Classification and complications of fractures. Splint and tractions.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have sufficient content from multiple authoritative sources. Let me compile the comprehensive answer.
Classification and Complications of Fractures — Splints and Traction
1. Classification of Fractures
1.1 Purpose of Classification
Fracture classification serves four core purposes: communication (common language among clinicians), treatment and prognosis guidance, research (grouping fractures for outcome analysis), and education of trainees. A good classification must demonstrate both reliability (reproducibility between observers, measured by the Kappa statistic) and validity (correlation with clinically meaningful outcomes).
— Rockwood and Green's Fractures in Adults, 10th ed. 2025
1.2 By Skin Integrity
| Type | Description |
|---|---|
| Closed (simple) | Skin over fracture intact |
| Open (compound) | Bone communicates with outside environment through a skin wound |
Gustilo–Anderson Classification of Open Fractures
| Grade | Description |
|---|---|
| I | Wound <1 cm, clean; simple fracture pattern |
| II | Wound 1–10 cm, minimal contamination |
| IIIA | Wound >10 cm with adequate soft tissue coverage |
| IIIB | Extensive soft tissue loss requiring flap coverage |
| IIIC | Any open fracture with arterial injury requiring repair |
— Rockwood and Green's Fractures in Adults, 10th ed. 2025
1.3 By Fracture Pattern (OTA/AO 2018 Compendium)
The OTA/AO alphanumeric classification first identifies which bone is fractured, then which segment (using the "rule of squares" — the end segments are defined by a square equal in width to the widest part of the epiphysis/metaphysis): proximal = 1, diaphyseal = 2, distal = 3.
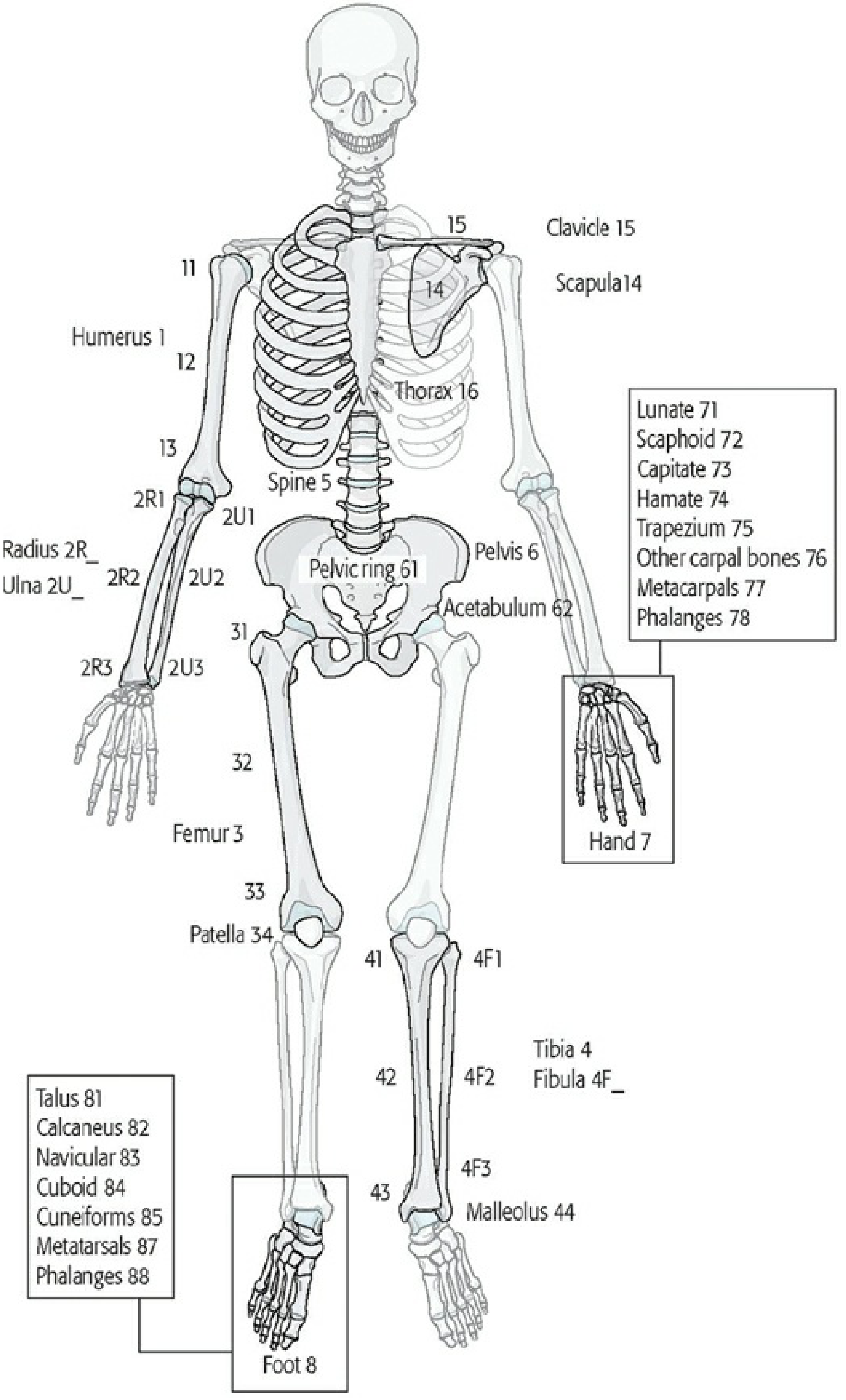
OTA/AO fracture classification scheme — bone and segment identification. (Rockwood & Green's)
Diaphyseal Fracture Morphology
| Code | Type | Description |
|---|---|---|
| A | Simple | Single fracture line, contact between fragments after reduction |
| B | Wedge | A third "butterfly" fragment; main fragments retain some contact |
| C | Multifragmentary (comminuted) | No contact between main fragments after reduction |
End-Segment (Metaphyseal / Epiphyseal) Morphology
| Code | Type |
|---|---|
| A | Extra-articular |
| B | Partial articular (part of articular surface involved) |
| C | Complete articular (epiphysis completely separated from metaphysis) |
Within each type, sub-groups (1, 2, 3) describe increasing severity.
1.4 Descriptive / Traditional Classification Terms
| Descriptor | Meaning |
|---|---|
| Transverse | Fracture line perpendicular to bone axis |
| Oblique | Fracture line at an angle |
| Spiral | Twisting force produces helical fracture line |
| Comminuted | Three or more fragments |
| Impacted | Fragments driven into each other |
| Avulsion | Fragment pulled off by ligament/tendon |
| Stress / fatigue | Repeated sub-threshold loading |
| Pathological | Through abnormal (e.g. neoplastic) bone |
| Greenstick | Incomplete fracture in children (cortex on one side intact) |
| Torus (buckle) | Cortex buckles, no complete break — children |
1.5 By Displacement and Alignment
- Undisplaced vs. displaced (translation, angulation, shortening, rotation)
- Angulation described by direction the apex points (volar, dorsal, varus, valgus)
2. Complications of Fractures
2.1 Immediate Complications
| Complication | Key Points |
|---|---|
| Hemorrhage | Blood loss 100 mL (small bones) → 2–3 L (femur, pelvis); pelvic fractures risk exsanguination and DIC |
| Neurovascular injury | Neurapraxia (contusion, recovers weeks–months), axonotmesis (crush, slower recovery), neurotmesis (severed, requires surgical repair) |
| Vascular injury | Especially knee dislocation (popliteal artery), ankle dislocation; loss of pulses requires urgent reduction; late complications include thrombosis, arteriovenous fistula, false aneurysm |
Nerve injuries associated with specific fractures:
| Fracture/Dislocation | Nerve at Risk |
|---|---|
| Elbow injury | Median or ulnar nerve |
| Shoulder dislocation | Axillary, musculocutaneous nerve |
| Sacral fracture | Cauda equina |
| Acetabular fracture | Sciatic nerve |
| Hip dislocation | Femoral nerve |
| Femoral shaft fracture | Peroneal nerve |
| Knee dislocation | Tibial or peroneal nerve |
| Lateral tibial plateau | Peroneal nerve |
2.2 Early Complications
| Complication | Description |
|---|---|
| Compartment syndrome | Increased pressure within fascial compartment → circulatory compromise, muscle necrosis, nerve damage. Surgical emergency — fasciotomy required. Classic signs: pain disproportionate to injury, pain with passive stretch, tense compartment |
| Fat embolism syndrome | Fat globules enter circulation from medullary canal; presents 24–72 h post-injury with hypoxia, petechiae, confusion |
| Infection / osteomyelitis | Risk highest with open fractures; requires debridement and antibiotics |
| Wound breakdown / skin necrosis | Particularly at risk in high-energy injuries and after tight casting |
2.3 Late / Delayed Complications
| Complication | Description |
|---|---|
| Malunion | Fracture heals in abnormal position (angulation, rotation, shortening) |
| Nonunion | Failure of healing; hypertrophic (adequate vascularity, poor stability) or atrophic (poor vascularity) |
| Delayed union | Healing slower than expected, but not yet nonunion |
| Avascular necrosis (AVN) | Loss of blood supply to bone; particularly femoral head (hip fractures), scaphoid, capitate |
| Post-traumatic arthritis | Especially with intra-articular fractures |
| Joint stiffness | Prolonged immobilization |
| Reflex sympathetic dystrophy (CRPS) | Chronic pain, autonomic changes, allodynia |
| Osteomyelitis | Late infection, particularly in open fractures or after operative fixation |
| Volkmann's ischemic contracture | End-stage of missed compartment syndrome — forearm muscles replaced by fibrous tissue |
— Tintinalli's Emergency Medicine, Roberts and Hedges' Clinical Procedures in Emergency Medicine
3. Splinting
3.1 Principles of Splinting
Splints allow for post-injury swelling, unlike circumferential casts. General principles:
- Administer analgesia before application
- Remove clothing; inspect for wounds
- Check neurovascular status before and after application (pulse, motor function, sensation)
- For severely angulated limb with neurovascular compromise: apply gentle longitudinal traction (≤10 lbs) before splinting; one attempt only
- Cover open wounds with dry sterile dressing first
- Immobilize the joint above and below a fracture (or the bone above and below a dislocation)
- After application: cool, elevate, reassess neurovascular status frequently
Splinting Materials
| Material | Characteristics |
|---|---|
| Plaster of Paris (calcium sulfate) | Most malleable, conforms well to limb, useful after reduction — sets slowly, heavier, damaged by moisture |
| Fiberglass (polyurethane resin) | Lightweight, fast-setting, moisture-resistant — less malleable |
Note: Both are exothermic on setting. Use room-temperature water to prevent burns — hot water accelerates setting and can cause thermal injury even at water temperatures that feel safe.
3.2 Common Splint Types
| Splint | Indication |
|---|---|
| Long-arm posterior splint | Elbow/proximal forearm fractures |
| Sugar-tong splint | Distal radius/wrist fractures; prevents pronation/supination |
| Short-arm ulnar gutter | 4th/5th metacarpal fractures ("boxer's fracture"), proximal phalanx ring/little finger |
| Short-arm radial gutter | Index/middle metacarpal/phalangeal injuries |
| Thumb spica | Scaphoid fracture, thumb metacarpal/proximal phalanx fractures |
| Posterior leg splint | Ankle, distal tibia fractures |
| Stirrup (ankle) splint | Ankle sprains, stable ankle fractures |
| Hard-soled shoe | Toe, 2nd–4th metatarsal, proximal 5th metatarsal fractures |
| Pneumatic walking brace | Stable foot/ankle fractures, moderate-severe ankle sprains |
| Sling + swath | Shoulder, proximal humerus — arm held across chest, secured with swath |
Splinting Complications
- Pressure necrosis
- Conversion of closed to open fracture (improper application)
- Neurovascular compromise (excessive tightness)
- Thermal burns (hot setting material)
- Compartment syndrome (especially with air splints)
— Tintinalli's Emergency Medicine; Roberts and Hedges' Clinical Procedures in Emergency Medicine
4. Traction
4.1 Historical Background
Traction for fractures dates from the time of Hippocrates. The modern traction splint was developed by Sir Hugh Owen Thomas (late 1800s) as a full-ring splint for femur fractures; later modified to a half-ring design by his nephew Sir Robert Jones for battlefield use. During World War I, use of the Thomas splint reduced femur fracture mortality from 80% to 15%.
4.2 Principles of Traction Splints
In femur fractures, muscle spasm causes the thigh to become spherical, increasing volume and allowing 1–2 L of hemorrhage to accumulate at the fracture site. A traction splint:
- Restores the cylindrical shape of the thigh
- Increases tissue pressure → reduces hemorrhage
- Reduces pain
- Prevents further damage to neurovascular structures
- Reduces incidence of fat embolism
4.3 Indications and Contraindications
| Indication | Isolated midshaft femur fracture |
| Contraindications | Pelvic fractures, hip injury with gross displacement, significant knee injury, avulsion/amputation of ankle or foot, associated distal tibia-fibula or ankle fracture in the same limb |
Open femur fracture: Use traction splint only when definitive care will be significantly delayed; irrigate before application; inform receiving clinician if contaminated fragments retract.
4.4 Types of Traction Splints
| Type | Key Feature |
|---|---|
| Thomas/Hare splint | Half-ring at proximal end (ischial tuberosity); most common prehospital splint |
| Sager splint | Applies bilateral traction with a single splint; does not extend beyond the heels; suited for confined spaces (helicopters, aircraft) |
Application principle: Apply traction gradually to approximately 10% of body weight or a maximum of 7 kg (15 lb) (15 kg/30 lb for bilateral fractures). The goal is stabilization and alignment — use the minimum force necessary.
4.5 After-Care / Monitoring
- Recheck distal neurovascular status after application and after every patient movement
- Secure patient and splint to stretcher
- Loss of pulses after splint application → immediately reassess strap position and traction amount
4.6 Traction Splint Complications
- Ongoing hemorrhage (if applied incorrectly)
- Peroneal nerve injury
- Perineal injury (pressure from proximal ring)
- Movement at fracture site
- Neurovascular compromise
- Wound contamination in open fractures
4.7 Skeletal Traction (Hospital Setting)
Used for definitive or temporary management (e.g., awaiting surgery), particularly for:
- Femoral shaft fractures (distal femoral or proximal tibial pin)
- Tibial plateau fractures
- Cervical spine injuries (skull tongs)
Traction weight is titrated by clinical examination and radiographic alignment. Skeletal traction carries risks of pin-site infection, osteomyelitis, neurovascular injury, and joint stiffness from prolonged immobility.
Key Sources:
- Rockwood and Green's Fractures in Adults, 10th ed. 2025
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.