Pelvic endometriosis with bilateral endometrioma detailed overview,pathophysiology according to comprehensive gynecology 8th edition
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from Berek & Novak's Gynecology. Let me compile the complete, detailed overview based on all the content I've gathered.
Pelvic Endometriosis with Bilateral Endometrioma: Detailed Overview
Primary source: Berek & Novak's Gynecology (the leading comprehensive gynecology reference in the library). Note: Comprehensive Gynecology 8th ed. by Lobo et al. was not available in the library; the content below draws from Berek & Novak's Gynecology, which covers identical material and is considered equivalent in scope and authority.
Definition
Endometriosis is a disorder in which endometrial glands and stroma are found outside the uterine cavity. The most common pelvic sites are the ovaries, cul-de-sac, and pelvic visceral/parietal peritoneum. When endometriotic cysts form within the ovary, they are called endometriomas (colloquially "chocolate cysts"). Bilateral endometriomas signify significant ovarian disease in the context of usually widespread pelvic involvement.
- Occurs in approximately 10% of the general female population
- Found in 15-20% of infertile women
- Found in >30% of women with chronic pelvic pain (CPP)
- Exclusive ovarian disease is found in only 1% of endometriosis patients - the vast majority with ovarian endometriomas also have extensive pelvic or intestinal disease
Pathophysiology / Etiology
Endometriosis is an estrogen-dependent disease. Three classical theories explain its pathogenesis, though no single theory accounts for all anatomic locations.
1. Transplantation Theory (Sampson's Theory)
Originally proposed by Sampson in the mid-1920s. Based on the assumption that endometriosis results from retrograde menstruation - the seeding and implantation of endometrial cells via transtubal regurgitation during menstruation.
- Retrograde menstruation occurs in 70-90% of women, and appears more common in women with endometriosis than without
- Endometrial cells are demonstrable in peritoneal fluid during menstruation
- This theory explains why endometriosis predominantly affects pelvic peritoneum, ovaries, and cul-de-sac (dependent areas hit by retrograde flow)
- Substantial clinical and experimental data support this hypothesis
However, the theory does not explain why most women with retrograde menstruation do not develop endometriosis, nor does it explain extrapelvic disease (e.g., pleural, diaphragm, and umbilical sites).
2. Coelomic Metaplasia Theory
Proposes that the peritoneal mesothelium undergoes metaplastic transformation into endometrial tissue, possibly triggered by hormonal or inflammatory stimuli. This theory helps explain endometriosis in anatomic locations unreachable by retrograde flow (e.g., pleura, pericardium).
3. Induction Theory
A combination of the above - circulating endometrial factors induce undifferentiated mesenchymal cells to form endometriotic tissue. This is essentially an extension of the metaplasia theory with a biochemical trigger.
Genetic Factors
- Endometriosis has a polygenic/multifactorial inheritance pattern
- First-degree relatives of affected women have a significantly increased risk (6-9x higher in some studies)
- Both germline variants (susceptibility loci identified by GWAS) and somatic alterations (mutations accumulating in ectopic tissue) contribute
- Somatic mutations, including those in tumor suppressor genes, explain the malignant transformation potential in a small subset
Immunologic Factors and Inflammation
- Women with endometriosis have altered peritoneal immunity: increased activated macrophages, elevated peritoneal fluid prostaglandins, IL-1, IL-6, IL-8, TNF-alpha, and VEGF
- Deficient NK cell cytotoxicity - normally NK cells would destroy ectopic endometrial cells; in endometriosis, this surveillance is impaired
- This immune defect allows retrograde endometrial cells to implant and survive
- Once established, implants produce prostaglandin E and F2α - petechial/red "flame" lesions (early disease) produce significantly more prostaglandins than the classic "powder-burn" black lesions of advanced disease
- Cytokines and prostaglandins contribute to the local inflammatory milieu promoting implant survival, neoangiogenesis, and pain
Role of Estrogen
- Ectopic endometrial implants are estrogen-dependent for growth and survival
- Local aromatase activity within endometriotic tissue converts androgens to estradiol, creating an autonomous estrogen source
- This is the rationale for all medical therapies targeting estrogen suppression
Neural Innervation and Pain Sensitization
- Endometriotic implants acquire a vascular and nerve supply, contributing to peripheral sensitization
- Nerve fiber density is increased in both ectopic and eutopic endometrium of affected women
- This peripheral neurogenic inflammation triggers central sensitization over time - explaining why pain can persist even after surgical removal, and why the severity of pain does not correlate with stage of disease
- Deeply infiltrating lesions (>5 mm below peritoneal surface) penetrate rich nerve endings in the cul-de-sac and uterosacral ligaments - strongly associated with pain
Stem Cells
- Recent research implicates bone marrow-derived stem cells and endometrial stem/progenitor cells in the establishment of ectopic implants, potentially explaining spread to distant sites
Environmental Factors
- Dioxin and polychlorinated biphenyls (PCBs) have been linked to endometriosis in primate models and human data, potentially through immune modulation and estrogen receptor interactions
Types / Anatomic Classification
1. Peritoneal Endometriosis
Classic findings on laparoscopy include:
- Powder-burn / gunshot lesions: black, dark brown, or bluish nodules or small cysts containing old hemorrhage surrounded by fibrosis - typical of longstanding disease
- Subtle/early lesions: red flame-like implants, petechial vesicles, clear/serous vesicles, white plaques or scarring, yellow-brown peritoneal discoloration
- Peritoneal windows (Allen-Masters defects)
2. Ovarian Endometriosis (Endometrioma)
The most relevant category for bilateral endometriomas:
- Superficial ovarian lesions may be typical or subtle
- Larger ovarian endometriotic cysts (endometriomas) are usually located on the anterior surface of the ovary
- Associated with retraction, pigmentation, and adhesions to the posterior peritoneum/pelvic sidewall/posterior uterus/cul-de-sac
- Contain thick, viscous dark brown "chocolate fluid" composed of hemosiderin from previous intraovarian hemorrhage
- Diagnosis confirmed when: cyst diameter <12 cm, adhesion to pelvic sidewall or broad ligament, endometriosis on ovarian surface, tarry chocolate-colored fluid content
- Because similar fluid can be found in hemorrhagic corpus luteum cysts or neoplastic cysts, biopsy and histologic confirmation are required per ASRM classification criteria
- Ovarian endometriosis is a marker for more extensive pelvic and intestinal disease - exclusive ovarian disease in only 1% of cases
3. Deep Infiltrating Endometriosis (DIE)
- Defined as endometriosis infiltrating >5 mm below the peritoneal surface
- Usually located in the posterior cul-de-sac, uterosacral ligaments, rectovaginal septum, and rectum
- May be detected only by palpation beneath visually normal peritoneum
- Deep lesions can create a "frozen pelvis" with obliteration of the cul-de-sac
- Mild forms can appear as minimal disease at laparoscopy, leading to underestimation
- Reduced cul-de-sac size suggests lesions develop intraperitoneally with burial of anterior rectal wall adhesions
4. Extrapelvic Endometriosis
Bowel, ureters, bladder, diaphragm, pleural cavity (catamenial pneumothorax), umbilicus
Risk Factors
| Risk Factors | Protective Factors |
|---|---|
| Early menarche | Multiparity |
| Short menstrual cycle / hypermenorrhea | Lactation |
| Nulliparity | Higher BMI |
| Müllerian anomalies | Diet high in vegetables/fruit |
| Family history (first-degree relative) | Tobacco exposure in utero |
| Tall stature | |
| Low birth weight | |
| DES exposure | |
| Dioxin/PCB exposure | |
| Diet high in fat and red meat |
Clinical Presentation
Symptoms
- Severe dysmenorrhea - cyclic pelvic pain beginning up to 2 weeks before menses
- Deep thrust dyspareunia (posterior cul-de-sac / uterosacral involvement)
- Chronic pelvic pain (non-cyclic)
- Subfertility / infertility
- Dyschezia - cyclic, with posterior cul-de-sac/bowel involvement
- Urinary urgency, frequency, cyclic hematuria (bladder/ureteral involvement)
- Cyclic bloating, abdominal distension
- Cyclic catamenial pneumothorax, hemothorax, shoulder pain (thoracic/diaphragmatic)
- Irregular uterine bleeding despite ovulatory cycles
Important: There is no correlation between disease stage and pain severity - 30-50% of patients have no pain regardless of stage, and 40-60% have no tenderness on examination regardless of stage.
Signs on Examination
- Uterosacral nodularity on bimanual/rectovaginal exam
- Fixed retroverted uterus (fibrosis)
- Lateral or cervical displacement from uterosacral scarring
- Fullness/cystic mass consistent with endometrioma on bimanual exam
- Focal uterosacral or broad ligament tenderness
- Reduced ovarian/tubal mobility ("frozen pelvis" in advanced disease)
- Pinpoint/stenotic cervical os
Endocrinologic Abnormalities Associated
- Anovulation
- Abnormal follicular development and impaired follicle growth
- Reduced circulating E2 during preovulatory phase
- Disturbed LH surge patterns
- Luteinized unruptured follicle (LUF) syndrome
- Premenstrual spotting
- Hyperprolactinemia, galactorrhea
Diagnosis
Non-surgical / Clinical Diagnosis
- Clinical diagnosis is accurate in only ~50% of cases
- Ultrasound: Homogeneous hemorrhagic-appearing cysts (ground-glass echogenicity) that fail to resolve after 1-2 menstrual cycles are suspicious for endometriomas; distinguishable from hemorrhagic corpus lutea by persistence
- CA-125: Can be elevated but is a non-specific, non-sensitive marker; useful in some contexts for monitoring rather than diagnosis
- MRI and other advanced imaging can assist for deep infiltrating disease
Definitive (Surgical) Diagnosis
- Made by direct operative visualization - laparoscopy (preferred) or laparotomy
- Histologic confirmation is essential
- Active red flame/vesicular lesions indicate early disease; powder-burn fibrotic lesions suggest longstanding disease
- Histologically negative biopsies of typical-appearing lesions occur in 24% of cases
- Deep infiltrating lesions and peritoneal windows are most commonly found in the posterior cul-de-sac at uterosacral ligaments
Laparoscopic Classification (ASRM)
Staging: minimal (stage I), mild (stage II), moderate (stage III), severe (stage IV) - based on size/depth of implants, adhesion extent, and endometrioma involvement. Bilateral endometriomas = at minimum stage III-IV.
Specific Considerations for Bilateral Endometrioma
- Bilateral endometriomas almost always indicate stage III or IV disease with extensive pelvic involvement
- Associated with significant adhesions to the posterior uterus, cul-de-sac, pelvic sidewalls, and in many cases the bowel
- The close attachment of the endometrioma to the ovarian cortex and stroma makes finding surgical dissection planes difficult
- Incomplete removal significantly increases the risk of recurrence
- Impact on ovarian reserve: bilateral disease and/or bilateral surgical excision poses a risk to the antral follicle count and oocyte yield for IVF
Management
Medical Treatment (Pain-focused)
- NSAIDs: First-line for dysmenorrhea
- Combined oral contraceptives (COCs): Continuous or cyclic; suppress endometriotic growth
- Progestins: Continuous progestins (MPA, norethindrone acetate, dienogest) - suppress ectopic implants via decidualization and atrophy
- GnRH agonists (leuprolide, nafarelin): Induce hypoestrogenic state ("medical oophorectomy"); effective for pain but cause bone loss with long-term use; add-back therapy required
- GnRH antagonists (elagolix, relugolix): Newer; dose-dependent estrogen suppression with more rapid onset and offset
- Aromatase inhibitors: Used in refractory cases given the local estrogen production by ectopic tissue
- Levonorgestrel IUD: Provides local progestin effect
Surgical Treatment
Peritoneal disease:
- Lesions removed by excision with scissors, bipolar coagulation, or laser (CO2, KTP, or argon)
- Surgical ablation and excision are considered equally effective for peritoneal disease
- Excision preferred because it allows histologic confirmation
Ovarian Endometrioma - the key controversy:
- Two main approaches: (1) Cystectomy (excision of cyst wall) or (2) Drainage and ablation of cyst wall
- Cochrane systematic review evidence strongly favors cystectomy:
- Reduced recurrence of endometrioma (OR 0.41)
- Reduced recurrence of dysmenorrhea (OR 0.15), dyspareunia (OR 0.08), non-menstrual pelvic pain (OR 0.10)
- Reduced need for further surgery (OR 0.21)
- Increased spontaneous pregnancy rate in previously infertile women (OR 5.21)
- ESHRE guideline: Recommends cystectomy over drainage and coagulation
- For very large endometriomas where excision risks removing a large portion of the ovary: a three-step procedure can be considered - marsupialization and rinsing, followed by hormonal treatment with GnRH analogs, then cyst wall electrocoagulation/laser vaporization 3 months later
- Ovarian hemostasis after cystectomy: intraovarian suturing results in lower postoperative adhesion rates compared to bipolar coagulation alone
Deep endometriosis:
- Usually multifocal; complete surgical excision in a single procedure is critical
- Requires skilled retroperitoneal dissection to protect ureters and bowel
- Multidisciplinary approach (urologic + colorectal surgeons) often needed for severe disease
Definitive surgery:
- Bilateral salpingo-oophorectomy ± hysterectomy: Reserved for patients who fail conservative surgical and medical therapy; provides significant pain relief to the majority
- At hysterectomy for endometriosis, conserving normal-appearing ovaries should be considered
- Post-oophorectomy: risk of recurrence if estrogen replacement given without progestin in the setting of residual disease
Fertility Management with Bilateral Endometrioma
- Endometriosis is strongly associated with infertility via multiple mechanisms: mechanical (adhesions, tubal distortion), endocrinologic, peritoneal inflammatory milieu, impaired folliculogenesis, and possible endometrial receptivity defects
- Endometriomas can reduce ovarian reserve; surgical excision may further reduce it
- IVF outcomes in women with endometriomas: may be reduced due to the inflammatory effects on oocyte quality
- Decision to excise endometriomas prior to IVF vs. proceeding directly to IVF is individualized
Endometriosis and Cancer Risk
- Modest increased risk of endometrioid and clear-cell ovarian cancer (OR 1.3-1.9) - the only well-established cancer association
- No increased risk for other gynecologic cancers
- Possible association with melanoma and non-Hodgkin lymphoma - unconfirmed
- Ectopic endometrium undergoes malignant transformation at a frequency similar to its eutopic counterpart - the low absolute risk makes routine cancer surveillance of endometriomas beyond standard ultrasound unnecessary
- Endometriosis should not be considered a clinically significant cancer-associated condition
Endometriosis-Related Pain Syndrome
A newer concept for pain unresponsive to adequate medical and surgical therapy (especially in minimal/mild disease):
- Neural plasticity - central sensitization initiated by the peripheral inflammatory insult
- The disease is no longer just the endometriosis itself, but is perpetuated by alterations in peripheral and CNS pain processing
- Frequently co-existent ("comorbid") with IC/PBS, IBS, myofascial pain, fibromyalgia, vulvodynia, and anxiety disorders
- These conditions must be managed concurrently
Sources: Berek & Novak's Gynecology - Chapter 13 (Endometriosis: Vanhie & D'Hooghe), Chapter 11 (Pelvic Pain / Endometriosis), and Chapter 26 (Laparoscopic Management of Endometriomas); Robbins & Kumar Basic Pathology (endometriosis pathology); Goodman & Gilman's Pharmacological Basis of Therapeutics (medical management).
Note on source: Comprehensive Gynecology 8th edition (Lobo, Gershenson, Lentz, Valea) was not available in this library. The above content comes primarily from Berek & Novak's Gynecology, which is equivalent in authority and coverage depth for this topic, and covers the same pathophysiological frameworks (Sampson's transplantation theory, coelomic metaplasia, induction theory, immunologic dysregulation, estrogen dependency) that Comprehensive Gynecology 8th ed. presents.
Pathophysiology of the Pelvic endometriosis with bilateral endometrioma in a digramactic manner for as to add it in my ppt
Generating Image
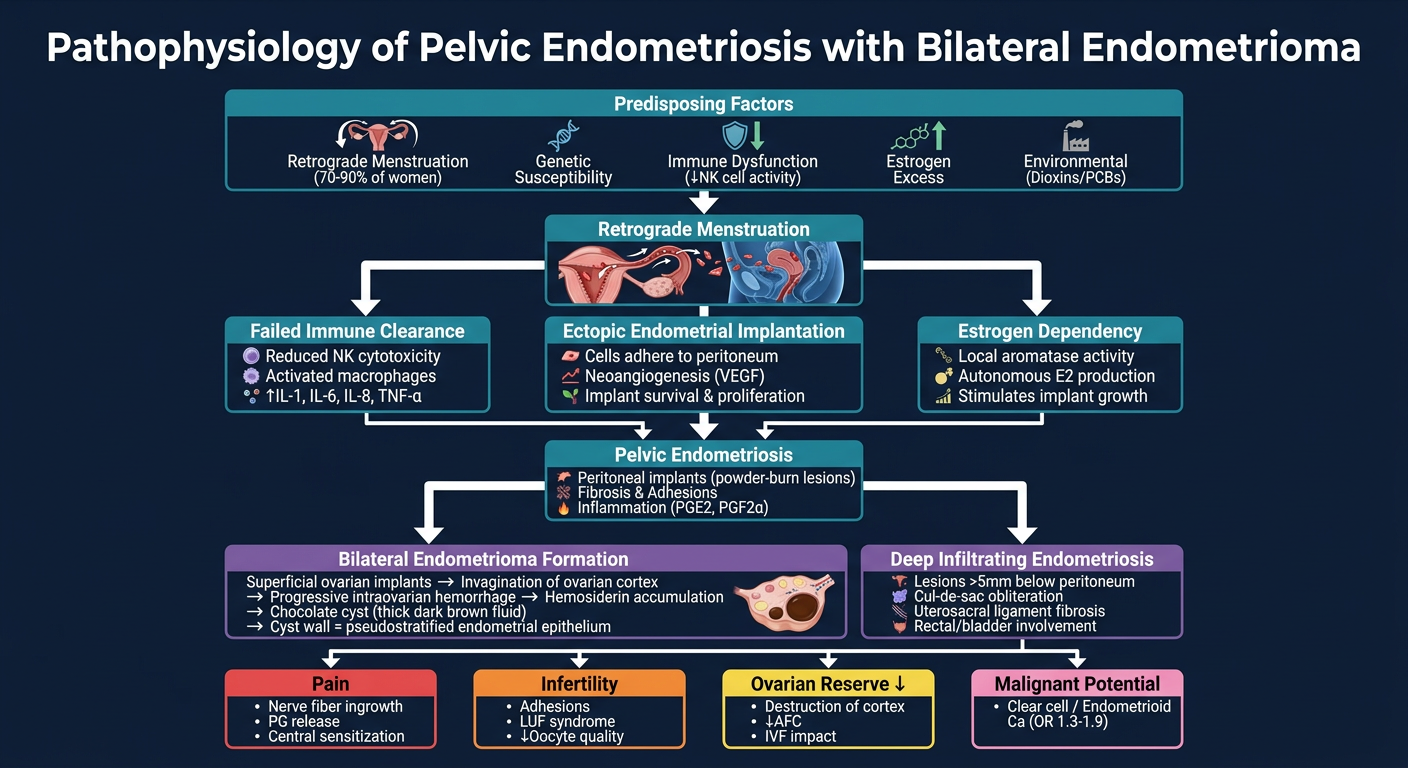
Here is your PPT-ready pathophysiology diagram. It flows top to bottom through the complete cascade:
- Predisposing Factors - retrograde menstruation, genetic susceptibility, immune dysfunction, estrogen excess, environmental triggers
- Retrograde Menstruation - endometrial cells entering the pelvis via the fallopian tubes
- Three parallel mechanisms - failed immune clearance (↓NK cytotoxicity, elevated cytokines), ectopic implantation (VEGF-driven neoangiogenesis), and estrogen dependency (local aromatase activity)
- Pelvic Endometriosis - peritoneal implants, fibrosis, prostaglandin-mediated inflammation
- Bilateral Endometrioma Formation - the complete sequence from ovarian implantation → cortical invagination → intraovarian hemorrhage → hemosiderin accumulation → "chocolate cyst" formation
- Four clinical outcomes - Pain, Infertility, Reduced Ovarian Reserve, and Malignant Potential
The dark navy background and color-coded boxes are optimized for direct use in a PowerPoint slide. If you'd like any changes - different color scheme, white background, added text, or a simplified version - just let me know.
This is a shared conversation. Sign in to Orris to start your own chat.