Optic neuritis
Reading File
Finding Sources
Searching Images
optic neuritis fundus clinical features
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Here is a comprehensive overview of optic neuritis, drawn from multiple authoritative sources.
Optic Neuritis
Definition & Pathophysiology
Optic neuritis is an inflammatory optic neuropathy most commonly caused by demyelinating disease. Demyelination disrupts nerve conduction within the white matter; myelin is phagocytosed by microglia and macrophages, with astrocytes subsequently laying down fibrous tissue in plaques. — Kanski's Clinical Ophthalmology, 10th ed.
Clinical Features
| Feature | Detail |
|---|---|
| Visual loss | Typically monocular; onset over hours to a few days; can range from mild reduction to no light perception |
| Pain | Periocular pain worsening with eye movement in ~90% of cases; typically lasts 3–5 days |
| Color vision | Impaired out of proportion to acuity; red desaturation (red object appears pink in affected eye) |
| Visual field | Diffuse depression or discrete scotomas (non-specific) |
| Afferent pupillary defect (APD) | Commonly present |
| Fundus | Normal in ~70% (retrobulbar neuritis); disc edema (papillitis) in ~30% — mild, less prominent than papilledema |
Pain persisting >7 days should prompt reconsideration of the diagnosis. — Bradley and Daroff's Neurology in Clinical Practice
Fundus Findings
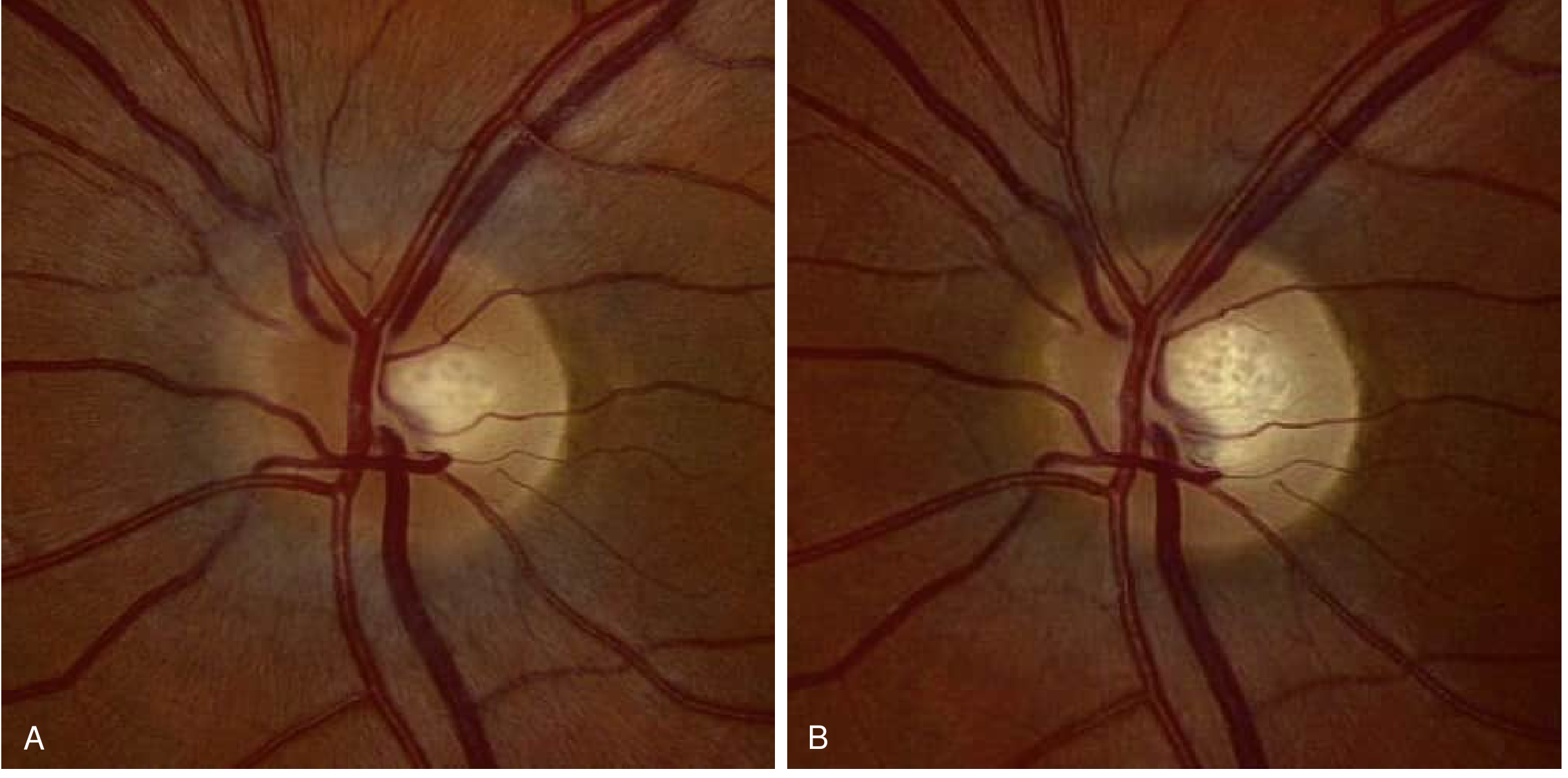
Fig. A — Acute optic neuritis: mild nasal disc edema, no hemorrhages or cotton-wool spots. B — Same eye 3 months later: edema resolved, mild temporal pallor indicating axonal loss. — Bradley and Daroff's Neurology in Clinical Practice
Etiology
- Idiopathic / Multiple sclerosis — most common
- NMOSD (Devic disease) — antibodies against aquaporin-4; bilateral optic neuritis + long-segment transverse myelitis
- MOGAD — antibodies against myelin oligodendrocyte glycoprotein; bilateral simultaneous optic neuropathy is a common feature
- Infections — measles, mumps, varicella, herpes zoster, EBV, syphilis, TB, cryptococcosis
- Post-vaccination (especially childhood vaccines)
- Contiguous inflammation — meningitis, orbital cellulitis, sinusitis
- Sarcoidosis
— Tintinalli's Emergency Medicine
Investigations
| Test | Finding |
|---|---|
| MRI brain (gadolinium) | White matter plaques; optic nerve enhancement on STIR/fat-sat T1 sequences; key prognosticator for MS risk |
| MRI orbits | Optic nerve swelling and T2 hyperintensity |
| VEP | Prolonged latency and reduced amplitude — abnormal in up to 100% of MS-associated cases |
| OCT | Retinal nerve fiber layer (RNFL) and ganglion cell layer atrophy post-episode |
| CSF | Oligoclonal bands in 90–95% of MS-associated cases |
| NMO-IgG (anti-AQP4) | Positive in ~70% of NMOSD — highly specific |
Risk of Progression to MS
- Overall 15-year risk: ~50% after a first optic neuritis episode
- With ≥1 MRI brain lesion: risk >70%
- With normal MRI: risk ~25%
Factors associated with lower MS risk (especially if MRI is normal):
- Male sex
- Optic disc swelling, disc/peripapillary hemorrhages, or macular exudates
- Vision reduced to no light perception
- Absent periocular pain
- No preceding viral syndrome
- Negative EBV serology
Optic neuritis is the presenting feature of MS in up to 30% of MS patients, and occurs at some point in 50% of established MS cases. — Kanski's Clinical Ophthalmology
Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Anterior ischemic optic neuropathy (AION) | Sudden, painless; older patients; pallid disc edema (GCA) or hyperemic (non-arteritic) |
| Papilledema | Bilateral; painless; visual acuity preserved until late |
| Hypertensive retinopathy | Systemic hypertension; bilateral |
| Orbital/intracranial tumor | Proptosis; visible on CT/MRI |
| Toxic/metabolic optic neuropathy | Alcohol, heavy metals, chloroquine — bilateral, painless |
| LHON | Peripapillary telangiectatic microangiopathy; mitochondrial genetics |
Treatment
Acute:
- IV methylprednisolone (high-dose) — hastens visual recovery; reduces short-term MS risk over the following 2 years, but does not significantly affect long-term visual outcomes
- Oral prednisone alone (1 mg/kg) should be avoided — associated with increased risk of recurrence
- For NMOSD: high-dose IV steroids → oral taper; plasmapheresis if steroid-refractory
Disease-modifying therapy (MS prevention):
- Early immunomodulatory treatment in high-risk patients (MRI lesions) to reduce 2–5 year MS risk
- NMOSD-specific agents: eculizumab, inebilizumab, satralizumab (for anti-AQP4+ patients); rituximab
Prognosis
- Visual recovery generally begins within 1 month; prognosis correlates with severity of initial deficit
- In MS-associated optic neuritis, vision usually improves without treatment over several months
- Post-episode OCT typically shows RNFL atrophy — a reliable structural marker of axonal loss even after clinical recovery
Sources: Bradley and Daroff's Neurology in Clinical Practice | Kanski's Clinical Ophthalmology, 10th ed. | Tintinalli's Emergency Medicine | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.