Obstetrics and gynaecology history talking in MBBS final year
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
I now have excellent content from authoritative textbooks. Let me compile the comprehensive answer:
Obstetrics & Gynaecology History Taking - MBBS Final Year
Here is a structured, examination-ready guide to taking an OB/GYN history, based on Berek & Novak's Gynecology and Schwartz's Principles of Surgery (Gynecology section).
Structure of the OB/GYN History
1. Patient Identification
- Name, age, occupation, marital status, religion
- Address, date of admission/consultation
2. Chief Complaint (CC)
State the presenting complaint in the patient's own words with duration. Common OB/GYN complaints include:
- Vaginal bleeding (normal or abnormal)
- Vaginal discharge
- Lower abdominal / pelvic pain
- Amenorrhoea
- Mass per abdomen
- Infertility
- Urinary symptoms (incontinence, frequency)
- Postmenopausal bleeding
3. History of Present Illness (HPI)
Explore the complaint using the SOCRATES framework:
- Site - pelvic, lower abdomen, vulval, etc.
- Onset - sudden or gradual
- Character - nature of pain/bleeding/discharge
- Radiation - to back, thigh, shoulder tip (ectopic)
- Associated symptoms - nausea, fever, dyspareunia, urinary/bowel symptoms
- Timing - relation to menstrual cycle, coitus, pregnancy
- Exacerbating/relieving factors
- Severity - impact on daily life
4. Menstrual History (ALWAYS ask in every OB/GYN history)
| Parameter | What to Ask |
|---|---|
| Menarche | Age of first period |
| LMP | Date of last menstrual period |
| Cycle | Length of cycle (days); normal = 21-35 days |
| Duration | Number of days of bleeding; normal = 2-7 days |
| Amount | Number of pads/day, passage of clots |
| Regularity | Regular or irregular |
| Dysmenorrhoea | Primary or secondary (suggest endometriosis, adenomyosis) |
| IMB / PCB | Intermenstrual or post-coital bleeding |
| Menopause | Age; method (natural / surgical / drug-induced) |
| PMB | Post-menopausal bleeding (always a red flag - cancer until proved otherwise) |
Mnemonic for menstrual history: "MLDCAR" - Menarche, LMP, Duration, Cycle, Amount, Regularity
5. Obstetric History (Gravida, Para, Abortus)
Use the G P A or GTPAL notation:
- G = Gravida (total number of pregnancies including current)
- T = Term births (≥ 37 weeks)
- P = Preterm births (28-37 weeks)
- A = Abortions (spontaneous + induced, < 28 weeks)
- L = Living children
For each pregnancy, record:
- Year and outcome (term/preterm, live/stillbirth, abortion/MTP)
- Mode of delivery - SVD, instrumental (forceps/vacuum), LSCS (indication)
- Birth weight
- Complications - PPH, sepsis, preeclampsia, gestational diabetes
- Neonatal outcome - NICU admission, neonatal death
"Number of pregnancies, dates, type of deliveries, pregnancy loss, abortion, and complications should all be systematically recorded." - Schwartz's Surgery
6. Sexual History
Ask sensitively and non-judgementally:
- Age of first intercourse (coitarche)
- Number of partners (current and past)
- Type of sexual activity (vaginal, anal, oral)
- Dyspareunia (superficial or deep)
- Post-coital bleeding
- Partner's health / STI risk
- Pregnancy intention / desires fertility
7. Contraceptive History
- Current method of contraception and duration of use
- Past methods and reasons for discontinuation
- Any complications from contraceptive use (IUD: pelvic pain, menorrhagia; OCP: thrombosis)
- IUCD in situ?
8. Gynaecological Screening History
- Last Pap smear / cervical smear - date and result
- HPV DNA testing / vaccination status
- Prior abnormal smear and any treatment (LEEP, CKC, cryotherapy)
- Last mammogram / breast ultrasound
9. Past Medical History (PMH)
- Diabetes, hypertension, thyroid disorders (strongly linked to menstrual irregularity and infertility)
- Bleeding disorders (von Willebrand disease - consider in menorrhagia)
- Autoimmune conditions (SLE - recurrent pregnancy loss)
- Tuberculosis (Asherman syndrome, infertility)
- Previous malignancies
10. Past Surgical History (PSH)
- Abdominal or pelvic surgeries (risk of adhesions, tubal damage)
- Previous gynaecological procedures: D&C, hysteroscopy, laparoscopy, myomectomy, LSCS
- Anaesthetic complications
11. Drug History
- Current medications including OTC drugs
- Hormonal drugs (OCP, HRT, progesterone injections)
- Anticoagulants (warfarin, heparin, aspirin - affect bleeding)
- Herbal medications
- Drug allergies (drug name + type of reaction)
12. Family History
Focus on:
- Breast cancer (especially first-degree relatives, premenopausal or bilateral)
- Ovarian / endometrial / cervical cancer
- BRCA1/BRCA2 mutations, Lynch syndrome
- Gestational trophoblastic disease
- Diabetes, hypertension, thyroid disorders
- Bleeding disorders
13. Social History
- Smoking (cervical cancer risk, placental problems)
- Alcohol use
- Illicit drug use
- Occupation (stress, chemical exposure)
- Marital status and relationship dynamics
- Domestic violence / sexual abuse (ask sensitively, alone with patient)
- Diet and exercise
- Housing conditions
14. Systemic Review
Briefly enquire about symptoms in other systems that may be relevant:
- Breast - lumps, nipple discharge, skin changes
- Urinary - frequency, urgency, stress incontinence, haematuria
- Bowel - constipation, blood in stool, rectal pain (endometriosis)
- General - weight loss, fatigue, appetite
Key Points for Exams
- Always ask LMP - essential for all women of reproductive age (rules out pregnancy before any investigation or treatment).
- Gravity/Parity notation - examiners specifically test this; be clear with G/T/P/A/L.
- Post-menopausal bleeding = endometrial cancer until proved otherwise.
- Menstrual history is distinct from obstetric history - do not conflate the two.
- Sexual history must be taken sensitively and confidentially - examiner looks for communication skills.
- Past surgical history in gynaecology must include prior uterine surgeries (scar uterus risk in subsequent pregnancies).
- For a pregnant patient (obstetric history), additionally ask about: antenatal visits, booking investigations, fetal movements, symptoms of preeclampsia (headache, visual disturbance, epigastric pain, oedema).
Specific Obstetric History (for Antenatal Patient)
Additional points for a pregnant woman:
| Domain | Key Questions |
|---|---|
| Current pregnancy | EDD (by LMP and USS), gestational age, ANC bookings |
| Antenatal investigations | Blood group, Rh factor, VDRL, HIV, blood sugar, anomaly scan |
| Symptoms | Morning sickness, bleeding (antepartum haemorrhage), PV discharge, fetal movements |
| Risk factors | HTN, GDM, thyroid, multiple gestation, placenta praevia |
| Social | Domestic situation, support at home |
Sources: Berek & Novak's Gynecology (16th ed.), p. 54-55; Schwartz's Principles of Surgery (11th ed.), Table 41-1, p. 1815
Tell me history tracking with meaning of gynaecology words and like what is pain types, where is site in photo etc
Finding Sources
Finding Sources
Searching the Web
gynaecology medical terms meaning dysmenorrhoea dyspareunia amenorrhoea menorrhagia metrorrhagia MBBS
Finding Sources
Finding Sources
Finding Sources
Generating Image
Reading File
Generating Image
Now I have everything I need. Let me compile the full, richly illustrated answer:
OB/GYN History Taking - Medical Terms Explained Visually
PART 1 - PAIN SITE DIAGRAM (Abdomen Regions)
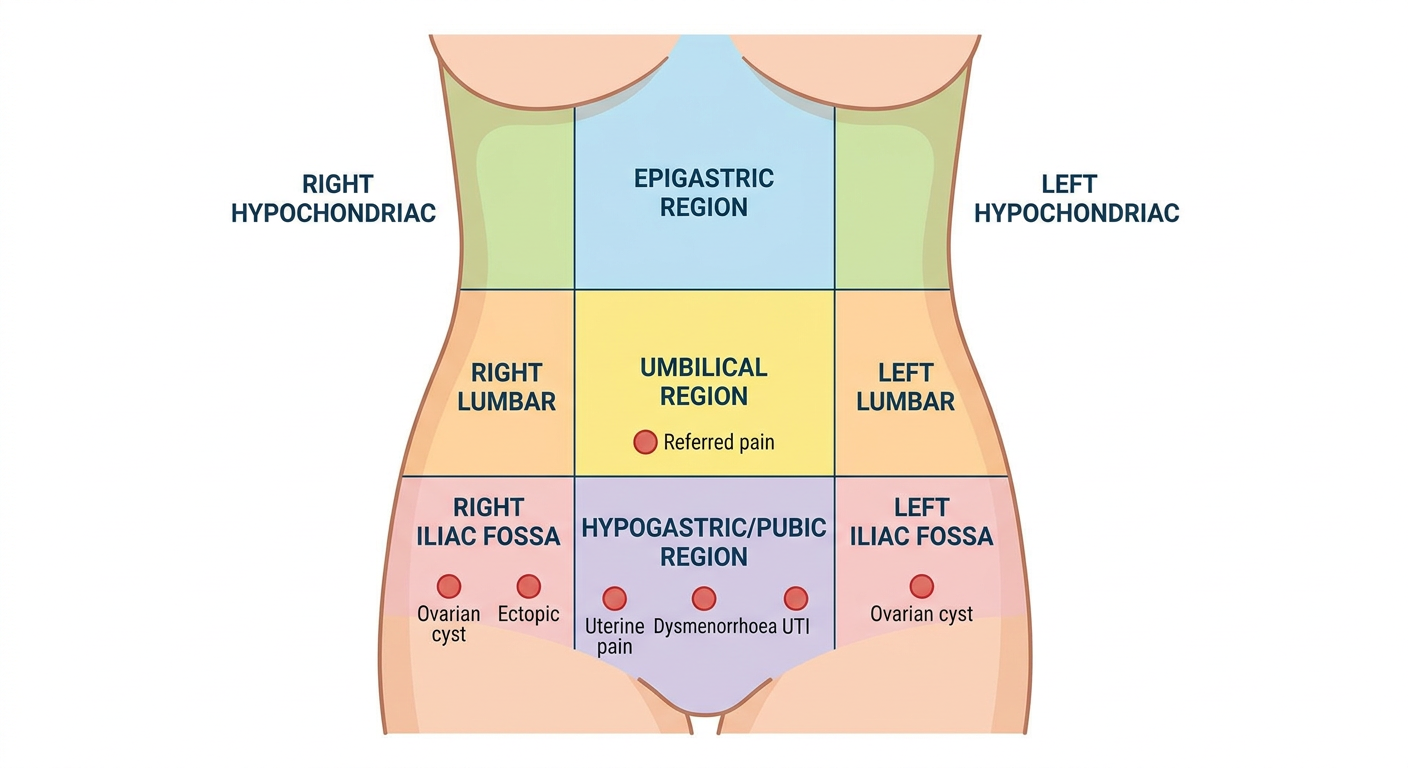
What Each Region Means in Gynaecology
| Region | Location | Gynaecological Causes |
|---|---|---|
| Right Iliac Fossa (RIF) | Lower right | Ovarian cyst (right), ectopic pregnancy (right tube), appendix (surgical overlap) |
| Left Iliac Fossa (LIF) | Lower left | Ovarian cyst (left), ectopic (left tube), endometriosis |
| Hypogastrium / Pubic | Lower centre (above pubis) | Uterine pain, dysmenorrhoea, fibroids, UTI, PID, bladder |
| Umbilical | Centre | Referred pain from pelvic organs (early appendix, ovarian cyst torsion) |
| Lumbar (flanks) | Either side of umbilicus | Ureteric colic, renal causes |
| Epigastrium | Upper centre | Referred shoulder-tip pain (ectopic rupture - diaphragm irritation by blood) |
Key exam point: Ectopic pregnancy rupture causes shoulder-tip pain (referred) because blood in the peritoneum irritates the diaphragm (phrenic nerve = C3,4,5 = shoulder region).
PART 2 - TYPES OF PAIN (with diagrams)
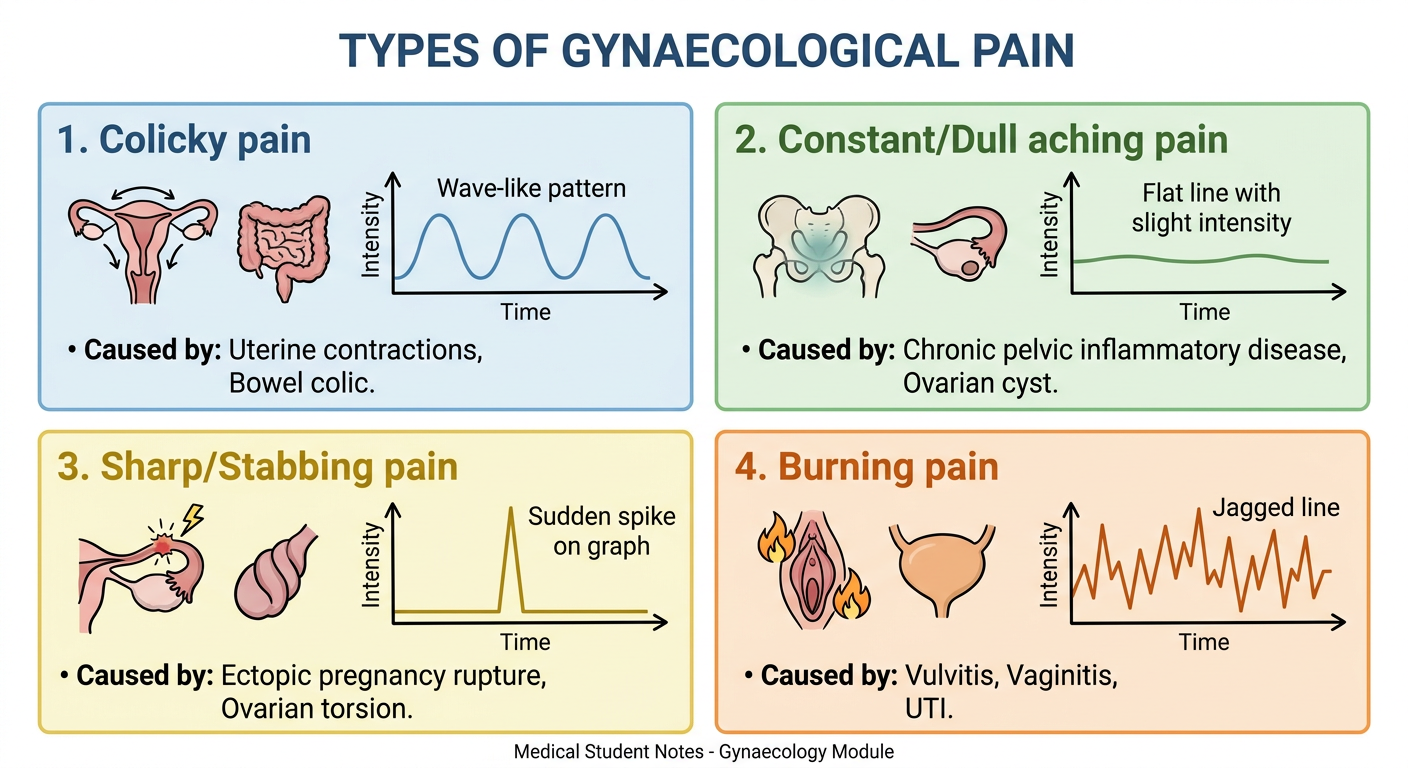
Pain Types Explained Simply
| Pain Type | What it feels like | Gynaecological Causes |
|---|---|---|
| Colicky | Comes and goes in waves, like cramps | Dysmenorrhoea (uterine contractions), miscarriage, labour |
| Constant / Dull ache | Always there, heavy dragging feeling | Chronic PID, fibroid, ovarian cyst, endometriosis |
| Sharp / Stabbing | Sudden, severe, knife-like | Ectopic rupture, ovarian torsion, follicle rupture (Mittelschmerz) |
| Burning | Hot, irritating | Vulvitis, vaginitis, UTI, herpes |
| Deep Dyspareunia | Pain deep inside during sex | Endometriosis, PID, ovarian cyst, retroverted uterus |
| Superficial Dyspareunia | Pain at the vaginal entrance during sex | Vaginismus, vulvodynia, atrophic vaginitis |
PART 3 - GYNAECOLOGY MEDICAL TERMS (Word by Word)
Bleeding Terms
| Medical Word | Meaning | Simple Explanation |
|---|---|---|
| Menorrhagia | Meno = menses + rrhagia = excessive flow | Heavy periods (> 80 mL per cycle OR > 7 days) |
| Metrorrhagia | Metro = uterus + rrhagia = flow | Bleeding between periods (irregular, not related to cycle) |
| Menometrorrhagia | Combined | Heavy AND irregular bleeding |
| Polymenorrhoea | Poly = many + meno = menses | Periods coming too frequently (< 21 days apart) |
| Oligomenorrhoea | Oligo = few | Infrequent periods (> 35 days apart) |
| Amenorrhoea | A = absence + meno = menses | No periods at all |
| Hypomenorrhoea | Hypo = less | Scanty/very light periods |
| Spotting | - | Light bleeding, just staining underwear |
| IMB | Intermenstrual bleeding | Bleeding between periods |
| PCB | Post-coital bleeding | Bleeding after sex (red flag - think cervical cancer) |
| PMB | Post-menopausal bleeding | Bleeding 12+ months after last period (RED FLAG - endometrial cancer) |
Amenorrhoea Types
| Type | Meaning |
|---|---|
| Primary amenorrhoea | Never had a period by age 16 (with secondary sex characteristics) or 14 (without) |
| Secondary amenorrhoea | Previously had periods, now absent for > 3 months (if irregular) or > 6 months (if regular) |
| Physiological | Pregnancy, breastfeeding, menopause - NORMAL |
| Pathological | Caused by disease (PCOS, hyperprolactinaemia, thyroid, Asherman's) |
Pain Terms
| Medical Word | Meaning | Simple Explanation |
|---|---|---|
| Dysmenorrhoea | Dys = painful + meno = menses | Painful periods |
| Primary dysmenorrhoea | No underlying pathology | Prostaglandin-driven cramping, starts within 1-2 years of menarche |
| Secondary dysmenorrhoea | Caused by underlying disease | Endometriosis, adenomyosis, fibroids, PID - starts LATER in life |
| Dyspareunia | Dys = painful + pareunia = intercourse | Painful sex |
| Superficial dyspareunia | Pain at the vaginal opening | Vaginismus, infections, vulvodynia |
| Deep dyspareunia | Pain deep in pelvis during sex | Endometriosis, PID, ovarian cysts |
| Vaginismus | - | Involuntary tightening of vaginal muscles - prevents penetration |
| Mittelschmerz | German: "middle pain" | Ovulation pain - mid-cycle, unilateral, RIF or LIF |
| Chronic pelvic pain | - | Pain below umbilicus lasting > 6 months |
Discharge Terms
| Medical Word | Meaning | Simple Explanation |
|---|---|---|
| Leucorrhoea | Leuco = white + rrhoea = flow | Normal white/clear physiological vaginal discharge |
| Vaginitis | - | Inflammation of the vagina - often infected discharge |
| Cervicitis | - | Inflammation of the cervix |
| Pruritus vulvae | - | Itching of the vulva |
| Bartholinitis | - | Infection of Bartholin's gland (swelling at vaginal entrance) |
Obstetric Terms
| Medical Word | Meaning | Simple Explanation |
|---|---|---|
| Gravida (G) | Gravidus = pregnant | Total number of pregnancies (including current) |
| Para (P) | Parere = to deliver | Number of deliveries after 28 weeks (live or stillbirth) |
| Nulligravida | Nulli = none | Never been pregnant |
| Nullipara | - | Never delivered |
| Primigravida | Primi = first | First pregnancy |
| Multigravida | Multi = many | More than one pregnancy |
| Grand multipara | Grand = large | 5 or more deliveries |
| LMP | Last Menstrual Period | First day of the last period - used to calculate EDD |
| EDD | Expected Date of Delivery | LMP + 9 months + 7 days (Naegele's rule) |
| EGA / POG | Estimated Gestational Age / Period of Gestation | How many weeks pregnant |
| Quickening | - | First felt fetal movements (16-20 weeks) |
| Antepartum | - | Before delivery |
| Postpartum | - | After delivery |
| Stillbirth | - | Baby born dead after 28 weeks |
| Abortion | - | Loss of pregnancy before 28 weeks |
| MTP | Medical Termination of Pregnancy | Induced abortion |
GTPAL Notation (Exam Favourite)
G2 T1 P0 A1 L1 means:
- 2 total pregnancies
- 1 term delivery (≥37 weeks)
- 0 preterm deliveries (28-37 weeks)
- 1 abortion (miscarriage or MTP)
- 1 living child
Other Important Gynaecology Terms
| Term | Meaning |
|---|---|
| Menarche | Age of first menstruation |
| Menopause | Last menstrual period (confirmed after 12 months of amenorrhoea) |
| Perimenopause | Transition period around menopause |
| Endometriosis | Endometrium-like tissue outside the uterus |
| Adenomyosis | Endometrial glands within the myometrium (muscle of uterus) |
| Fibroids / Leiomyoma | Benign smooth muscle tumour of the uterus |
| PCOS | Polycystic Ovarian Syndrome - irregular periods + excess androgens |
| PID | Pelvic Inflammatory Disease - infection of upper genital tract |
| Ovarian torsion | Ovary twists on its pedicle - surgical emergency |
| Ectopic pregnancy | Pregnancy outside the uterus (usually fallopian tube) |
| Hydatidiform mole | GTD - abnormal placental tissue, no viable fetus |
PART 4 - PALM-COEIN Classification (AUB)
Modern classification of Abnormal Uterine Bleeding (replaces old term "dysfunctional uterine bleeding"):
PALM = Structural causes COEIN = Non-structural causes
P - Polyp C - Coagulopathy
A - Adenomyosis O - Ovulatory dysfunction
L - Leiomyoma (fibroid) E - Endometrial
M - Malignancy I - Iatrogenic
N - Not yet classified
Normal blood loss per cycle = 35 mL | Abnormal = > 80 mL Normal duration = 2-7 days | Normal cycle = 21-35 days
(Source: Rosen's Emergency Medicine & Berek & Novak's Gynecology)
PART 5 - QUICK HISTORY-TAKING CHECKLIST (Exam Flowchart)
START → Patient ID → Chief Complaint
↓
HPI (SOCRATES for pain/bleeding)
↓
┌────────────────────────────────┐
│ MENSTRUAL HISTORY │
│ Menarche → LMP → Cycle → │
│ Duration → Amount → Regularity │
│ Dysmenorrhoea → IMB/PCB/PMB │
└────────────────────────────────┘
↓
┌────────────────────────────────┐
│ OBSTETRIC HISTORY │
│ G P T A L → Each pregnancy: │
│ Date, mode, complications, │
│ birth weight, baby outcome │
└────────────────────────────────┘
↓
Sexual Hx → Contraceptive Hx → Screening Hx
↓
PMH → PSH → Drug Hx → Family Hx → Social Hx
↓
Systemic Review (Breast / Urinary / Bowel)
Sources: Berek & Novak's Gynecology (16th ed.); Schwartz's Principles of Surgery (11th ed.), Table 41-1; Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.