Chest xray
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Here is a thorough guide to normal chest X-ray anatomy and interpretation, drawn from Grainger & Allison's Diagnostic Radiology.
Normal Chest X-Ray (CXR) - Anatomy & Interpretation
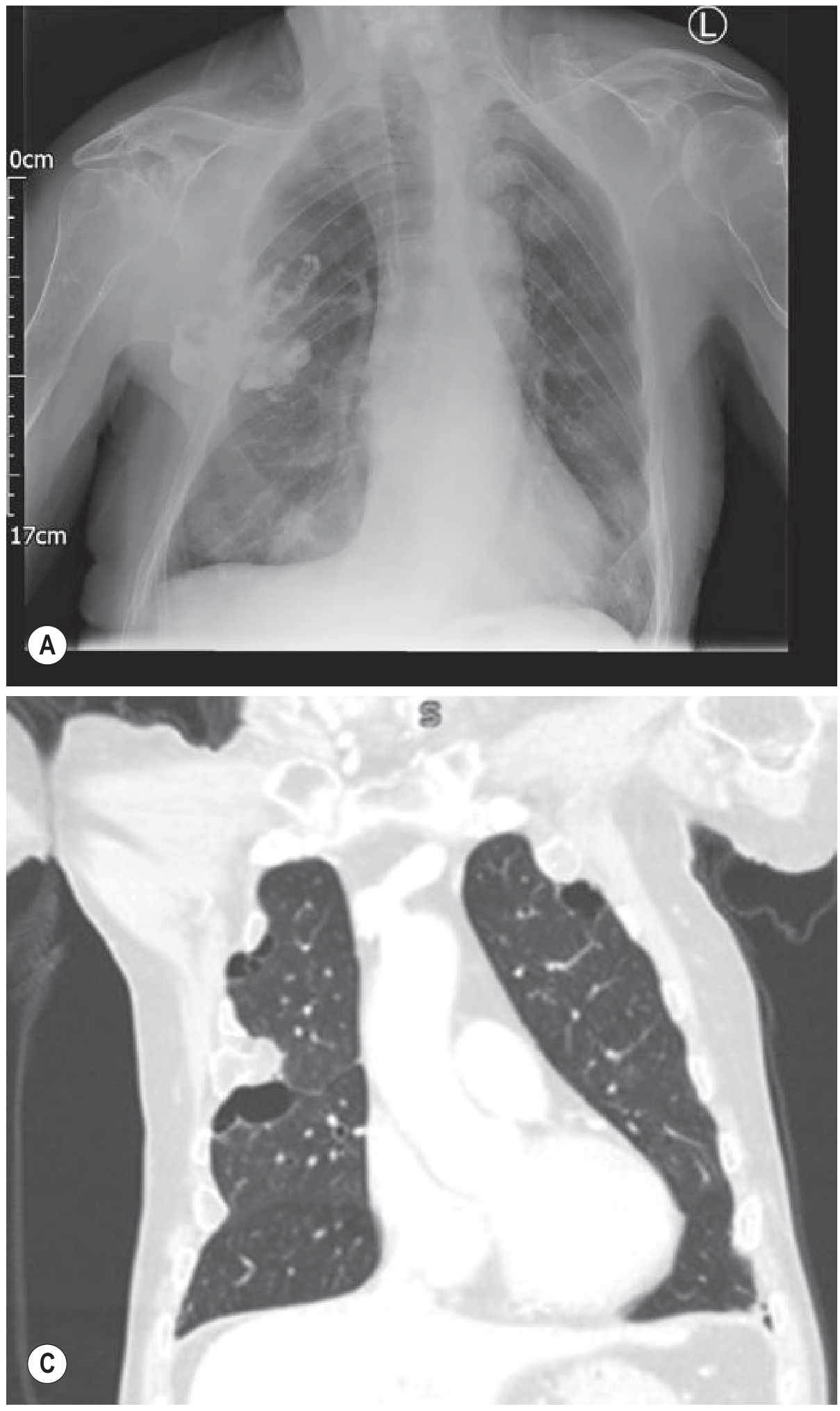
PA chest radiograph (top) with coronal CT lung windows (bottom) - Grainger & Allison's Diagnostic Radiology
Standard Views
| View | Notes |
|---|---|
| PA (posteroanterior) | Standard erect view; patient faces detector, X-ray beam from behind. Minimises cardiac magnification. |
| AP (anteroposterior) | Done supine/portable (ICU, trauma). Cardiac silhouette is magnified - do not measure CTR on AP films. |
| Lateral | Identifies posterior costophrenic recesses and lesions hidden behind the heart/diaphragm on PA. |
Key Structures - What to See
1. Trachea
- Midline at the neck, deviates slightly to the right at the level of the aortic arch - a normal variant.
- The carina (bifurcation) lies at the level of T4/T5 (roughly the angle of Louis).
- The carinal angle is normally < 70°; widening suggests left atrial enlargement.
2. Heart
- The cardiothoracic ratio (CTR) should be < 0.5 on a PA film (heart width : widest chest width).
- Right heart border = right atrium.
- Left heart border (top to bottom) = aortic knuckle → pulmonary trunk → left atrial appendage → left ventricle.
- The right hemidiaphragm is normally higher than the left by ~15 mm (up to 30 mm is normal) because of the liver.
3. Mediastinum
- Superior mediastinum: contains aorta, SVC, trachea, oesophagus, lymph nodes.
- Aortic knuckle: visible on the left at the level of T4 - the aortic arch.
- Mediastinal widening (> 8 cm at T4) raises concern for aortic pathology, lymphoma, or mass.
4. Hila
- Left hilum is normally higher than the right by up to 3 cm.
- Hila are composed mainly of pulmonary arteries (upper lobe veins also contribute).
- Hilar enlargement may be unilateral (lymphoma, sarcoid, lung cancer) or bilateral (sarcoidosis, bilateral hilar lymphadenopathy).
5. Lungs
- Lung markings (vascular shadows) should be visible to the lung periphery.
- Upper zone vessels are normally smaller than lower zone vessels on an erect film.
- Upper lobe blood diversion (upper > lower lobe vessel size) = sign of raised pulmonary venous pressure.
- The fissures: horizontal fissure (right side, runs from hilum to 6th rib laterally); oblique fissures (not seen on PA, visible on lateral).
6. Diaphragm
- Each hemidiaphragm is a smooth, convex upward curve.
- The diaphragm normally lies at the level of the 5th or 6th anterior rib interspace in the mid-lung field.
- The costophrenic (CP) angles should be sharp and acute - blunting requires ~200-500 mL of pleural fluid.
- The cardiophrenic angles are often less well-defined due to adjacent fat.
7. Soft Tissues & Bones
- Check ribs (fractures, notching), clavicles, scapulae, spine.
- Rib notching (inferior) = coarctation of the aorta.
- Soft tissue: breast shadows, subcutaneous emphysema, neck/axillary masses.
A Systematic Approach (ABCDE)
| Letter | What to Assess |
|---|---|
| A - Airway | Trachea midline? Carina angle? ETT/tracheostomy position? |
| B - Breathing (Lungs) | Lung fields clear? Pneumothorax? Consolidation? Effusion? Fissures visible? |
| C - Cardiac | CTR < 0.5? Cardiac borders sharp? Calcification? |
| D - Diaphragm | CP angles sharp? Right > left? Free gas below? |
| E - Everything else | Mediastinum width? Hila? Bones? Soft tissue? Tubes/lines/devices? |
Common Normal Variants (Not Pathology)
- Slight right tracheal deviation at the aortic arch
- Prominent aortic knuckle in the elderly (unfolded aorta)
- Visible azygos fissure (accessory fissure, right upper lobe)
- Slight leftward rotation making the left heart border appear more prominent
- Fat pads at cardiophrenic angles - can simulate cardiomegaly
Judging Film Quality (RIPE)
| Letter | Criterion |
|---|---|
| R - Rotation | Medial ends of both clavicles equidistant from the spinous process |
| I - Inspiration | ≥ 6 anterior ribs (or 10 posterior ribs) visible above the diaphragm |
| P - Projection | PA vs AP (check if labelled) |
| E - Exposure | Vertebral bodies barely visible through the cardiac shadow; lung vasculature visible |
Sources: Grainger & Allison's Diagnostic Radiology (9780323760751); Roberts & Hedges' Clinical Procedures in Emergency Medicine (9780323354783)
This is a shared conversation. Sign in to Orris to start your own chat.