Vitamin b12 deficiency, neuropathy and treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
"vitamin B12 deficiency" AND neuropathy
Reading File
Reading File
Reading File
Searching PubMed
"cobalamin deficiency" AND "peripheral neuropathy" AND treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, authoritative information from multiple major textbooks. Let me compile the full answer.
Vitamin B12 (Cobalamin) Deficiency, Neuropathy, and Treatment
Overview
Vitamin B12 (cobalamin) deficiency affects both the hematopoietic and nervous systems. Notably, neurological and hematological manifestations do not always coincide - up to 40% of patients with neurological B12 deficiency have no anemia or macrocytosis, making clinical suspicion and biochemical testing essential.
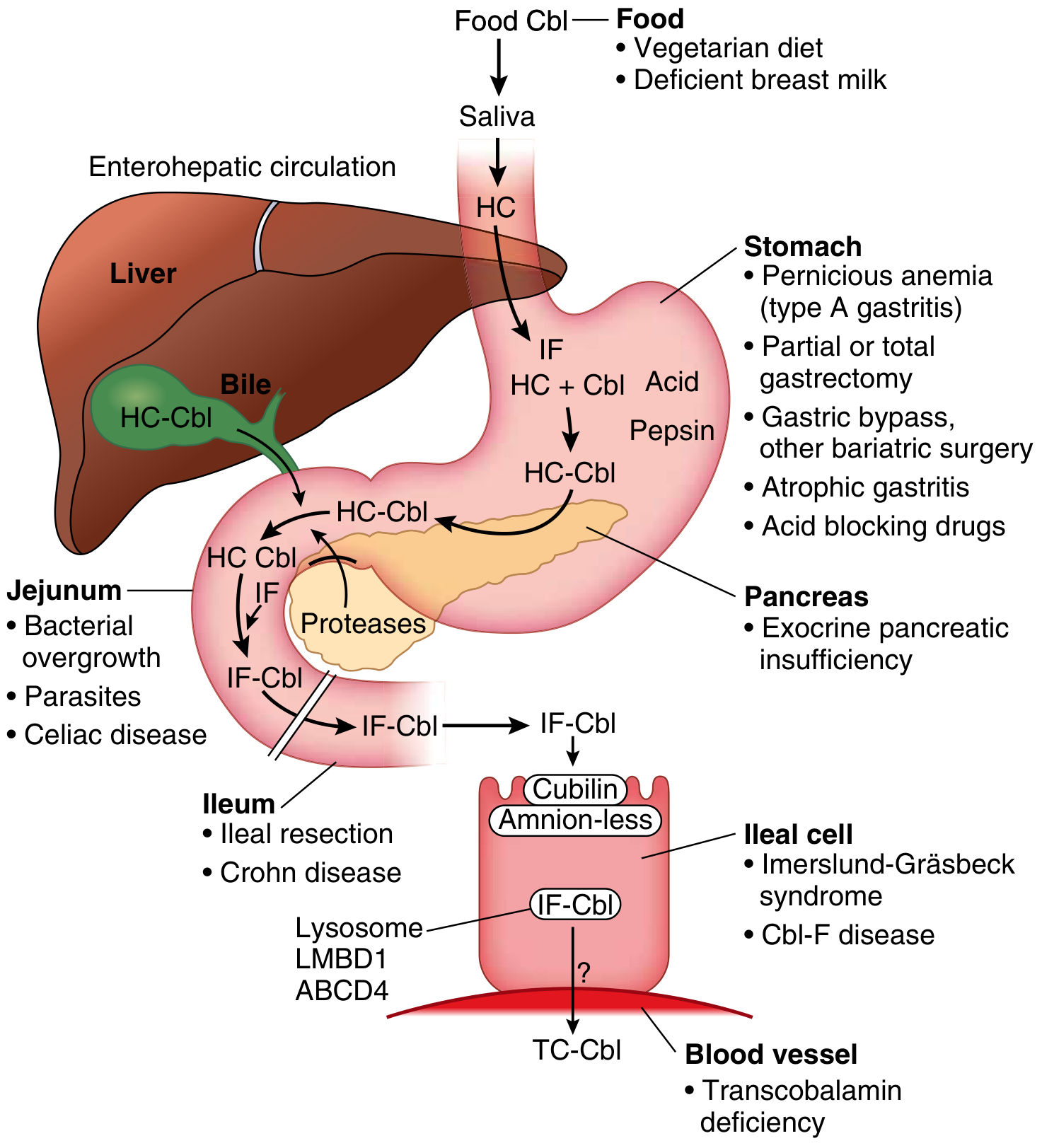
Cobalamin absorption pathway showing sites where deficiency can arise - Goldman-Cecil Medicine
Biochemical Basis
Cobalamin is a cofactor in only two enzymatic reactions in humans:
- Methionine synthase: methylcobalamin converts homocysteine to methionine, using methyl-THF. Methionine is activated to S-adenosylmethionine (SAM), the methyl donor for lipid synthesis, neurotransmitter production, DNA methylation, and myelin maintenance.
- Methylmalonyl-CoA mutase: adenosylcobalamin converts methylmalonyl-CoA to succinyl-CoA. Blockage causes methylmalonic acid (MMA) accumulation.
When cobalamin is deficient, methionine synthesis fails, SAM drops, and myelin maintenance is impaired. This is the primary mechanism of neurological damage. - Goldman-Cecil Medicine, p. 1728
Causes of Deficiency
| Category | Examples |
|---|---|
| Lack of intrinsic factor | Pernicious anemia (autoimmune type A gastritis), gastrectomy, gastric bypass, congenital IF defect |
| Food-cobalamin malabsorption | Atrophic gastritis, achlorhydria, exocrine pancreatic dysfunction |
| Ileal disease | Crohn disease, ileal resection, Imerslund-Gräsbeck syndrome |
| Intestinal usurpation | Bacterial overgrowth, blind loops, Diphyllobothrium latum, Giardia |
| Dietary/nutritional | Strict vegans, breast-fed infants of deficient mothers |
| Drug-induced | Nitrous oxide (recreational "whippets" or anesthesia), metformin, PPIs, H2 blockers |
| Inborn errors | Transcobalamin II deficiency, CblC-J mutations |
Pernicious anemia is the most common cause overall. Food-cobalamin malabsorption is an underappreciated cause, particularly in older individuals. - Harrison's Principles, p. 3655; Goldman-Cecil, p. 1064
Neurological Manifestations
Subacute Combined Degeneration (SCD)
The spinal cord is affected first and most prominently. The term "subacute combined degeneration" refers specifically to the B12-deficiency lesion of the spinal cord involving both the posterior columns (dorsal) and lateral columns (corticospinal tracts). This is the hallmark neurological presentation.
Symptom progression:
-
Early: symmetric paresthesias (tingling, "pins and needles") beginning in the hands, then feet - constant and progressive
-
Progressive: unsteady gait, stiffness and weakness of legs, sensory ataxia
-
Advanced: ataxic paraplegia with variable spasticity, loss of proprioception and vibration sense
-
Severe: behavioral changes ranging from mild irritability/forgetfulness to frank psychosis, dementia, optic neuropathy
-
Adams and Victor's Principles of Neurology 12e, p. 1176
Peripheral Neuropathy
The peripheral neuropathy of B12 deficiency is a point of some debate. The clinical features include:
- Large-fiber sensory loss predominates - proprioception and vibration affected more than pain/temperature
- Absent Achilles reflexes combined with diffuse hyperreflexia (hyperreflexia from corticospinal tract damage + areflexia from posterior root/peripheral damage)
- Electrodiagnostics: axonal sensorimotor neuropathy pattern on nerve conduction studies
- Early in SCD, nerve conduction may be normal; when abnormal, somatosensory evoked potentials show central conduction delays, implicating the posterior columns as primary
- Some patients present with pure peripheral neuropathy without obvious myelopathy
"Numb hands typically appear before lower extremity paresthesias." - Harrison's, p. 3655
Other Neurological Manifestations
- Optic neuropathy (optic atrophy in severe cases)
- Encephalopathy (cognitive slowing, dementia, psychosis)
- Neuropsychiatric symptoms can appear even without hematological abnormalities
Key Clinical Pearl
Since folic acid fortification began (US, 1994), anemia is no longer a reliable marker of B12 deficiency. The myeloneuropathy severity is inversely related to the severity of megaloblastic anemia - severe neurological disease can present with minimal or absent anemia. - Bradley & Daroff Neurology in Clinical Practice
Hematological Manifestations
- Megaloblastic anemia: oval macrocytes, hypersegmented neutrophils (>1 cell with 6 lobes or >5 cells with 5 lobes per 100 is abnormal), pancytopenia in severe cases
- Ineffective erythropoiesis: intramedullary hemolysis causing indirect hyperbilirubinemia, elevated LDH, low haptoglobin
- The bone marrow shows hypercellularity with nuclear-cytoplasmic dissociation - can be mistaken for acute leukemia
Diagnosis
Serum B12: Normal range 150-660 pM (~200-900 pg/mL). Deficiency suspected below 150 pM. May be falsely normal in liver disease or myeloproliferative disorders. - Goodman & Gilman's, p. 933
Confirmatory metabolite testing (more sensitive and specific):
- Methylmalonic acid (MMA): elevated in cobalamin deficiency - most sensitive marker
- Homocysteine: elevated in both cobalamin AND folate deficiency (less specific)
- These are elevated even with normal serum B12 levels, detecting intracellular deficiency
Pernicious anemia workup:
- Anti-intrinsic factor antibodies (~60% sensitivity, highly specific)
- Anti-parietal cell antibodies (~90% in PA)
- Endoscopy with gastric biopsy recommended (PA patients are at higher risk for gastric carcinoid and adenocarcinoma)
Neuroimaging: MRI can show T2 signal changes in the posterior and lateral columns of the cervical and upper thoracic cord.
Electrodiagnostics: NCS typically shows axonal sensorimotor pattern; somatosensory evoked potentials may show central conduction delay.
Treatment
Parenteral (First-line for severe/neurological disease)
In severely symptomatic patients or confirmed pernicious anemia:
| Phase | Regimen |
|---|---|
| Loading (severe) | 1000 µg cyanocobalamin or hydroxocobalamin IM/SC daily for 7 days, or every other day for 2 weeks |
| Consolidation | Weekly injections for 4-8 weeks |
| Maintenance | Monthly IM injections indefinitely |
- Hydroxocobalamin is retained better than cyanocobalamin; after loading, can be given every 2-4 months instead of monthly
- A single 10,000 µg dose can correct pernicious anemia for at least 3 months
- There is no toxicity upper limit for cobalamin
- Goldman-Cecil Medicine, p. 1389; Adams & Victor, p. 1179
High-Dose Oral (Equally effective for most causes)
Randomized trials show oral cobalamin 1000-2000 µg/day is equivalent to parenteral for rising serum B12 and normalizing MMA and homocysteine. About 0.5-2% of a high dose is absorbed by passive diffusion independent of intrinsic factor.
- Patients with food-cobalamin malabsorption (but intact IF mechanism) can absorb free oral cobalamin and should be treated this way
- Severe symptomatic disease: start at ≥2000 µg/day orally (absorbs ~20-40 µg/day)
- Maintenance after parenteral loading: 500-2000 µg/day orally is acceptable
- Tablets are available over the counter in the US (500 µg to 2.5 mg formulations)
- Goldman-Cecil Medicine, p. 1389-1390
Note on pernicious anemia: Parenteral or nasal/sublingual routes are generally preferred over oral for confirmed PA with neurological manifestations, as oral absorption still relies on some mucosal function.
Other Formulations
- Intranasal and sublingual preparations exist but are less studied for true pernicious anemia
- Methylcobalamin and adenosylcobalamin forms offer no proven advantage over cyano- or hydroxocobalamin for most indications; however, methylcobalamin may be specifically useful for neuropathic pain treatment
Prognosis of Neuropathy
Recovery depends critically on how long symptoms have been present before treatment:
- < 3 months duration: greatest improvement, often complete recovery
- 3-12 months: improvement mostly in first 3-6 months, slower over the following year
- Long-standing disease: best outcome is arrest of progression; significant residual deficit is likely
- Neurological improvement and arrest of progression occur at any stage; treatment should never be withheld
"The extent of residua correlates with the severity and duration of symptoms before treatment." - Bradley & Daroff Neurology in Clinical Practice
Special Situations
| Situation | Note |
|---|---|
| Nitrous oxide exposure | Inactivates methionine synthase; can precipitate acute SCD even in marginally deficient patients; treat urgently with IM B12 |
| Metformin use | Reduces B12 absorption; monitor B12 annually in diabetic patients on long-term metformin |
| Vegans/vegetarians | Oral supplementation prophylactically (25-100 µg/day) or high-dose (1000 µg/day) |
| Pregnancy | Deficiency in mother causes deficiency in breast-fed infant; supplement throughout |
| Folic acid fortification | Can mask megaloblastic anemia but does NOT prevent neurological damage; neurological B12 deficiency can progress silently |
Sources:
- Goldman-Cecil Medicine International Edition, Chapter 150 (Cobalamin Deficiency)
- Adams and Victor's Principles of Neurology, 12th Edition, p. 1176-1179
- Harrison's Principles of Internal Medicine, 22e (2025), p. 3655
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 933
- Bradley & Daroff's Neurology in Clinical Practice
Role of pregabalin and mecofol combination
Reading File
Finding Sources
Finding Sources
Searching PubMed
pregabalin AND methylcobalamin AND neuropathy
Reading File
Reading File
Reading Article
Searching PubMed
pregabalin AND mecobalamin AND diabetic neuropathy
Reading File
Reading File
Searching PubMed
pregabalin AND methylcobalamin AND combination AND "diabetic peripheral neuropathy"
I have everything I need. Let me now compose the comprehensive answer.
Pregabalin + Mecobalamin (Mecofol) Combination: Role in Neuropathy
What Is Mecofol?
Mecofol is a brand name for mecobalamin, which is the same as methylcobalamin - the active, neurologically bioavailable form of vitamin B12. Unlike cyanocobalamin (the synthetic storage form), methylcobalamin crosses the blood-brain barrier more readily, participates directly in methionine synthase activity, and is specifically taken up by nerve tissue, where it supports myelin synthesis and axonal regeneration.
The pregabalin + mecobalamin combination is widely used in South Asia, Southeast Asia, and other markets for neuropathic pain conditions, particularly diabetic peripheral neuropathy (DPN), postherpetic neuralgia, and other painful neuropathies.
Rationale for the Combination: Complementary Mechanisms
The two drugs target fundamentally different aspects of neuropathic disease, making their combination logical:
| Property | Pregabalin | Mecobalamin (Methylcobalamin) |
|---|---|---|
| Drug class | α2-δ ligand / GABA analog | Active B12 coenzyme |
| Primary action | Symptom control (pain suppression) | Disease modification (nerve repair) |
| Mechanism | Blocks voltage-gated calcium channels (α2-δ subunit) at presynaptic terminals → reduces release of glutamate, substance P, noradrenaline → dampens central sensitization | Cofactor for methionine synthase → restores SAM → supports phospholipid and myelin synthesis; promotes axonal regeneration and Schwann cell function |
| Acts on | Central sensitization, pain signaling | Peripheral nerve structure and metabolism |
| Onset of benefit | Rapid (days) | Slower (weeks to months) |
| Target symptom | Pain, burning, allodynia, sleep | Numbness, paresthesia, vibration/proprioception loss |
This is a symptomatic + neuroprotective/regenerative pairing. Pregabalin provides early pain relief while mecobalamin works on the underlying nerve pathology.
Pregabalin: Mechanism and Evidence
Mechanism of Action
Pregabalin is a structural GABA analog (S-(+)-3-isobutyl GABA) but does not act directly on GABA receptors. It binds selectively to the α2-δ subunit of voltage-dependent calcium channels in the dorsal horn of the spinal cord and dorsal root ganglia. This reduces calcium influx at presynaptic terminals and decreases release of excitatory neurotransmitters - glutamate, noradrenaline, and substance P. The net effect is reduced central sensitization and neuropathic pain signaling. - Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 9897
Pharmacokinetics
- Bioavailability: >90% (linear, dose-proportional - unlike gabapentin)
- Half-life: ~6 hours (requires twice-daily dosing)
- Protein binding: nil
- Metabolism: negligible hepatic metabolism; 95% excreted unchanged in urine
- No drug-drug interactions via CYP enzymes
- Renal dosing required - clearance directly proportional to creatinine clearance
Clinical Efficacy (FDA-approved indications)
- Diabetic peripheral neuropathy (2005)
- Postherpetic neuralgia
- Fibromyalgia
- Neuropathic pain from spinal cord injury
- Adjunct for partial-onset seizures
At 300 mg/day, ~45% of DPN patients achieve ≥50% pain relief. NNT = 2.2 for diabetic neuropathy - which is superior to most other anticonvulsants. Pain, mood, sleep, and quality of life measures all improve. - Bradley & Daroff's Neurology in Clinical Practice, p. 2464
Dosing for Neuropathic Pain
| Phase | Dose |
|---|---|
| Starting | 75 mg twice daily (150 mg/day) |
| After 1 week (if tolerated) | 150 mg twice daily (300 mg/day) |
| Maximum | 300 mg twice daily (600 mg/day) for DPN and PHN |
Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 9900
Mecobalamin (Methylcobalamin): Mechanism and Evidence
Why Methylcobalamin Over Cyanocobalamin for Nerves?
Methylcobalamin is the biologically active coenzyme form that directly participates in:
- Methionine synthase: converts homocysteine → methionine → S-adenosylmethionine (SAM), the key methyl donor for phospholipid synthesis, neurotransmitter methylation, and myelin maintenance
- Promotes axonal transport and regeneration in peripheral nerves
- Schwann cell support: facilitates myelination and remyelination in the peripheral nervous system
Unlike cyanocobalamin, which must be converted intracellularly, methylcobalamin is immediately usable by neurons and has demonstrated direct nerve regeneration effects in experimental studies.
Clinical Role in Neuropathy
- Improves vibration perception threshold, pressure sensation, and thermal sensitivity
- Reduces burning pain and paresthesias (though less potent than pregabalin for pain)
- Addresses the structural defect in the nerve rather than just the pain signal
- Particularly useful in deficiency-related neuropathy, but also studied in DPN where metabolic derangements impair cobalamin utilization
Evidence for the Combination
Key RCT: Sharma et al., 2021 (PMID: 34854403)
A prospective, randomized, open-label parallel-group study in 100 patients with painful diabetic neuropathy compared three groups over 12 weeks:
- Group A: Methylcobalamin alone
- Group B: Methylcobalamin + Pregabalin
- Group C: Methylcobalamin + Duloxetine
| Outcome | Group A (Methylcobalamin alone) | Group B (Methylcobalamin + Pregabalin) | Group C (Methylcobalamin + Duloxetine) |
|---|---|---|---|
| Vibration perception improved | 11.6% | 37.9% | 41.4% |
| Pressure sensation improved | 7.6% | 37.9% | 37.9% |
| Thermal sensitivity improved | 15.4% | 31.1% | 37.9% |
| VAS pain score reduction | 0.58 ± 0.14 | 3.82 ± 0.05 | 4.17 ± 0.48 |
| Adverse effects | 0% | 6.9% | 10.3% |
Key conclusions:
- Methylcobalamin + duloxetine was most efficacious overall
- Methylcobalamin + pregabalin was significantly more effective than methylcobalamin alone across all sensory and pain outcomes
- Pregabalin combination had the better safety profile compared to duloxetine combination (6.9% vs 10.3% adverse effects)
- Methylcobalamin alone was clearly insufficient as monotherapy for painful DPN
The combination was superior to monotherapy for both pain and sensory deficits, while maintaining an acceptable tolerability profile. - Sharma C et al., Indian J Pharmacol 2021
Clinical Indications for the Combination
The pregabalin + mecobalamin combination is most commonly used in:
- Diabetic peripheral neuropathy - the primary indication, addressing both pain (pregabalin) and structural nerve damage (mecobalamin)
- B12 deficiency neuropathy - mecobalamin treats the cause; pregabalin manages pain during recovery
- Chemotherapy-induced peripheral neuropathy - studied as a supportive regimen
- Postherpetic neuralgia - pregabalin for pain; mecobalamin for nerve repair
- Cervical/lumbar radiculopathy - particularly common in South Asian clinical practice
Advantages of the Combination
- Dual-action: one drug addresses pain signaling; the other supports nerve structure and function
- Additive without pharmacokinetic interaction: pregabalin has negligible hepatic metabolism and no CYP interactions; methylcobalamin is a vitamin - no pharmacokinetic conflict between the two
- Different timeline of benefit: pregabalin acts quickly (within days) while mecobalamin provides slower but more structural improvement (weeks to months) - complementary temporal profiles
- Safety: the combination had fewer adverse effects than pregabalin + duloxetine in the above RCT
- Addresses both symptomatic and etiological components in B12-deficient neuropathy
Side Effects and Precautions
Pregabalin
- Common: dizziness, somnolence, peripheral edema, dry mouth, weight gain
- Serious (rare): angioedema, PR interval prolongation, elevated creatine kinase, thrombocytopenia
- Renal dose adjustment mandatory (renally cleared)
- Schedule V controlled substance (abuse potential; can cause euphoria and withdrawal)
- Increased suicidality risk (anticonvulsant class warning)
- Pregnancy category C - avoid unless benefit clearly outweighs risk
Mecobalamin
- Extremely well tolerated; no significant adverse effects at standard doses
- Generally safe in renal impairment
- Avoid prolonged exposure to light (photosensitive molecule)
Practical Prescribing Notes
- The combination is commercially available as fixed-dose combinations (FDC) under several brand names in India and other markets (e.g., Mecofol-P, various combinations with 75 mg pregabalin + 1500 mcg methylcobalamin)
- Standard doses: pregabalin 75-150 mg twice daily + mecobalamin 500-1500 mcg daily (oral or IM)
- In B12 deficiency: start IM mecobalamin for loading before switching to oral
- Monitor renal function and adjust pregabalin dose accordingly
- Warn patients about dizziness/somnolence from pregabalin, especially when starting
Sources:
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, Pregabalin chapter, pp. 9896-9900
- Bradley & Daroff's Neurology in Clinical Practice, Anticonvulsants in Pain, p. 2464
- Goldman-Cecil Medicine, Adjuvant Analgesics, Chapter 26
- Sharma C, Kaur I, Singh H et al. "A randomized comparative study of methylcobalamin, methylcobalamin plus pregabalin and methylcobalamin plus duloxetine in patients of painful diabetic neuropathy." Indian J Pharmacol. 2021;53(5). [PMID: 34854403]
This is a shared conversation. Sign in to Orris to start your own chat.