Physiology of vision opthalmology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have rich, comprehensive content from two authoritative physiology textbooks. Let me compile the full answer:
Physiology of Vision
Sources: Ganong's Review of Medical Physiology 26th Ed. | Costanzo Physiology 7th Ed.
1. Anatomy of the Eye
The eye consists of three concentric layers:
- Outer (fibrous) layer: Cornea anteriorly (transparent, allows light entry) + sclera posteriorly (white, protective)
- Middle (vascular) layer / uvea: Iris, ciliary body, and choroid. The choroid supplies oxygen and nutrients to the retina
- Inner (neural) layer: Retina - contains the photoreceptors
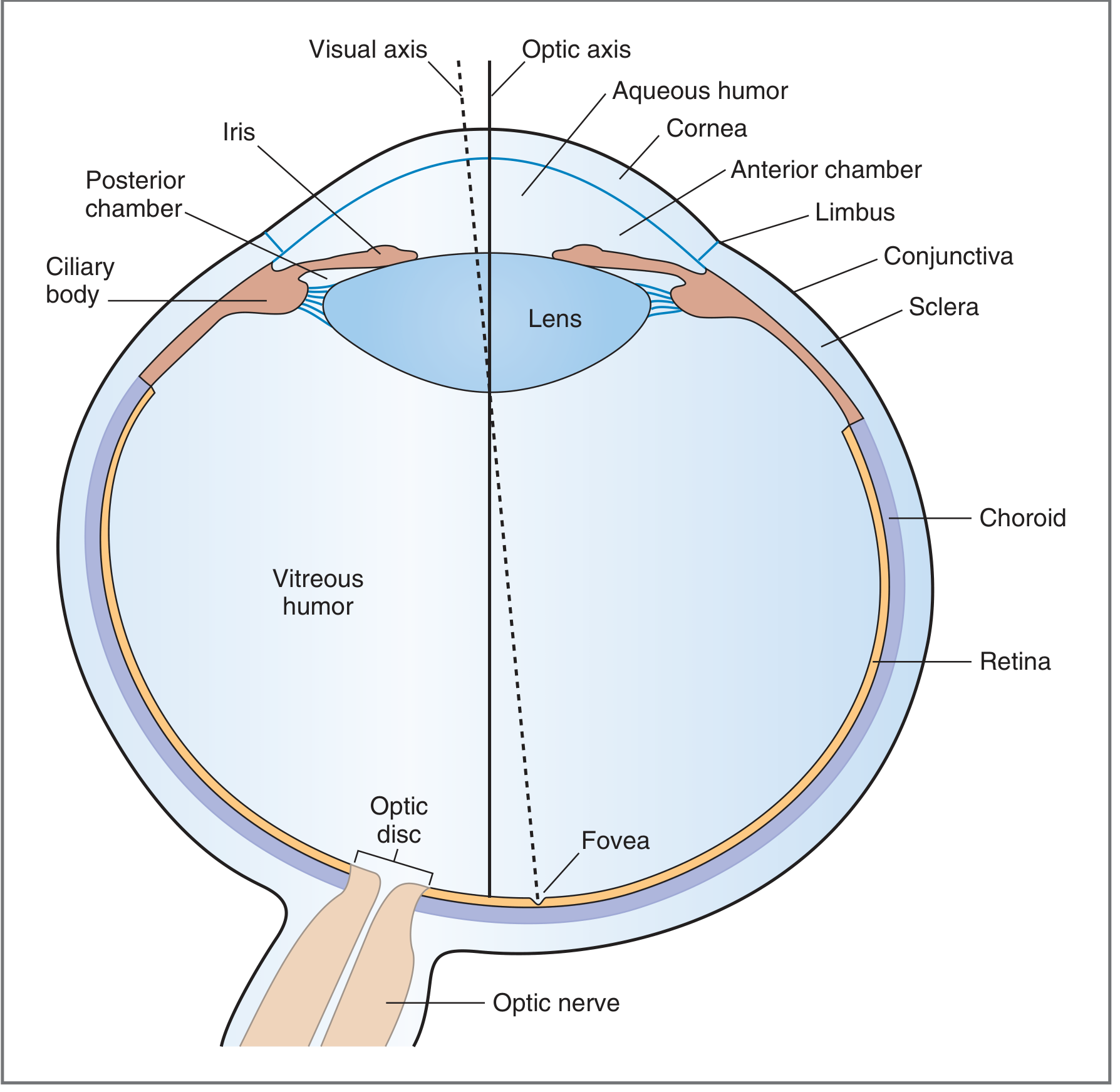
Key structures:
- Cornea: Primary refracting surface (~70% of total refractive power); contributes ~43 diopters
- Lens: Adds ~17 diopters (variable via accommodation); avascular, nourished by aqueous humor
- Iris: Diaphragm controlling pupil size; regulates light entering the eye
- Ciliary body: Produces aqueous humor; contains ciliary muscle for accommodation
- Fovea: Central depression in the macula; highest cone density; point of maximum visual acuity
- Optic disc (blind spot): Where ganglion cell axons exit; no photoreceptors here
- Aqueous humor: Fills anterior chamber; produced by ciliary processes; drains via canal of Schlemm
- Vitreous humor: Gel-like; fills posterior chamber; maintains eye shape
2. Optics and Refraction
Light rays from distant objects are parallel; the relaxed eye focuses them on the retina. Total refractive power of the eye is ~59 diopters.
Accommodation
When focusing on near objects, the ciliary muscle contracts, zonule fibers relax, and the lens becomes more convex - increasing its refractive power. This is controlled by the parasympathetic nervous system (CN III).
Refractive Errors
| Error | Mechanism | Correction |
|---|---|---|
| Myopia (near-sightedness) | Eyeball too long; focus in front of retina | Concave (diverging) lens |
| Hyperopia (far-sightedness) | Eyeball too short; focus behind retina | Convex (converging) lens |
| Astigmatism | Unequal corneal curvature | Cylindrical lens |
| Presbyopia | Age-related loss of lens elasticity | Reading glasses |
Pupillary Light Reflex
- Bright light → afferent signal via CN II → pretectal nucleus (midbrain) → bilateral Edinger-Westphal nuclei → CN III → ciliary ganglion → pupillary constrictor (sphincter pupillae)
- Controls retinal illumination over ~1 log unit; pupils change diameter from ~2 mm to 8 mm
3. The Retina
Layers of the Retina (outer to inner)
- Pigment epithelium - absorbs stray light; recycles retinal (all-trans to 11-cis form)
- Photoreceptor layer - rod and cone outer/inner segments
- Outer nuclear layer - nuclei of photoreceptors
- Outer plexiform layer - synapses between photoreceptors and bipolar/horizontal cells
- Inner nuclear layer - bipolar cells, horizontal cells, amacrine cells
- Inner plexiform layer - synapses between interneurons and ganglion cells
- Ganglion cell layer - output cells of retina
- Optic nerve fiber layer - ganglion cell axons converging to optic disc
Rods vs. Cones
| Feature | Rods | Cones |
|---|---|---|
| Number | ~120 million | ~6 million |
| Distribution | Peripheral retina | Concentrated at fovea |
| Light sensitivity | Very high (scotopic/night vision) | Lower (photopic/day vision) |
| Visual acuity | Low | High |
| Color vision | No | Yes |
| Dark adaptation | Slow (20-30 min) | Fast (5-7 min) |
| Pigment | Rhodopsin | Photopsins (3 types) |
Convergence ratio: ~105 rods+cones → 1.2 million optic nerve fibers (105:1 convergence)
4. Phototransduction
The Dark Current
In darkness, cGMP-gated cation channels in the outer segment are held open by high intracellular cGMP. This allows Na⁺ (and Ca²⁺) influx - the "dark current." The photoreceptor is relatively depolarized (~-40 mV) in the dark and continuously releases glutamate at its synapse.
Response to Light (Rhodopsin Cascade)
- Photon absorption - 11-cis retinal is isomerized to all-trans retinal within rhodopsin
- Rhodopsin activation - conformational change creates metarhodopsin II (activated form)
- Transducin (G-protein) activation - metarhodopsin II activates transducin (Gαt)
- PDE activation - Gαt activates phosphodiesterase (PDE), which hydrolyzes cGMP → 5'-GMP
- Channel closure - cGMP levels fall → cGMP-gated channels close
- Hyperpolarization - Na⁺ influx stops → membrane hyperpolarizes to ~-70 mV
- Reduced glutamate release - hyperpolarization decreases synaptic glutamate release
- Signal propagation - bipolar cells respond to decreased glutamate → ganglion cells fire
Amplification: One photon activates ~500 transducin molecules → closes hundreds of channels. This is why rods can detect a single photon.
Recovery (Dark Adaptation)
- Rhodopsin kinase phosphorylates metarhodopsin II → arrestin binds and inactivates it
- Transducin GTPase hydrolyzes GTP to GDP (self-inactivation)
- Guanylate cyclase regenerates cGMP → channels reopen
- Retinal is reconverted to 11-cis retinal by retinal pigment epithelium (RPE) - this is the slow step of dark adaptation (20-30 minutes)
5. Retinal Signal Processing
Retinal interneurons shape the signal before it leaves the eye:
- Bipolar cells: Direct pathway; can be "ON" (depolarize when light hits center) or "OFF" (hyperpolarize when light hits center) - depends on glutamate receptor type
- Horizontal cells: Lateral inhibition at outer plexiform layer; create surround inhibition
- Amacrine cells: Lateral processing at inner plexiform layer; motion detection, contrast enhancement
- Ganglion cells: Only cells producing all-or-none action potentials; have center-surround receptive fields
Receptive fields have an ON-center/OFF-surround or OFF-center/ON-surround organization, maximizing contrast detection at edges.
6. Visual Pathways
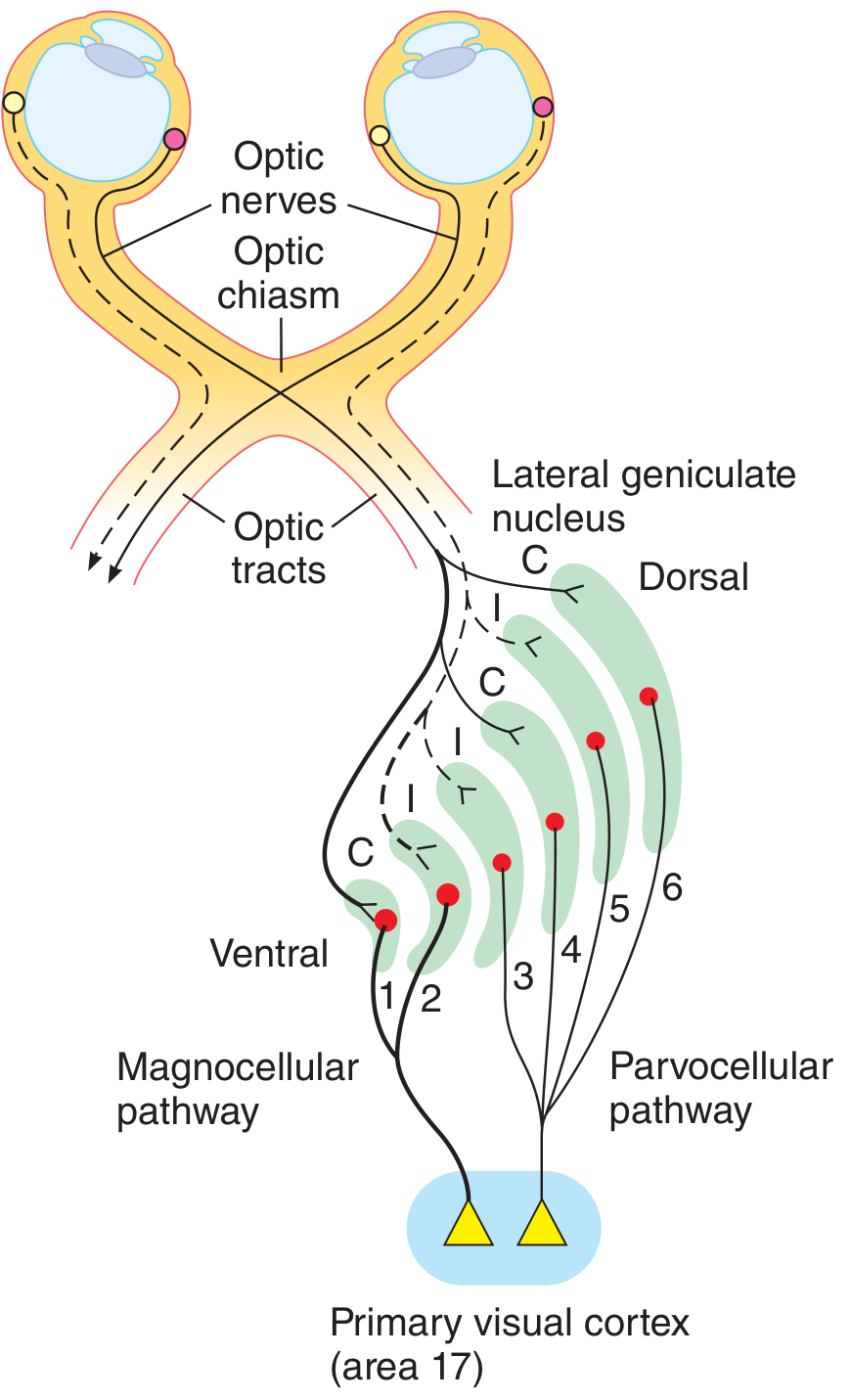
Route: Retina → Visual Cortex
- Optic nerve (CN II) - ganglion cell axons; carries entire visual field from one eye
- Optic chiasm - nasal fibers from each retina decussate (cross); temporal fibers remain ipsilateral
- Optic tract - carries contralateral visual field from both eyes
- Lateral Geniculate Nucleus (LGN) of thalamus - 6 layers:
- Layers 1 & 2: Magnocellular (M pathway) - motion, depth, low-contrast
- Layers 3-6: Parvocellular (P pathway) - color, fine detail, high-contrast
- Layers 1, 4, 6: contralateral eye input
- Layers 2, 3, 5: ipsilateral eye input
- Optic radiations (geniculocalcarine tract) → primary visual cortex (V1, calcarine fissure, area 17)
- Upper fibers: carry lower visual field → upper calcarine cortex
- Lower fibers (Meyer's loop): carry upper visual field → loop through temporal lobe
- Visual association cortex (V2-V5/MT):
- Dorsal "where" stream → parietal cortex (motion, spatial location)
- Ventral "what" stream → temporal cortex (object recognition, faces)
Visual Field Defects from Lesions
| Location | Defect |
|---|---|
| Optic nerve (one side) | Monocular blindness |
| Optic chiasm (center) | Bitemporal hemianopia |
| Optic tract (one side) | Contralateral homonymous hemianopia |
| Meyer's loop (temporal) | "Pie in the sky" - contralateral superior quadrantanopia |
| Parietal radiation | Contralateral inferior quadrantanopia |
| Occipital cortex (one side) | Contralateral homonymous hemianopia with macular sparing |
7. Color Vision
Three types of cones with different photopsin pigments (trichromatic theory):
- S-cones (blue): peak ~420 nm
- M-cones (green): peak ~530 nm
- L-cones (red): peak ~560 nm
Color perception results from comparing the ratio of excitation across these three cone types (opponent-color processing at the retinal ganglion and LGN level).
Color Blindness
- Most common: red-green color blindness (X-linked recessive; 8% males, 0.5% females)
- Protanopia: absent red cones
- Deuteranopia: absent green cones
- Tritanopia: absent blue cones (rare, autosomal)
8. Dark and Light Adaptation
- Light adaptation (going from dark to bright): Cones adapt within 5-7 minutes; rhodopsin bleaches rapidly; pupil constricts; sensitivity decreases
- Dark adaptation (going from bright to dark): Two phases:
- Cones adapt first (5-7 min)
- Rods adapt slowly over 20-30 minutes (limited by rate of rhodopsin regeneration from RPE)
- Purkinje shift: In dim light, peak sensitivity shifts from ~555 nm (cone/photopic) to ~507 nm (rod/scotopic) - blues appear relatively brighter at dusk
9. Pupillary Reflexes (Summary)
| Reflex | Afferent | Center | Efferent | Response |
|---|---|---|---|---|
| Light reflex | CN II | Pretectal nucleus → EW nuclei | CN III | Bilateral miosis |
| Accommodation | Cortex | Convergence center | CN III | Miosis + convergence + accommodation |
| Argyll Robertson pupil | Defective light reflex, intact accommodation | Dorsal midbrain lesion | CN III intact | No light response, but accommodates |
10. Clinical Correlations
- Vitamin A deficiency → deficient rhodopsin synthesis → night blindness (nyctalopia) → if severe, corneal xerosis and Bitot's spots
- Glaucoma → elevated intraocular pressure (impaired aqueous drainage) → optic nerve damage → visual field loss
- Age-related macular degeneration (AMD) → photoreceptor and RPE degeneration at the macula → central vision loss
- Retinitis pigmentosa → rod degeneration (mutations in rhodopsin gene most common) → night blindness → progressive peripheral visual loss → "tunnel vision"
- Diabetic retinopathy → neovascularization, macular edema → blurred vision
Sources:
- Ganong's Review of Medical Physiology, 26th Ed. - Chapter 10: Vision
- Costanzo Physiology, 7th Ed. - Chapter 3: VISION section
Do u hv opthalmology
Finding Sources
Yes! The library has 2 ophthalmology textbooks:
📚 Ophthalmology Books Available
-
Kanski's Clinical Ophthalmology - A Systematic Approach, 10th Edition
- The gold-standard clinical ophthalmology reference
- Covers all major eye conditions systematically (retina, glaucoma, cornea, lens, neuro-ophthalmology, etc.)
-
The Wills Eye Manual - Office and Emergency Room Diagnosis and Treatment of Eye Disease
- Practical clinical reference for diagnosis and management
- Great for emergency eye conditions and outpatient practice
Plus, for physiology of vision (as covered in the previous response), the library also has:
- Ganong's Review of Medical Physiology, 26th Ed. - full chapter on vision
- Costanzo Physiology, 7th Ed. - vision section
Just ask any ophthalmology topic - glaucoma, retinal diseases, corneal disorders, uveitis, strabismus, neuro-ophthalmology, ocular pharmacology, surgical procedures, or anything else - and I'll pull directly from these textbooks!
Ok teach what I write from optha sources only physiology of vision
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
I now have all the content from Kanski's to build a thorough, ophthalmology-specific physiology of vision response. Here it is:
Physiology of Vision
From Kanski's Clinical Ophthalmology, 10th Edition
1. Visual Acuity (VA)
Visual acuity is the most fundamental measure of visual function. It is directly related to the minimum angle of separation (subtended at the nodal point of the eye) between two objects that allow them to be perceived as distinct.
Snellen Visual Acuity
The Snellen chart uses black optotypes (letters/symbols) on a white background, read at a standard distance (6 metres).
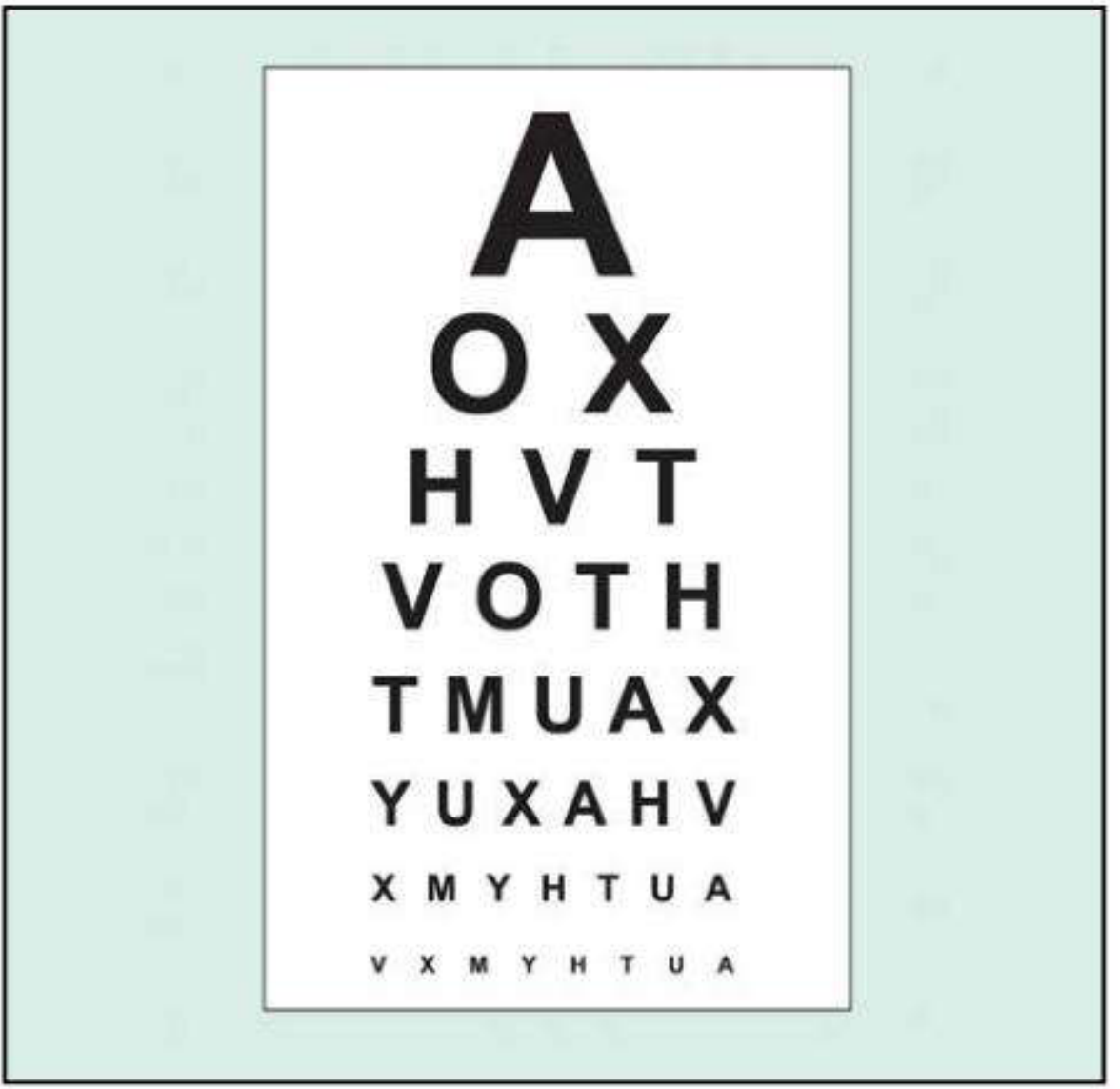
- 6/6 (20/20) = Normal monocular VA in young adults
- 6/X notation: numerator = testing distance (6 m); denominator = distance at which that line's letters subtend 5 arc minutes
- Best-corrected VA (BCVA) = VA achieved with optimal refractive correction
- Pinhole VA: a 1 mm pinhole compensates for refractive error by eliminating peripheral rays. If pinhole VA improves, the deficit is likely refractive. If it worsens, macular or posterior lens pathology should be suspected.
Very Poor VA (in order of severity)
| Level | Meaning |
|---|---|
| Counting Fingers (CF) | Can count fingers held at specified distance (usually 1 m) |
| Hand Movements (HM) | Can distinguish whether examiner's hand is moving |
| Perception of Light (PL) | Can detect only light, no shapes or movement |
| No Perception of Light (NPL) | Completely blind |
Tip: In PL patients with a dense media opacity (e.g. cataract), the direction of light projection should be testable - inability to localise it suggests retinal or optic nerve disease.
LogMAR Acuity
- More precise and statistically valid than Snellen for clinical trials
- LogMAR 0.0 = 6/6; positive values = worse vision, negative = better than 6/6
- Bailey-Lovie chart and ETDRS chart (Early Treatment Diabetic Retinopathy Study) use LogMAR notation; ETDRS has 5 letters per line with equal log steps
Near Visual Acuity
Tested with Jaeger charts or Times New Roman font sizes. Used to assess reading vision.
Contrast Sensitivity
- Measures the ability of the visual system to distinguish an object against its background - a different dimension from spatial resolution
- High contrast targets (e.g. black letters on white) may be read normally even when contrast sensitivity is significantly impaired
- Reduced in: amblyopia, optic neuropathy, some cataracts, higher-order aberrations - even when Snellen VA is preserved
- Pelli-Robson chart: viewed at 1 m; rows of letters of equal size but decreasing contrast in steps of 0.15 log units per group of three letters
- SPARCS (Spaeth-Richman): computer-based; tests both central and peripheral contrast sensitivity using sine-wave gratings
2. Colour Vision
Physiology of Colour Vision
Colour vision depends on three populations of retinal cones, each with specific peak sensitivity:
- S-cones (blue/tritan): peak 414-424 nm
- M-cones (green/deuteran): peak 522-539 nm
- L-cones (red/protan): peak 549-570 nm
Normal colour perception requires all three primary cone types to match wavelengths within the spectrum.
Types of Colour Deficiency
| Term | Meaning |
|---|---|
| Trichromat | All three cone types present (normal or anomalous) |
| Anomalous trichromat | All three types present but one is shifted - most common CVD |
| Dichromat | Only two cone types |
| Monochromat | Only one cone type - total colour blindness |
Congenital Colour Vision Deficiency (CVD):
- X-linked recessive; affects ~8% Northern European men, ~0.5% women
- Prevalence in Black Africans: ~4% men, ~1.5% women
- Protanomaly (2% men): red-cone weakness; Protanopia: red-cone absent
- Deuteranomaly (6% men): green-cone weakness; Deuteranopia: green-cone absent
- Tritanomaly/Tritanopia: blue-cone defect (rare, autosomal)
Acquired colour defects:
- Macular disease → blue-yellow defects
- Optic nerve lesions → red-green defects
Colour Vision Tests
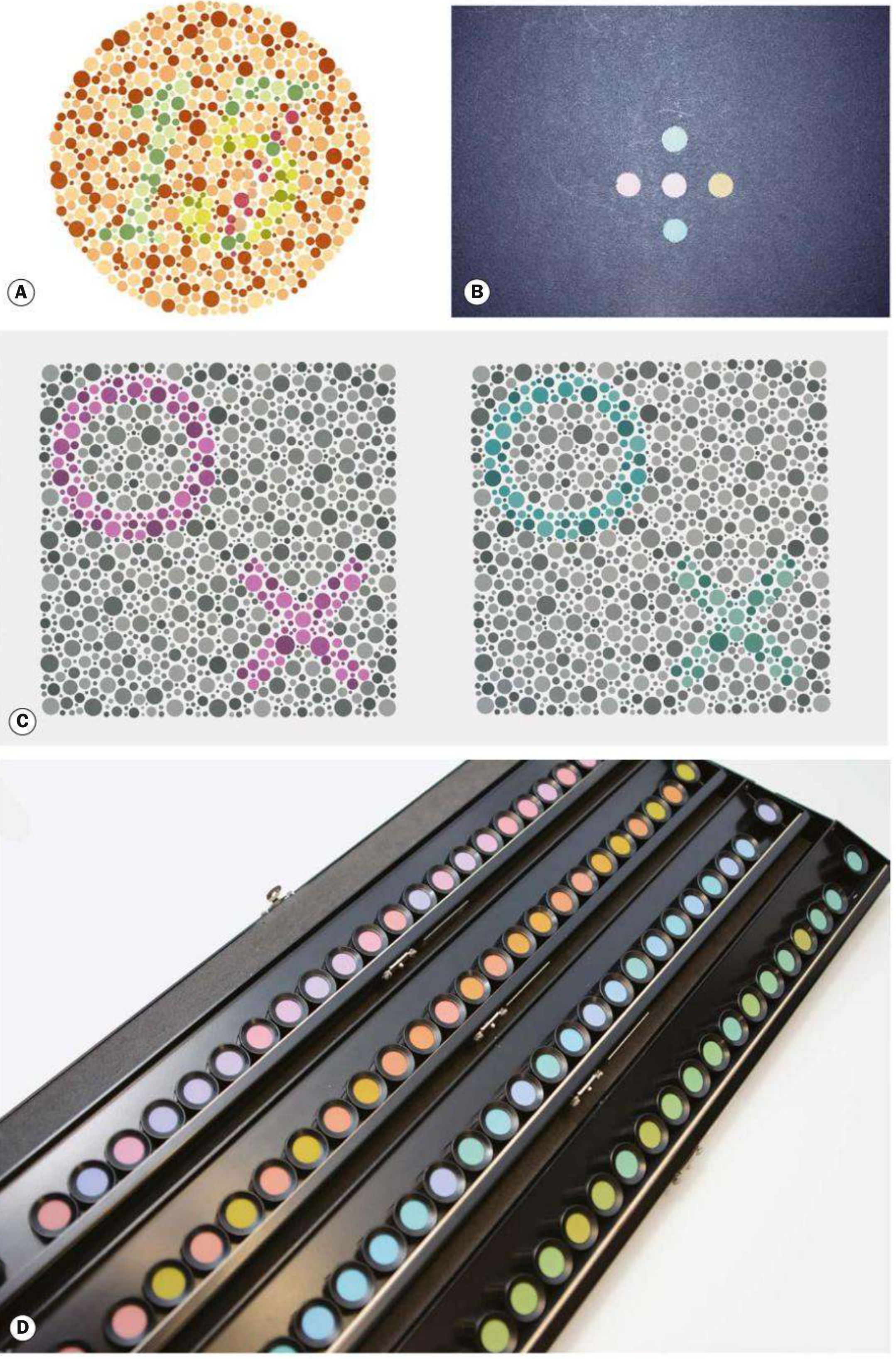
| Test | Purpose | Details |
|---|---|---|
| Ishihara | Screens protan & deuteran defects | 16 plates with dot-matrix numbers; most widely used |
| City University | General colour defect screening | 10 plates; central + 4 peripheral colours to match |
| Hardy-Rand-Rittler (HRR) | All three congenital defects | Detects tritan defects too (unlike Ishihara) |
| Farnsworth-Munsell 100-hue | Sensitive; congenital & acquired | 85 colour caps to arrange in order; quantifies severity and axis of defect |
Tip: Children with congenital CVD may need early career counselling as certain occupations (e.g. pilot, electrician, some military roles) require normal colour vision.
3. Amsler Grid - Testing the Macular Physiology
The Amsler grid evaluates the central 20° of the visual field centred on fixation (corresponding to the macular region).
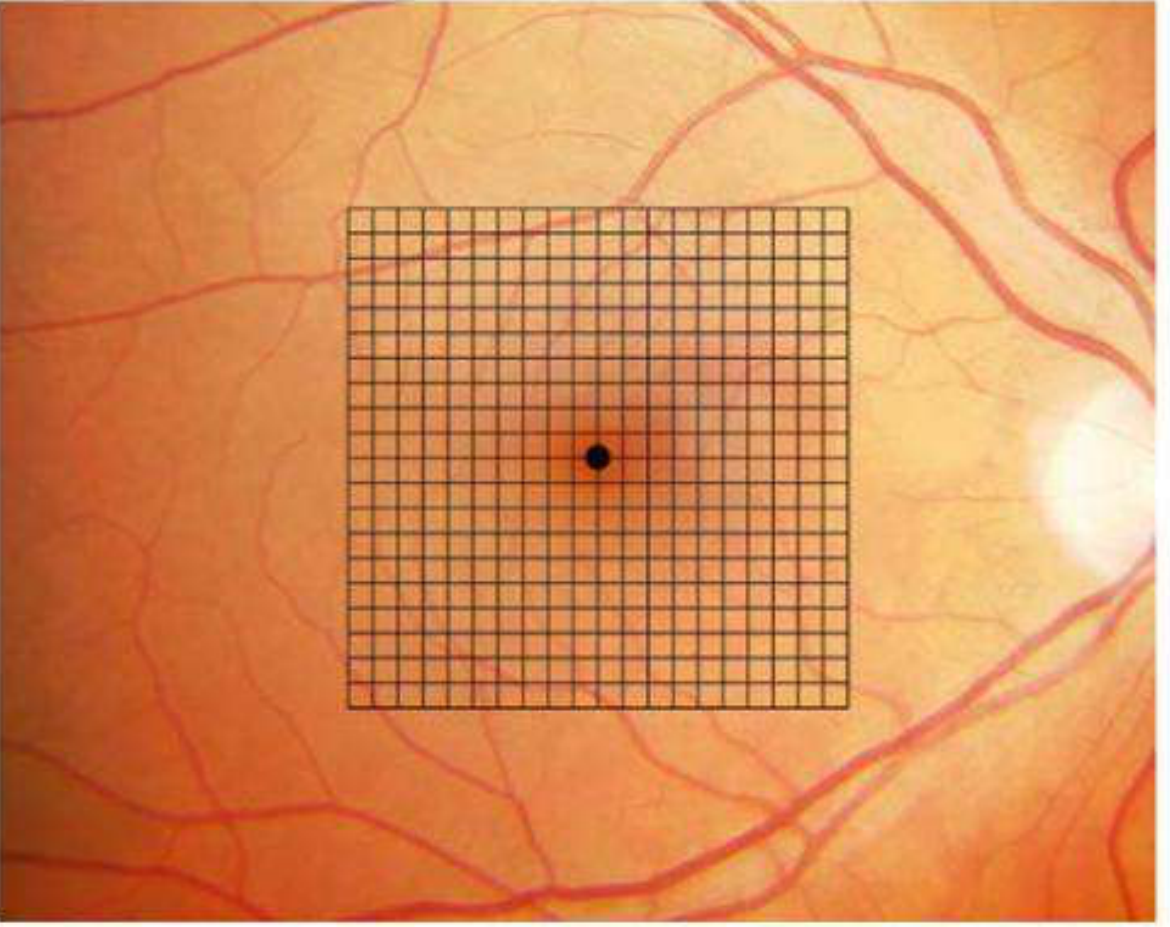
- 7 charts available; Chart 1 is the standard (white grid on black background, 400 squares of 5 mm each)
- Principally used for screening and monitoring macular disease (e.g. AMD, macular oedema)
- Patients with risk of macular neovascularization (MNV) should use it at home regularly
- Abnormal findings: metamorphopsia (distorted lines), scotoma (missing area), micropsia/macropsia
4. Perimetry (Visual Field Testing)
The visual field is the total area in which objects can be seen in peripheral vision while the eye is focused on a central point.
Definitions
- Isopter: line connecting points of equal sensitivity for a given target size and luminance
- Scotoma: area of decreased or absent vision within the visual field
- Threshold: minimum luminance increment detectable at each point in the field
Testing Algorithms
- Threshold testing: determines exact sensitivity at each point; most accurate; used for glaucoma monitoring (e.g. SITA Standard, SITA Fast on Humphrey Field Analyser)
- Suprathreshold testing: simply checks whether a brighter-than-threshold stimulus is seen; faster; used for screening
5. Photostress Test and Light-Brightness Comparison
Photostress Recovery Test
- A bright light is shone into one eye and the time to recover normal VA is measured
- Normal: recovery within ~60 seconds
- Prolonged recovery (>90 s): suggests macular disease (RPE/photoreceptor dysfunction), not optic nerve disease
- Optic nerve disease does NOT prolong photostress recovery
Light Brightness Comparison
- Patient compares the perceived brightness of a light in each eye alternately
- Reduction in one eye suggests ipsilateral optic nerve or extensive retinal disease
- Used to detect relative afferent pupillary defect (RAPD) equivalent on subjective testing
6. Binocular Vision Physiology
Binocular vision requires precise coordination of both eyes. Kanski's describes three grades:
Grades of Binocular Single Vision (Worth's classification)
| Grade | Level | Description |
|---|---|---|
| 1st degree | Simultaneous macular perception | Both eyes perceive simultaneously; no fusion yet |
| 2nd degree | Fusion | Brain combines the two images into one; can measure fusional reserves |
| 3rd degree | Stereopsis | Appreciation of depth from slight horizontal disparity between the two retinal images |
Field of Binocular Single Vision
- The binocular field is the overlapping region where both eyes can see simultaneously
- Normally extends ~60° to each side of fixation in the horizontal plane
- Restricted in: strabismus, cranial nerve palsies, orbital disease
7. Cone Physiology - Enhanced S-cone Syndrome (Kanski clinical example)
Kanski uses Enhanced S-cone syndrome to illustrate normal cone physiology:
"The human retina has three photoreceptor types: short-wave sensitivity (S), middle-wave sensitivity (M) and long-wave sensitivity (L). Most inherited retinal dystrophies exhibit progressive attenuation of rods and all classes of cones. However, enhanced S-cone syndrome is characterized by hyper-function of S-cones and severe impairment of M- and L-cones, with non-recordable rod function."
- The gene implicated is NR2E3 (AR inheritance), encoding a ligand-dependent transcription factor that normally suppresses S-cone fate during development
- Clinically: nyctalopia (night blindness), reduced colour vision (tritan axis preserved), cystoid maculopathy, vitreous degeneration
- ERG: no rod response; scotopic maximum response mimics photopic ERG waveform
This demonstrates that each cone class has a genetically programmed role in the trichromatic system.
Summary: Clinical Tests of Visual Physiology at a Glance
| Function | Test | Key Principle |
|---|---|---|
| Visual resolution | Snellen / LogMAR / ETDRS | Minimum angle of resolution |
| Refractive error | Pinhole VA | Eliminates peripheral/aberrant rays |
| Macular function | Amsler grid, photostress test | Central 20°; RPE-photoreceptor interface |
| Colour vision | Ishihara, FM 100-hue, HRR | Cone type-specific wavelength processing |
| Contrast sensitivity | Pelli-Robson, SPARCS | Spatial frequency processing independent of VA |
| Visual field | Perimetry (Humphrey/Goldmann) | Threshold sensitivity across the retinal map |
| Binocular vision | Worth 4-dot, stereo tests | Cortical fusion and stereopsis |
| Optic nerve function | RAPD (swinging torch), colour desaturation, brightness comparison | Afferent pathway integrity |
Source: Kanski's Clinical Ophthalmology - A Systematic Approach, 10th Edition
Visual pathway
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content directly from Kanski's. Let me compile the full visual pathway response:
Visual Pathway
From Kanski's Clinical Ophthalmology, 10th Edition (Neuro-ophthalmology chapter)
Overview of the Visual Pathway
The visual pathway transmits signals from the retinal photoreceptors to the visual cortex. It consists of six anatomical segments, each producing characteristic visual field defects when damaged:
Retina → Optic Nerve → Optic Chiasm → Optic Tract
→ Lateral Geniculate Body → Optic Radiations → Visual Cortex (V1)
1. Retina
- Each retina is divided by a vertical meridian through the fovea into a nasal hemiretina (medial) and a temporal hemiretina (lateral)
- The temporal hemiretina sees the nasal visual field; the nasal hemiretina sees the temporal visual field
- Ganglion cell axons converge at the optic disc to form the optic nerve
- The macula has a disproportionately large cortical representation (magnification factor)
2. Optic Nerve (CN II)
- Carries all visual information from one eye only
- Surrounded by meninges (dura, arachnoid, pia) and bathed in CSF - explains why raised ICP causes papilloedema
- Four segments: intraocular (optic disc) → intraorbital (25 mm, sinuous to allow eye movement) → intracanalicular (6 mm, tightest space - most vulnerable to compression) → intracranial (10 mm)
- A lesion here causes monocular visual loss (ipsilateral eye only)
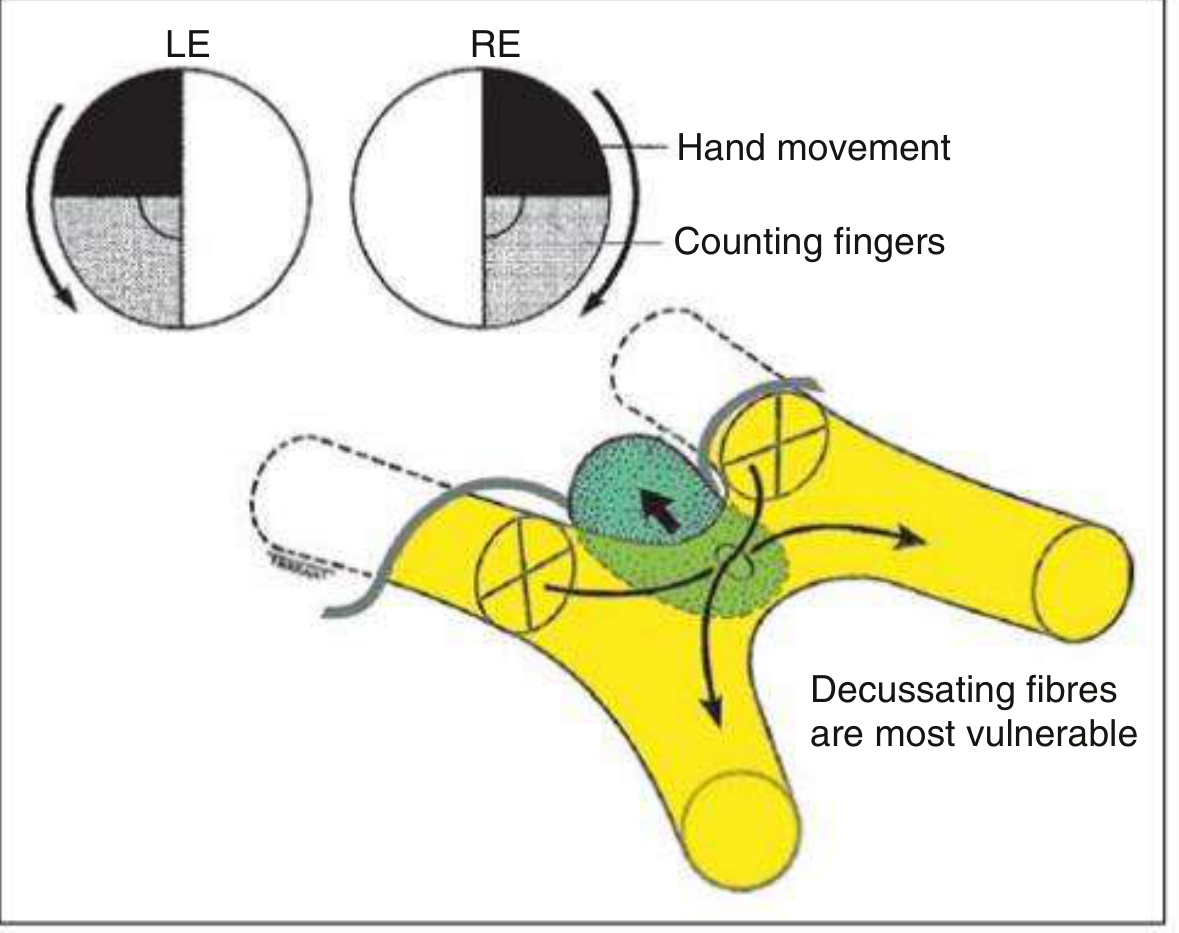
3. Optic Chiasm
The chiasm is the key crossing point of the visual pathway.
Anatomy at the Chiasm
- Nasal fibres (from each eye's nasal hemiretina, carrying temporal field information) decussate (cross) to the opposite optic tract
- Temporal fibres (from each eye's temporal hemiretina, carrying nasal field information) do NOT cross - they remain ipsilateral
- The macular fibres run centrally through the chiasm
Anatomical Variations (Position of Chiasm)
- Normal (~79%): chiasm lies above the pituitary fossa (sella turcica)
- Prefixed (~9%): chiasm lies anterior - the optic tracts are long and more vulnerable; pituitary lesions affect tracts, not chiasm
- Postfixed (~12%): chiasm lies posteriorly - pituitary lesions may affect optic nerves
Fibre Arrangement at Chiasm
- Lower nasal fibres run inferiorly and anteriorly through the chiasm → affected first by expanding pituitary lesions growing upward from below → produces upper temporal quadrantanopia progressing to bitemporal hemianopia
- Upper nasal fibres run high and posteriorly → affected first by craniopharyngioma (arising above the chiasm) → lower temporal quadrantanopia first
- Wilbrand's knee: lower nasal fibres from one eye loop briefly into the contralateral optic nerve before crossing - a lesion at the junction of one optic nerve and chiasm produces an ipsilateral central scotoma + contralateral upper temporal quadrantanopia (junctional scotoma)
Classic Chiasmal Field Defect
Bitemporal hemianopia - loss of both temporal fields - is pathognomonic of chiasmal compression
Clinical signs of chiasmal compression:
- Colour desaturation across the vertical midline of the visual field is an early sign - test by moving a red target from nasal to temporal field; asymmetry is significant
- Optic atrophy (present in ~50% with field defects): nasal fibre loss → "bow-tie / band atrophy" of the optic disc (temporal and nasal disc pallor only)
- Papilloedema is rare with chiasmal lesions
Common causes of chiasmal compression:
- Pituitary adenoma (most common)
- Craniopharyngioma (tends to compress from above)
- Meningioma (tuberculum sellae, olfactory groove)
- Aneurysm (anterior communicating artery, internal carotid)
- Glioma
4. Optic Tract
- Arises at the posterior chiasm, diverges, and wraps around the cerebral peduncles to terminate in the lateral geniculate body (LGB)
- Each optic tract carries:
- Crossed fibres from the contralateral nasal hemiretina
- Uncrossed fibres from the ipsilateral temporal hemiretina
- Combined: represents the contralateral visual hemifield of both eyes
- Nerve fibres from corresponding retinal points are not yet aligned in the tract → field defects are incongruous
Optic Tract Lesion → Contralateral incongruous homonymous hemianopia
Wernicke Hemianopic Pupil
- The optic tract contains both visual fibres (→ LGB) AND pupillomotor fibres (→ leave tract before LGB → brachium of superior colliculus → pretectal nuclei)
- An optic tract lesion may produce an afferent pupillary defect: light shone onto the hemianopic side produces a weaker pupillary response than light shone onto the seeing side
- This is called the Wernicke hemianopic pupillary reaction - difficult to elicit in practice due to scatter of light within the eye; a fine beam is needed
Optic Atrophy After Tract Lesion
- Ipsilateral disc: "bow-tie atrophy" (superior and inferior rim pallor from temporal fibre loss)
- Contralateral disc: diffuse/simple atrophy (nasal fibre loss)
5. Lateral Geniculate Body (LGB)
- A thalamic relay nucleus on each side
- 6 well-defined laminar layers:
- Layers 1-2: Magnocellular (M pathway) - motion, depth, coarse form
- Layers 3-6: Parvocellular (P pathway) - colour, fine detail, high acuity
- Layers 1, 4, 6: contralateral eye input
- Layers 2, 3, 5: ipsilateral eye input
- Retinotopic map is maintained
- Lesions here produce asymmetric / sectoral homonymous field defects (due to dual blood supply from anterior and posterior circulations)
6. Optic Radiations (Geniculocalcarine Tract)
Fibres leave the LGB and fan out as the optic radiations to reach the primary visual cortex. They divide into three groups:
a. Temporal (Inferior) Radiations - Meyer's Loop
- Carry fibres from the inferior retina (representing the superior visual field)
- Loop anteriorly and inferiorly into the temporal lobe (most anterior extent = Meyer's loop, reaching the tip of the temporal horn of lateral ventricle)
- Lesion → Contralateral superior homonymous quadrantanopia ("pie in the sky")
- Caused by: temporal lobe tumours, temporal lobectomy for epilepsy
b. Anterior Parietal Radiations
- Carry fibres from the superior retina (representing the inferior visual field)
- Run directly posteriorly through the parietal lobe
- Lesion → Contralateral inferior homonymous quadrantanopia ("pie on the floor")
- Often associated with: dominant parietal lobe signs (acalculia, agraphia, left-right disorientation, Gerstmann syndrome); non-dominant signs (dressing apraxia, spatial neglect)
c. Main (Deep Parietal) Radiations
- Carry all fibres; run deep to the parietal lobe, external to the lateral ventricle trigone
- Lesion → Complete contralateral homonymous hemianopia
7. Primary Visual Cortex (V1 / Area 17 / Striate Cortex)
- Located in the calcarine fissure of the occipital lobe
- Upper lip of calcarine = lower visual field; lower lip = upper visual field
- Posterior pole = macular representation (large cortical area); anterior cortex = peripheral field
- Dual blood supply to occipital cortex (MCA + PCA) protects the macula → lesions often produce macular sparing
Occipital Cortex Lesion → Contralateral homonymous hemianopia with macular sparing
OKN (Optokinetic Nystagmus) - Cogan Dictum
Used to distinguish parietal vs. occipital lesions:
- Parietal lesion: OKN asymmetrical - erratic when drum rotated towards the side of the lesion (smooth pursuit pathways damaged); more likely to be a tumour
- Occipital lesion: OKN symmetrical (smooth pursuit intact); more likely an infarction
8. Pupillary Light Reflex Pathway (parallel to visual pathway)
4 neurones (per Kanski's):
| Neurone | Course |
|---|---|
| 1st (sensory) | Retina → optic nerve → chiasm → optic tract → pretectal nucleus (midbrain, level of superior colliculi). Nasal fibres cross; temporal fibres ipsilateral → bilateral pretectal input from each eye |
| 2nd (internuncial) | Each pretectal nucleus → both Edinger-Westphal (EW) nuclei → therefore uniocular light → bilateral symmetrical constriction (consensual reflex). Damage here → light-near dissociation |
| 3rd (preganglionic motor) | EW nucleus → CN III → ciliary ganglion in the orbit |
| 4th (postganglionic) | Ciliary ganglion → short ciliary nerves → sphincter pupillae (miosis) |
Note: Pupillomotor fibres leave the optic tract before the LGB → an optic tract lesion can produce a RAPD (Wernicke hemianopic pupil), but LGB or more posterior lesions do NOT affect the pupil
Summary: Visual Field Defects by Lesion Location
| Site | Field Defect | Key Features |
|---|---|---|
| Optic nerve | Monocular visual loss / central scotoma | RAPD present; disc changes ipsilateral |
| Optic chiasm (central) | Bitemporal hemianopia | Pituitary/craniopharyngioma; bow-tie atrophy |
| Junctional (nerve-chiasm) | Ipsilateral central scotoma + contralateral upper temporal quadrantanopia | Wilbrand's knee |
| Optic tract | Contralateral incongruous HH | Wernicke hemianopic pupil; RAPD |
| LGB | Asymmetric/sectoral HH | Dual blood supply pattern |
| Temporal radiation (Meyer's loop) | Contralateral superior quadrantanopia ("pie in sky") | Temporal lobe surgery/tumour |
| Parietal radiation | Contralateral inferior quadrantanopia ("pie on floor") | Parietal signs; OKN asymmetrical |
| Occipital cortex | Contralateral HH with macular sparing | OKN symmetrical; infarction |
| Bilateral occipital | Cortical blindness | Pupils normal; Anton syndrome (denial of blindness) |
HH = Homonymous Hemianopia
9. Higher Visual Processing - Cerebral Visual Impairment (CVI)
Beyond V1, visual information flows through two cortical streams:
- Dorsal stream ("where" pathway): V1 → posterior parietal lobes via superior longitudinal fasciculus. Creates a real-time 3D map of surroundings for visually guided movement. Damage → Balint syndrome (optic ataxia, oculomotor apraxia, simultagnosia)
- Ventral stream ("what" pathway): V1 → temporal lobes. Object recognition, faces, colour. Damage → prosopagnosia, visual agnosia
CVI is the most common cause of visual disability in children in industrialised countries (affects up to 3% of school children). Causes: hypoxia/ischaemia, prematurity, meningitis. Characterised by: difficulty with visual complexity, visual field preference, slow visual latency, preference for moving targets.
Source: Kanski's Clinical Ophthalmology - A Systematic Approach, 10th Edition, Neuro-ophthalmology Chapter
Errors of refraction
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive content from Kanski's to deliver a thorough answer on errors of refraction. Here it is:
Errors of Refraction
From Kanski's Clinical Ophthalmology, 10th Edition
Basic Concepts
Emmetropia
The normal state: parallel rays of light from a distant object are focused exactly on the retina by the relaxed (non-accommodating) eye. No refractive correction is needed for distance.
Ametropia
Any deviation from emmetropia - the eye has a refractive error. Light does not focus on the retina in the relaxed state. Includes: myopia, hypermetropia, astigmatism, and presbyopia.
The Unit: Dioptre (D)
- 1 dioptre = the power of a lens with a focal length of 1 metre
- The eye's total refracting power = ~59 D (cornea ~43 D + lens ~16 D)
- Refractive errors are measured in dioptres
1. Myopia (Short-sightedness / Near-sightedness)
Definition
The parallel rays of light from a distant object come to a focus in front of the retina in the unaccommodated eye. Near objects can be seen clearly (hence "near-sighted").
Types/Causes
- Axial myopia (most common): eyeball is too long (axial length > normal ~24 mm)
- Refractive/curvature myopia: corneal or lens curvature is too steep (excessive power)
- Index myopia: increased refractive index of lens (e.g. early nuclear cataract - "second sight")
Symptoms
- Blurred distance vision; clear near vision
- Squinting to see distant objects
- Headaches from effort to focus
Classification by degree
| Category | Myopia |
|---|---|
| Low | Up to -3 D |
| Moderate | -3 to -6 D |
| High | More than -6 D |
Correction
- Concave (diverging, minus) lens - diverges incoming rays so they focus further back (on retina)
- Spectacles, contact lenses, or refractive surgery
Refractive Surgery Options for Myopia (Kanski's)
- LASIK: central ablative flattening of corneal stroma; corrects up to -6 to -8 D (limited by corneal thickness; residual bed ≥250 µm must remain)
- Surface ablation (PRK/LASEK): for lower myopia; slower visual recovery; reduced risk of flap complications
- SMILE (Small Incision Lenticule Extraction): small incision laser technique; no flap; corrects myopia and myopic astigmatism
- Phakic IOL (iris-clip 'lobster claw' or posterior chamber): for high myopia beyond laser range; natural lens retained
- Clear lens exchange: removes natural lens; risk of retinal detachment in high myopes
2. Hypermetropia (Hyperopia / Long-sightedness / Far-sightedness)
Definition
Parallel rays from a distant object focus behind the retina in the unaccommodated eye. The eye is not long enough or has insufficient refractive power.
Types/Causes
- Axial hypermetropia (most common): eye is too short
- Refractive hypermetropia: cornea or lens too flat (insufficient power)
Important clinical subtlety: Accommodation can mask hypermetropia
Young patients use their accommodation (ciliary muscle contraction, lens rounding) to compensate for hypermetropia - this is called latent hypermetropia. They may be asymptomatic until the demand on accommodation becomes excessive or accommodation begins to fail with age.
- Manifest hypermetropia = portion revealed without cycloplegia
- Latent hypermetropia = masked by accommodation; revealed only under cycloplegia
- Total hypermetropia = manifest + latent (only measurable under full cycloplegia)
This is why cycloplegic refraction (with cyclopentolate or atropine) is essential in children, especially for strabismus evaluation - accommodation can completely mask the true refractive error.
Symptoms
- Blurred near vision (worse at near than distance)
- Eyestrain (asthenopia), headaches after reading
- In significant hypermetropia: blurred distance vision too
- In children: convergent squint (esotropia) - hypermetropia triggers excess accommodation → excess convergence → esotropia
Refraction in Childhood (Kanski's)
- At birth: most babies are hypermetropic
- After age 2: may increase until ~6 years, then levels off and decreases (emmetropisation)
- Prescribing guidelines:
- Up to 4 D without a squint: usually do not correct unless symptomatic
-
4 D: give two-thirds correction
- With esotropia present: prescribe full cycloplegic correction even under age 2
Correction
- Convex (converging, plus) lens - converges light rays so they focus further forward (on retina)
- LASIK: corrects up to +3-4 D
- Conductive Keratoplasty (CK): radiofrequency energy to peripheral corneal stroma → thermal shrinkage → central steepening → treats low-moderate hypermetropia; disadvantages: regression, induced astigmatism
3. Astigmatism
Definition
The refracting surface (usually the cornea) has unequal curvature in different meridians - it is not perfectly spherical. Rays in one meridian are focused at a different point than rays in the perpendicular meridian. There is no single point focus - instead, two focal lines (Sturm's conoid).
Types
- Regular astigmatism: principal meridians are at 90° to each other (correctable with cylindrical lenses)
- With-the-rule: steeper meridian is vertical (corrected by plus cylinder at 90°)
- Against-the-rule: steeper meridian is horizontal (plus cylinder at 180°)
- Oblique: principal meridians are between 30°-60° and 120°-150°
- Irregular astigmatism: meridians not at 90° (e.g. keratoconus, corneal scarring) - NOT correctable with spectacles; needs rigid contact lenses
Symptoms
- Blurred vision at all distances
- Distorted or tilted images
- Eyestrain and headaches
- Tendency to squint or tilt the head
Correction
- Cylindrical (toric) lenses in spectacles or toric contact lenses
- Surgical:
- Limbal relaxing incisions / arcuate keratotomy: paired arcuate incisions in the steep meridian → flattening of that meridian; useful post-keratoplasty
- LASIK/PRK: up to 5 D (LASIK) / 3 D (PRK/LASEK)
- Toric IOL: intraocular lens incorporating cylindrical correction; risk of post-op rotation off-axis
- Conductive keratoplasty: for hypermetropic astigmatism
Astigmatism in childhood
- A cylinder of ≥1 D should be corrected; decreases in significance after the age of about 2 years
4. Presbyopia
Definition
Age-related progressive loss of accommodation (the ability to increase the power of the lens for near vision). Not a true refractive error in the classic sense but a physiological change.
Mechanism
- The crystalline lens progressively hardens (loss of elasticity) with age
- Even when the ciliary muscle contracts, the lens can no longer change shape (become more convex) adequately
- Typically becomes symptomatic around age 40-45
Symptoms
- Difficulty reading or doing near work - patient holds reading material further away
- Headaches and eyestrain with near tasks
- Worse in dim light (pupil dilates → more peripheral/aberrated rays used)
Correction
Unique challenge - correction of presbyopia achieves consistently satisfactory results less reliably than correction of other refractive errors.
Non-surgical:
- Reading glasses (simple plus lens) - for near only
- Bifocals - upper distance, lower near segment
- Progressive addition lenses (PALs) - gradual transition from distance to near; no visible segment line
- Monovision contact lenses: one eye corrected for distance, fellow eye for near
Surgical:
- Multifocal / trifocal / extended depth-of-focus (EDOF) IOLs: implanted after clear lens exchange; can restore reading vision; side effects: nocturnal glare, halos, reduced contrast sensitivity; multifocal IOL is a contraindication to pilot licence in some jurisdictions
- Monovision IOL targeting: dominant eye for distance, non-dominant for near
- PresbyLASIK: alters corneal asphericity to create multifocal effect; benefit over monofocal ablation not yet clearly established
- Intracorneal inlays: (a) refractive, (b) reshaping, (c) small aperture types; placed in stromal pocket or under LASIK flap; complications include decentration, dry eye, vascularisation
- Conductive keratoplasty (CK): can impart some degree of multifocal functionality
- Scleral expansion surgery: inconsistent and unpredictable results
5. Anisometropia
- Unequal refractive errors between the two eyes
- Causes aniseikonia (unequal retinal image sizes)
- If significant, the brain suppresses the blurred image → amblyopia in childhood
- Treat with full refractive correction; if amblyopia present, add occlusion therapy
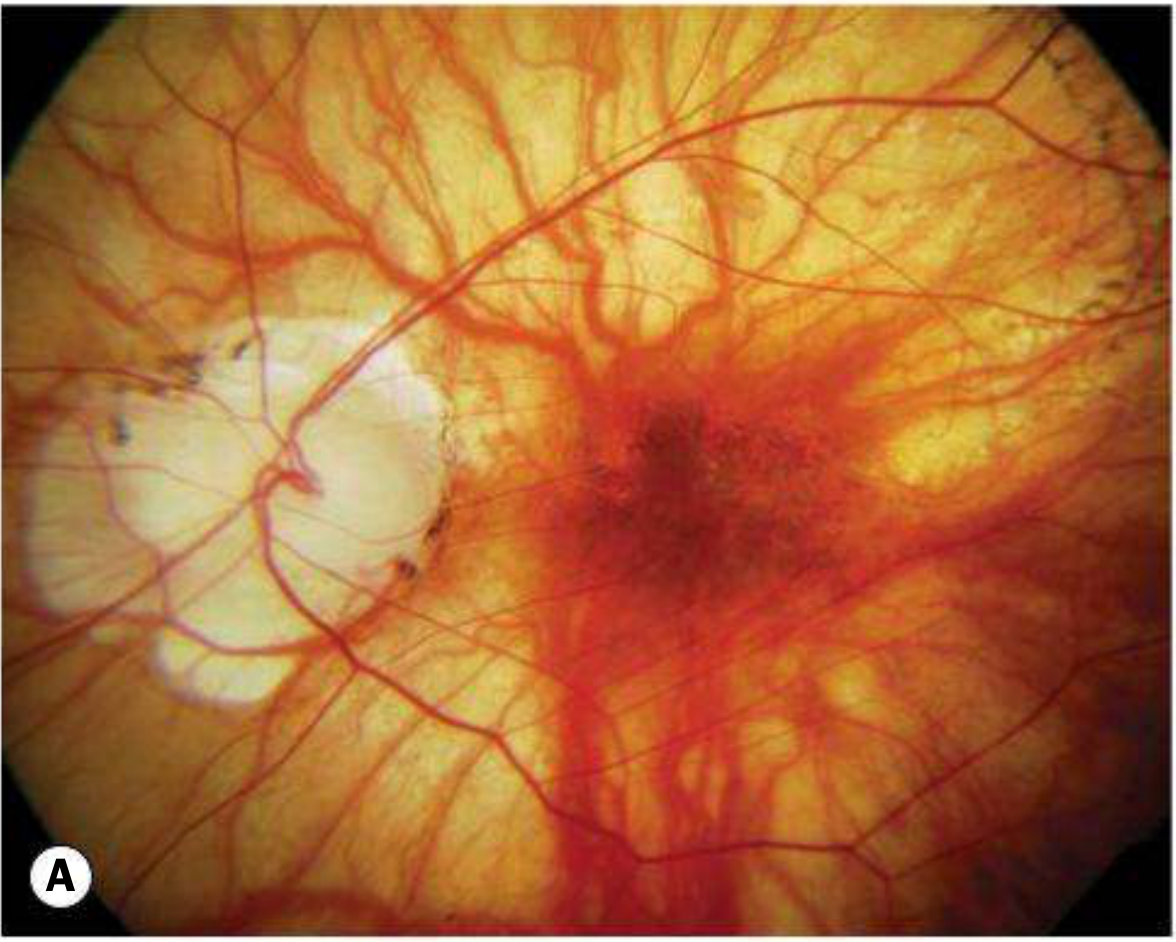
6. High Myopia and Degenerative (Pathological) Myopia
High myopia (>-6 D) is a distinct clinical entity with serious structural consequences, covered extensively in Kanski's.
Definition & Epidemiology
- Axial length usually >26 mm
- Affects >2% of Western adults; up to 10% in East Asians
- A significant cause of legal blindness; maculopathy is the most common cause of visual loss
Pathogenesis
Progressive anteroposterior scleral elongation → mechanical stretching of all posterior ocular structures (RPE, Bruch's membrane, choroid, retina)
Fundus Features of High/Degenerative Myopia
| Feature | Description |
|---|---|
| Tessellated (tigroid) fundus | Pale background from RPE attenuation; choroidal vessels visible |
| Focal chorioretinal atrophy | Patchy visibility of choroidal vessels and sclera |
| Peripapillary atrophy | Temporal crescent of absent RPE around disc; very common |
| Tilted disc | Anomalous optic nerve head appearance |
| Lacquer cracks | Fine yellow irregular lines in RPE-Bruch's complex (~5% of high myopes); can be complicated by MNV |
| Subretinal 'coin' haemorrhages | From lacquer cracks without MNV |
| Fuchs spot | Pigmented scar at macula from old MNV |
| Posterior staphyloma | Localised scleral ectasia at posterior pole |
Complications
- MNV (myopic neovascularisation): 10% of highly myopic eyes
- Rhegmatogenous retinal detachment: much more common (lattice degeneration, PVD, atrophic holes)
- Myopic traction maculopathy, myopic macular hole
- Increased risk of glaucoma and cataract
- (Peri)papillary intrachoroidal cavitation: mimics glaucomatous field defects on perimetry
Systemic Associations of High Myopia (Kanski's Table 14.4)
- Down syndrome
- Marfan syndrome
- Stickler syndrome
- Prematurity
- Noonan syndrome
- Ehlers-Danlos syndrome
- Pierre-Robin syndrome
Myopia Progression Control in Children (Kanski's)
- Low-dose atropine 0.01% at bedtime: significantly slows progression in children 5-15 years whose myopia is increasing >1 D/year
- Time outdoors in sunshine: encouraged; protective effect
- High-add (+2.50 D) multifocal soft contact lens: BLINK trial shows dose-dependent slowing in ages 7-11 years with <5 D myopia
Summary Table: Errors of Refraction
| Error | Focal Point | Axial Length | Lens Needed | Surgery |
|---|---|---|---|---|
| Emmetropia | On retina | Normal | None | - |
| Myopia | In front of retina | Too long | Concave (-) | LASIK, SMILE, phakic IOL |
| Hypermetropia | Behind retina | Too short | Convex (+) | LASIK (up to +4D), CK |
| Astigmatism | Two focal lines | Normal/variable | Cylindrical (toric) | LASIK, arcuate keratotomy, toric IOL |
| Presbyopia | Behind retina (near objects) | Normal | Plus (reading) | Multifocal IOL, monovision, inlays |
Source: Kanski's Clinical Ophthalmology - A Systematic Approach, 10th Edition, Chapters 8 (Refractive Procedures) & 14 (Degenerative Myopia) & Chapter on Strabismus/Paediatric Ophthalmology
Refraction surgery
Finding Sources
Reading File
Reading File
Reading File
Excellent - I now have full content from Kanski's on LASIK, surface ablation (PRK/LASEK/LASEK), SMILE, phakic IOLs, and complications. Let me compile the comprehensive response:
Refractive Surgery
From Kanski's Clinical Ophthalmology, 10th Edition (Chapter 8)
Overview
Refractive surgery encompasses a range of procedures aimed at changing the refraction of the eye by altering the cornea or lens - the principal refracting components. Myopia, hypermetropia, and astigmatism can all be addressed. Correction of presbyopia remains less reliably achievable.
Patient Selection and Preoperative Assessment
Who is a candidate?
- Patients with stable refractive error (stable for at least 1 year before laser surgery)
- Those who desire freedom from spectacles/contact lenses
- Adults with realistic expectations
Contraindications (Kanski's)
- Unacceptably high patient expectations
- Dry eye syndrome
- Non-stable refractive error
- Systemic diseases: SLE, rheumatoid arthritis, immunocompromise
- Ocular disease: chronic blepharitis, previous herpes simplex keratitis, glaucoma, macular degeneration
- Keratoconus or forme fruste keratoconus (risk of ectasia)
Contact Lens Cessation Before Assessment
- Soft contact lenses: discontinue 2 weeks before
- Rigid gas-permeable (RGP) lenses: discontinue at least 3 weeks (some surgeons recommend 1 week per year of wear) - to allow corneal distortion to settle before keratometry
Preoperative Evaluation (for LASIK)
- Complete ocular examination
- Tear film osmolarity - to exclude dry eye syndrome
- Corneal pachymetry - to determine residual stromal bed thickness and exclude keratoconus
- Corneal topography - to exclude irregular astigmatism, keratoconus, forme fruste keratoconus, pellucid marginal degeneration
- Corneal OCT - produces an epithelial map
- Corneal and whole-eye wavefront aberrometry
Occupational Considerations
- Pilots, air-traffic controllers, truck drivers, marksmen, military personnel need to understand the limitations of refractive surgery and the implications before proceeding
- In some jurisdictions, multifocal IOL implantation is a contraindication to holding a private or commercial pilot's licence or to military service
Classification of Refractive Procedures
Refractive Surgery
├── CORNEAL PROCEDURES
│ ├── Laser (excimer)
│ │ ├── Surface ablation (PRK, LASEK, TransPRK/TPRK)
│ │ └── LASIK (flap + excimer)
│ ├── Femtosecond laser
│ │ └── SMILE (lenticule extraction)
│ ├── Incisional
│ │ ├── Radial keratotomy (RK) - historical
│ │ └── Arcuate keratotomy / Limbal relaxing incisions
│ ├── Thermal
│ │ └── Conductive keratoplasty (CK)
│ └── Additive
│ └── Intracorneal inlays
└── INTRAOCULAR PROCEDURES
├── Phakic IOL (natural lens retained)
│ ├── Iris-clip (Artisan/Verisyse)
│ └── Posterior chamber phakic IOL (ICL/EVO-ICL)
└── Clear lens exchange (CLE/RLE)
└── Standard / Multifocal / Toric / EDOF IOL
A. LASER CORNEAL PROCEDURES
The Excimer Laser
- Emits ultraviolet light at 193 nm wavelength
- Can ablate corneal tissue to a precise depth with negligible disruption of surrounding tissue (photoablative decomposition)
- Removes ~0.25 µm of stroma per pulse
- Myopia: central ablation → flattens cornea → reduces refractive power
- Hypermetropia: mid-peripheral ablation → central zone becomes relatively steeper
- Astigmatism: elliptical/toric ablation pattern
1. Surface Ablation Procedures
PRK (Photorefractive Keratectomy)
- Epithelium manually removed (mechanical, alcohol, or laser) → excimer laser applied directly to Bowman's layer / anterior stroma
- No flap created
- Epithelium regenerates over 3-5 days (protective soft contact lens worn)
LASEK (Laser Epithelial Keratomileusis)
- Dilute alcohol (20%) loosens epithelial attachments → epithelium reflected as a sheet (not discarded) → excimer ablation → epithelial flap replaced
- Epithelial flap acts as a biological bandage
TransPRK (Transepithelial PRK / TPRK)
- Single-step: laser removes the epithelium AND ablates the stroma in one pass
- No mechanical contact with cornea
Range of Correction
- Myopia: up to -6 D (less than LASIK)
- Hypermetropia: up to +4 D (less reliable)
- Astigmatism: up to 3 D
Advantages over LASIK
- No flap → no flap-related complications
- Better for patients with thin corneas or those at risk of trauma (martial arts, contact sports)
- Less risk of ectasia
Disadvantages vs LASIK
- Slower visual recovery (days to weeks)
- More postoperative pain and discomfort
- Longer stabilisation of refraction
- Subepithelial haze - managed with MMC (mitomycin C) application to reduce scarring
2. LASIK (Laser In Situ Keratomileusis)
The most widely performed refractive procedure worldwide.
Principle
- A thin superficial corneal flap is created → reflected → excimer laser ablates the stromal bed → flap repositioned
- Flap acts as a natural bandage; heals rapidly
Flap Creation
- Microkeratome (mechanical oscillating blade): creates flap of variable thickness (~130-160 µm); risk of buttonhole or free flap
- Femtosecond laser (preferred): creates a precise, uniform flap of 100-120 µm; more predictable, safer; reduced risk of complications
Range of Correction
| Refractive Error | Maximum (LASIK) |
|---|---|
| Myopia | -6 to -8 D (depends on corneal thickness) |
| Hypermetropia | up to +3-4 D |
| Astigmatism | up to 5 D |
- Critical safety rule: residual corneal stromal bed must be ≥250 µm after ablation to prevent ectasia
LASIK Variants
- Wavefront-guided LASIK: ablation pattern based on wavefront aberrometry measurements; corrects higher-order aberrations (HOAs) for better quality of vision
- 'Optimised' LASIK: proprietary algorithms to produce larger optical zones and reduce induced HOAs
- Topography-guided LASIK: useful for irregular astigmatism
Advantages over Surface Ablation
- Greater postoperative comfort
- Faster visual rehabilitation (clear vision within 24-48 hours)
- More rapid stabilisation of refraction
- Milder stromal haze
LASIK Complications
Intraoperative
| Complication | Comment |
|---|---|
| Buttonhole flap | Blade penetrates through the flap; much rarer with femtosecond laser |
| Incomplete flap | Suction loss during cutting |
| Free flap (no hinge) | Flap completely detached |
| Irregular flap | |
| Penetration into anterior chamber | Rare |
Early Postoperative
- Flap decentration
- Flap wrinkling, distortion or dislocation
- Interface debris
Late Postoperative
| Complication | Details |
|---|---|
| Dry eye | Most common; up to 70% of patients; usually improves spontaneously |
| Transient light sensitivity syndrome | 2-8 weeks post-op; more common after hyperopic LASIK (9%) than myopic (5%) or SMILE (1%); responds to topical steroids |
| Subepithelial haze | Glare, haloes, starbursts especially at night; settles within 3-6 months |
| Epithelial ingrowth | 1-2%; cells grow under the flap; if vision affected → lift flap and scrape |
| Diffuse lamellar keratitis (DLK) | "Sands of the Sahara"; granular deposits at flap interface; 1-7 days post-op; treat with intensive topical antibiotic + steroid |
| Bacterial keratitis | Rare; culture and sensitivity-guided antibiotics |
| Epithelial hyperplasia | Regression; diagnosed with epithelial OCT map |
| Pressure-induced stromal keratitis (PISK) | Fluid cleft in interface due to elevated IOP from prolonged steroids; presents as under-correction/regression |
| Corneal ectasia | Most serious late complication (0.2-0.6%); progressive thinning and bulging of cornea |
Ectasia risk factors: abnormal preoperative topography (keratoconus/FFKC/PMD), low central corneal thickness, low residual stromal bed, high percentage corneal tissue altered, high myopia, young age
3. SMILE (Small Incision Lenticule Extraction)
Principle
- Uses a femtosecond laser (Carl Zeiss VisuMax) exclusively - no excimer laser needed
- Laser cuts a lens-shaped piece of corneal stroma (a lenticule) at two different depths within the intact cornea
- The lenticule is extracted through a small 4 mm arcuate incision - no large flap
- ReLex (Refractive Lenticule Extraction): if removed via a LASIK-style flap instead of the small incision
Results
- Visual outcomes similar to LASIK
Advantages over LASIK
| Advantage | Mechanism |
|---|---|
| Low risk of flap complications | No flap created |
| Biomechanical advantage | Anterior stroma (strongest Bowman's layer fibres) preserved; stronger cornea post-op |
| Faster recovery of dry eye | Less corneal nerve disruption |
| Quicker corneal reinnervation | Smaller incision = less nerve transection |
| Minimal surface disturbance | vs. surface ablation |
Limitation
- Currently approved mainly for myopia and myopic astigmatism (not yet widely available for hyperopia)
B. NON-LASER CORNEAL PROCEDURES
Limbal Relaxing Incisions (LRI) / Arcuate Keratotomy
- Paired arcuate incisions on opposite sides of the cornea in the axis of the steep meridian (the meridian of the correcting plus cylinder)
- Flattening of the steep meridian + mild steepening of the flat meridian → reduces astigmatism
- Effect controlled by: length and depth of incisions + distance from optical centre
- Useful post-keratoplasty where astigmatism can be very high; may be combined with compression sutures in perpendicular meridian
Radial Keratotomy (RK)
- Historical (rarely performed now)
- 8 or more radial incisions from optical zone to limbus → peripheral incisions gape → peripheral cornea flattens → central cornea steepens relatively
- Unpredictable, unstable, diurnal fluctuation of vision
Conductive Keratoplasty (CK)
- Radiofrequency energy applied to corneal stroma in peripheral ring(s) using a micro-needle probe
- Thermal stromal shrinkage → central corneal steepening → treats low-moderate hypermetropia and hypermetropic astigmatism; also used for presbyopia
- Disadvantages: early over-correction, significant regression, induced astigmatism
C. INTRAOCULAR PROCEDURES
Used when refractive error is too high for corneal laser procedures, or cornea is too thin.
1. Phakic IOL (Natural Lens Retained)
Iris-clip IOL ("Lobster Claw" / Artisan / Verisyse)
- Lens attached mechanically to the iris
- Complications: subluxation/dislocation (one/both attachments), oval pupil
Posterior Chamber Phakic IOL (ICL / EVO-ICL - Implantable Collamer Lens)
- Implanted in the posterior chamber between the iris and natural lens
- Excellent optical quality; reversible
- Key complications: cataract (from vaulting issues), raised IOP, endothelial cell loss; newer EVO-ICL has a central port to prevent pupillary block
2. Clear Lens Exchange (CLE / RLE - Refractive Lens Exchange)
- Removal of the clear (non-cataractous) natural lens + IOL implantation
- Provides very good visual results but carries a small risk of cataract surgery complications - particularly retinal detachment in high myopes
- Permanently eliminates accommodation in younger patients
IOL options for CLE:
| IOL Type | Benefit | Side Effect |
|---|---|---|
| Monofocal | Excellent distance (or near) VA | Needs glasses for other distance |
| Bifocal / Trifocal diffractive | Restores near + distance | Nocturnal glare, haloes, reduced contrast sensitivity |
| Extended Depth of Focus (EDOF) | Wider range of clear vision | Reduced contrast sensitivity |
| Toric IOL | Corrects astigmatism | Risk of post-op rotation |
| Multifocal + Toric | Corrects astigmatism + presbyopia | All of the above |
Monovision: one IOL targeted for distance (dominant eye), the other for near. Requires neuro-adaptation and suppression of blur. Effective for presbyopia correction.
D. Summary: Which Procedure for Which Error?
| Refractive Error | 1st Line | 2nd Line (high/thick limits) |
|---|---|---|
| Low-moderate myopia (-1 to -6 D) | LASIK or SMILE | Surface ablation (PRK/LASEK) |
| High myopia (>-8 D) | Phakic IOL (ICL) | Clear lens exchange |
| Low hypermetropia (+1 to +3 D) | LASIK | CK |
| High hypermetropia (>+4 D) | Clear lens exchange | Phakic IOL |
| Astigmatism (up to 3D) | LASIK/PRK | LRI/Toric IOL |
| Astigmatism post-keratoplasty | Arcuate keratotomy + sutures | Toric IOL |
| Presbyopia | Multifocal IOL / monovision | PresbyLASIK / inlays / CK |
| Myopia + thin cornea / keratoconus risk | SMILE or surface ablation | Phakic IOL |
E. Laser Refractive Procedures Comparison Table
| Feature | PRK/LASEK | LASIK | SMILE |
|---|---|---|---|
| Flap | No | Yes | No (small incision) |
| Laser type | Excimer only | Excimer (+ femtosecond for flap) | Femtosecond only |
| Recovery speed | Slow (days-weeks) | Fast (24-48 hrs) | Fast |
| Pain | More | Less | Less |
| Dry eye risk | Less | High (up to 70%) | Lowest |
| Flap complications | None | Yes | None |
| Ectasia risk | Lower | Higher | Lower (Bowman's preserved) |
| HOA induction | More | Less | Similar |
| Stromal haze | Yes (use MMC) | Minimal | Minimal |
| Max myopia | ~-6 D | -6 to -8 D | -10 D (in development) |
| Hyperopia correction | Yes | Yes (+3-4 D) | Not yet routine |
Source: Kanski's Clinical Ophthalmology - A Systematic Approach, 10th Edition, Chapter 8: Corneal and Refractive Surgery
What
This is a shared conversation. Sign in to Orris to start your own chat.