximately 2.6%
- 61% of patients with hematuria have no significant pathology found after evaluation
Localization by Timing
The portion of the urinary stream affected provides diagnostic clues:
- Initial stream hematuria - mild bleeding from prostatic or urethral source
- Total stream hematuria - upper tract or diffuse bladder source
- Terminal hematuria - bladder neck irritation, expressed at end of urination (e.g., bladder cancer, prostatitis)
Clot Morphology
- Vermiform (worm-shaped) clots - origin in the upper urinary tract (ureter/renal pelvis)
- Cuboid clots - formed within the bladder
Differential Diagnosis
| Category | Causes |
|---|---|
| Malignancy | Bladder cancer, renal cell carcinoma, urothelial carcinoma of upper tract |
| Urologic | Urolithiasis, BPH, trauma, urethral stricture |
| Infectious | UTI (cystitis, pyelonephritis), schistosomiasis |
| Renal/Nephrologic | Glomerulonephritis, IgA nephropathy, thin basement membrane disease |
| Iatrogenic | Catheter trauma, recent urologic procedure, anticoagulation |
| Other | Cyclophosphamide (hemorrhagic cystitis), radiation cystitis |
Risk Factors Mandating Full Urologic Evaluation
- Age >50 years
- Smoking history
- Occupational exposure to aromatic amines, benzidine, rubber/dye industries
- Alkylating chemotherapy (cyclophosphamide)
- Analgesic abuse
- Chronic foreign body in urinary tract (catheter, stone)
- History of pelvic radiation
Evaluation
After excluding UTI (particularly in young women), nephrologic pathology, trauma, or recent urologic manipulation:
- Urine cytology - detects cancer in only ~50% of high-grade bladder cancers
- Cystoscopy - direct visual examination of the bladder; the most effective means to diagnose bladder cancer
- CT urogram - evaluates kidneys and upper urinary tract
- MR urogram - substitute in patients with poor renal function
- Fluorescent in situ hybridization (FISH) - detects cancer-associated chromosomal changes in urine; useful for recurrence surveillance
- Blue light cystoscopy / Narrow-band imaging cystoscopy - improve detection of small and flat (non-invasive) tumors; now used routinely in bladder cancer surveillance
- Ureteroscopy or retrograde pyelography - when upper tract tumors are suspected with no bladder findings
Campbell Walsh Wein Urology, Harrison's Principles of Internal Medicine 22E, Textbook of Family Medicine 9e
3. Bladder Cancer
Epidemiology
- ~81,190 new diagnoses per year in the US
- Men have 3x the incidence of women
- Incidence in white men is 2x that of African American men
- Over 700,000 Americans live with bladder cancer
- Highly recurrent disease
Risk Factors
| Risk Factor | Details |
|---|---|
| Tobacco smoking | Single most important risk factor; 4-7x increased risk; 90% of bladder cancer diagnoses occur in current or former smokers |
| Aromatic amines | Benzidine, β-naphthylamine in dyes, rubber, leather, paint, printing industries |
| Arsenic | Contaminated drinking water in developing countries |
| Cyclophosphamide | Alkylating agent - acrolein metabolite causes hemorrhagic cystitis and urothelial cancer |
| Pelvic radiation | |
| Chronic catheterization | Leads to squamous cell carcinoma in paraplegic patients |
| Schistosoma haematobium | Endemic in Egypt, Africa, Middle East - causes squamous cell carcinoma (60% of bladder cancers in affected regions) |
| Pioglitazone | Small increased risk with long-term use |
| Aristolochic acid | Found in some herbal supplements |
Histology
- Urothelial carcinoma (transitional cell carcinoma) - 90% of cases; best prognosis
- Squamous cell carcinoma - 5-10%; associated with chronic infection, calculi, catheter use, schistosomiasis
- Adenocarcinoma - 1-2%; primary or urachal origin
- Small cell/undifferentiated carcinoma - <1%; aggressive, usually presents with metastases
Histopathology Images
Figure A: Normal urothelium (125x)
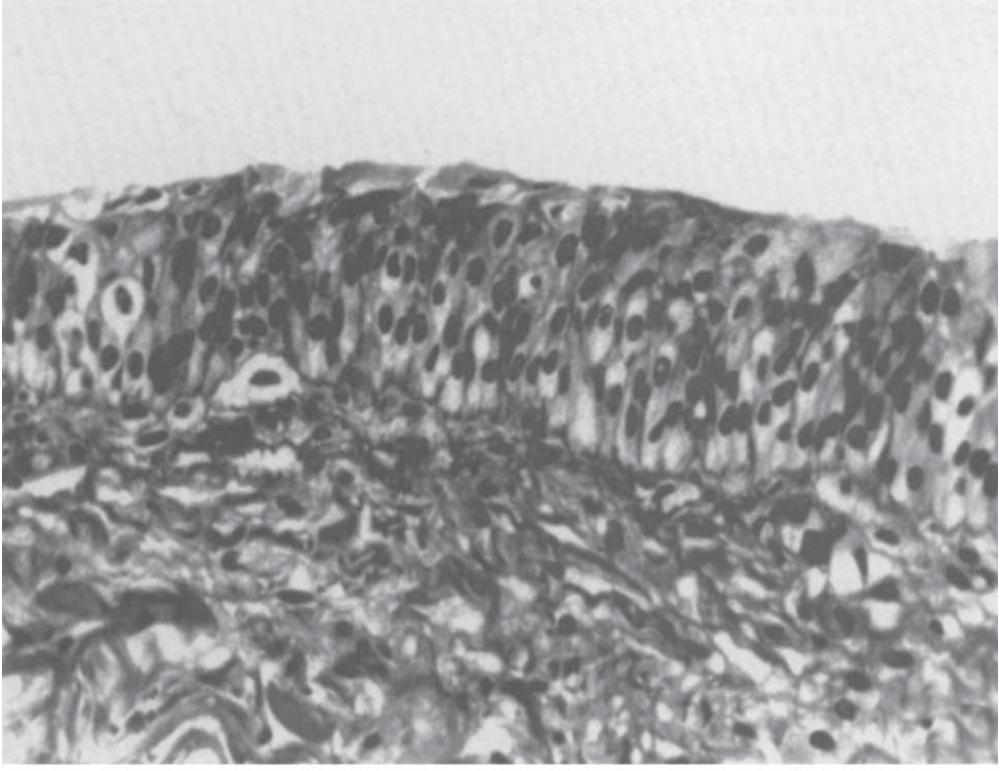
Figure B: Moderately well differentiated papillary bladder cancer (60x)
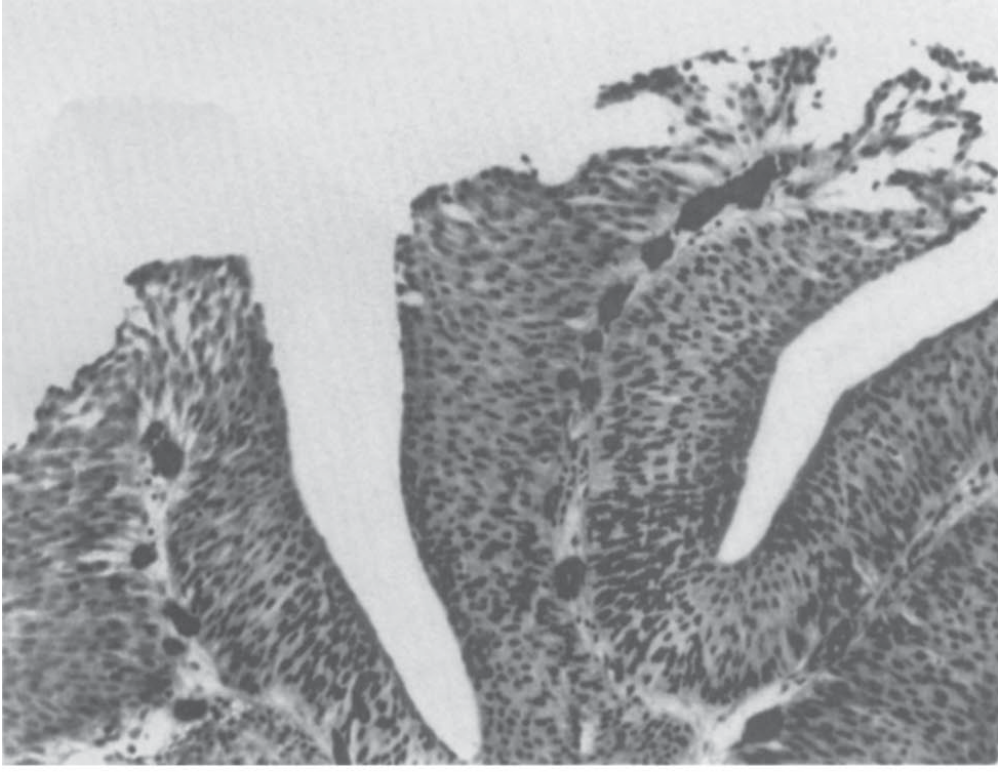
Figure C: Carcinoma in situ (CIS) (200x)
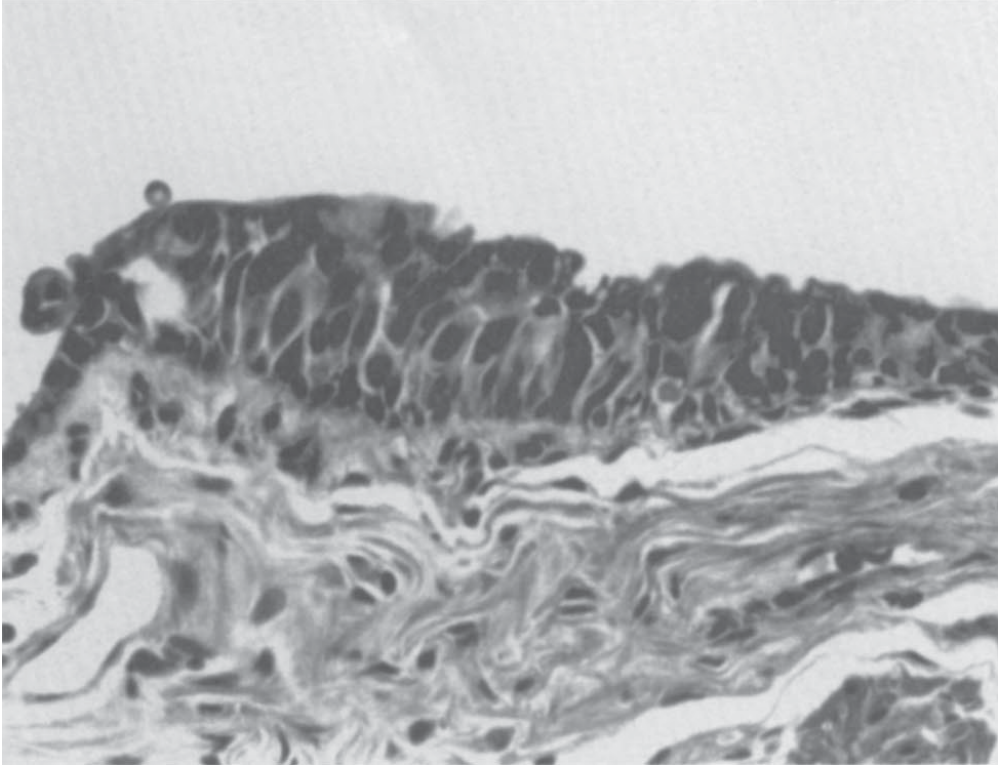
Smith and Tanagho's General Urology, 19th Edition
Clinical Presentation
- Painless gross or microscopic hematuria - most common initial sign (present in virtually all cases)
- Irritative voiding symptoms: urgency, frequency, dysuria
- In women, hematuria due to malignancy can be mistaken for UTI or menstrual bleeding
- Flank pain if the tumor obstructs a ureteral orifice or if upper tract cancer is present
- Rarely: cachexia and widespread metastatic disease at presentation
Staging (TNM)
| Stage | Description | 5-Year Survival |
|---|---|---|
| Ta | Non-invasive papillary carcinoma | ~90-95% |
| Tis (CIS) | Flat carcinoma in situ | High grade; risk of progression |
| T1 | Lamina propria invasion | 80-88% (NMIBC combined) |
| T2 | Muscle (detrusor) invasion | 53-80% |
| T3 | Perivesical fat invasion | 39-68% |
| T4 | Adjacent organ invasion (prostate, uterus, vagina, pelvic/abdominal wall) | 25-40% |
- 75-85% of cases are non-muscle-invasive (NMIBC) at diagnosis (stages Ta, Tis, T1)
- ~25% present with invasive or metastatic disease with no prior bladder cancer history
- Lymphovascular invasion even in node-negative disease is a poor prognostic factor
Staging Workup
- TURBT (Transurethral Resection of Bladder Tumor) - includes examination under anesthesia (EUA), samples muscle wall to assess depth of invasion
- CT scan (chest/abdomen/pelvis) - assess nodal and visceral metastasis
- CT urography - evaluate upper urinary tracts
- Bone scan - only if bone pain, known advanced disease, or elevated alkaline phosphatase
- Restaging TURBT within 2-6 weeks if initial resection was incomplete or uncertain - especially important for Tis, Ta, T1, and T2 disease considered for bladder preservation
AUA Risk Stratification of NMIBC
| Low Risk | Intermediate Risk | High Risk |
|---|---|---|
| PUNLMP; single low-grade Ta ≤3 cm | Single low-grade Ta >3 cm; low-grade Ta recurrent within 1 year; multifocal low-grade Ta; primary high-grade Ta ≤3 cm; low-grade T1 | Any CIS; high-grade T1; high-grade Ta >3 cm (or multifocal); recurrent high-grade Ta; BCG failure; variant histology; lymphovascular invasion; prostatic urethral involvement |
Treatment
Non-Muscle-Invasive Bladder Cancer (NMIBC)
- Low-risk: TURBT alone + single immediate post-operative instillation of intravesical chemotherapy
- Intermediate-risk: TURBT + immediate intravesical chemotherapy + subsequent intravesical chemotherapy or BCG immunotherapy
- High-risk: TURBT + intravesical BCG immunotherapy; if BCG failure, radical cystectomy is warranted
- Recurrence rates after TURBT: 50-70% - hence adjuvant intravesical therapy is standard
- Intravesical chemotherapy (e.g., mitomycin C) reduces recurrence by 44-73% vs. TURBT alone
- BCG reduces recurrence by >50% vs. TURBT alone
Muscle-Invasive Bladder Cancer (MIBC - T2+)
- Radical cystectomy is the standard of care for T2-T4 resectable disease
- Neoadjuvant cisplatin-based chemotherapy before cystectomy improves survival
- Bladder preservation with trimodal therapy (maximal TURBT + radiation + concurrent chemotherapy) is an option in select patients
- For metastatic disease: cisplatin-based combination chemotherapy (e.g., gemcitabine + cisplatin)
- Checkpoint inhibitors (pembrolizumab, atezolizumab) are now used for cisplatin-ineligible patients and in the maintenance setting
Genetics and Molecular Biology
- FGFR3 mutations - common in low-grade papillary Ta tumors
- TP53 and RB1 alterations - associated with high-grade and muscle-invasive disease
- GWAS susceptibility loci identified: 8q24.21 (near MYC), 3q28 (TP63), 5p15.33 (hTERT), PSCA at 8q24.3, NAT2, UGT1A, GSTM1, and others
- Telomere dysfunction is implicated in chromosomal instability and cancer progression
Campbell Walsh Wein Urology, Schwartz's Principles of Surgery 11e, Smith & Tanagho's General Urology 19e, Harrison's Principles of Internal Medicine 22E
The Triangle: Catheter - Hematuria - Bladder Cancer
These three topics intersect clinically in several important ways:
-
Catheter as cause of hematuria: Direct urethral or bladder irritation by a catheter causes hematuria. This is usually transient and mild but requires distinction from other causes, especially in at-risk patients.
-
Catheter-associated hematuria vs. cancer: When a catheterized patient develops hematuria, clinical context matters. Acute hematuria in a CAUTI setting has characteristic features (fever, altered mental status), whereas tumor-related hematuria is typically painless and may be intermittent. If hematuria persists after catheter removal and resolution of infection, full urologic evaluation (cystoscopy, CT urogram) is warranted.
-
Chronic catheter use as a carcinogen: Prolonged indwelling catheterization (especially in paraplegic patients) causes chronic mucosal irritation and inflammation, predisposing to squamous cell carcinoma of the bladder. These tumors are often nodular and already invasive at diagnosis.
-
Bladder cancer causing need for catheterization: Large bladder tumors obstructing the bladder outlet or causing massive hemorrhagic cystitis with clot retention may require catheterization - including three-way catheters for continuous bladder irrigation (CBI). Note that clots can obstruct an indwelling catheter.
-
Hematuria as the bridge: Hematuria is the unifying symptom - it is the cardinal presenting sign of bladder cancer AND a complication of catheterization AND a feature of CAUTI. Accurately characterizing hematuria in a catheterized patient requires careful clinical reasoning.
Recent Evidence (2024-2026)
A 2026 meta-analysis (PMID 41520313) compared hyperthermic intravesical chemotherapy vs. BCG in NMIBC, finding comparable or superior efficacy with heat-enhanced chemotherapy - an emerging alternative in BCG-shortage settings.
Sources: Campbell Walsh Wein Urology (3-Volume Set), Smith & Tanagho's General Urology 19e, Schwartz's Principles of Surgery 11e, Harrison's Principles of Internal Medicine 22E, Tintinalli's Emergency Medicine, Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.