Explain me jaundice from basic to clinics but not in too much detail also add treatment management and symptoms to diagnose
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the essential content needed for a comprehensive yet concise explanation of jaundice from basics to clinics. Let me compose the full answer.
Jaundice: From Basic to Clinical
1. What Is Jaundice?
Jaundice (also called icterus) is a yellow discoloration of the skin, sclera (whites of the eyes), and mucous membranes caused by the accumulation of bilirubin in the blood. It becomes clinically visible when serum bilirubin rises above 2.5-3 mg/dL (normal: 0.3-1.0 mg/dL).
- Schwartz's Principles of Surgery, 11th Ed., p. 1381
- Tietz Textbook of Laboratory Medicine, 7th Ed.
2. Bilirubin Metabolism (The Basics)
Understanding jaundice starts with knowing how bilirubin is made and cleared:
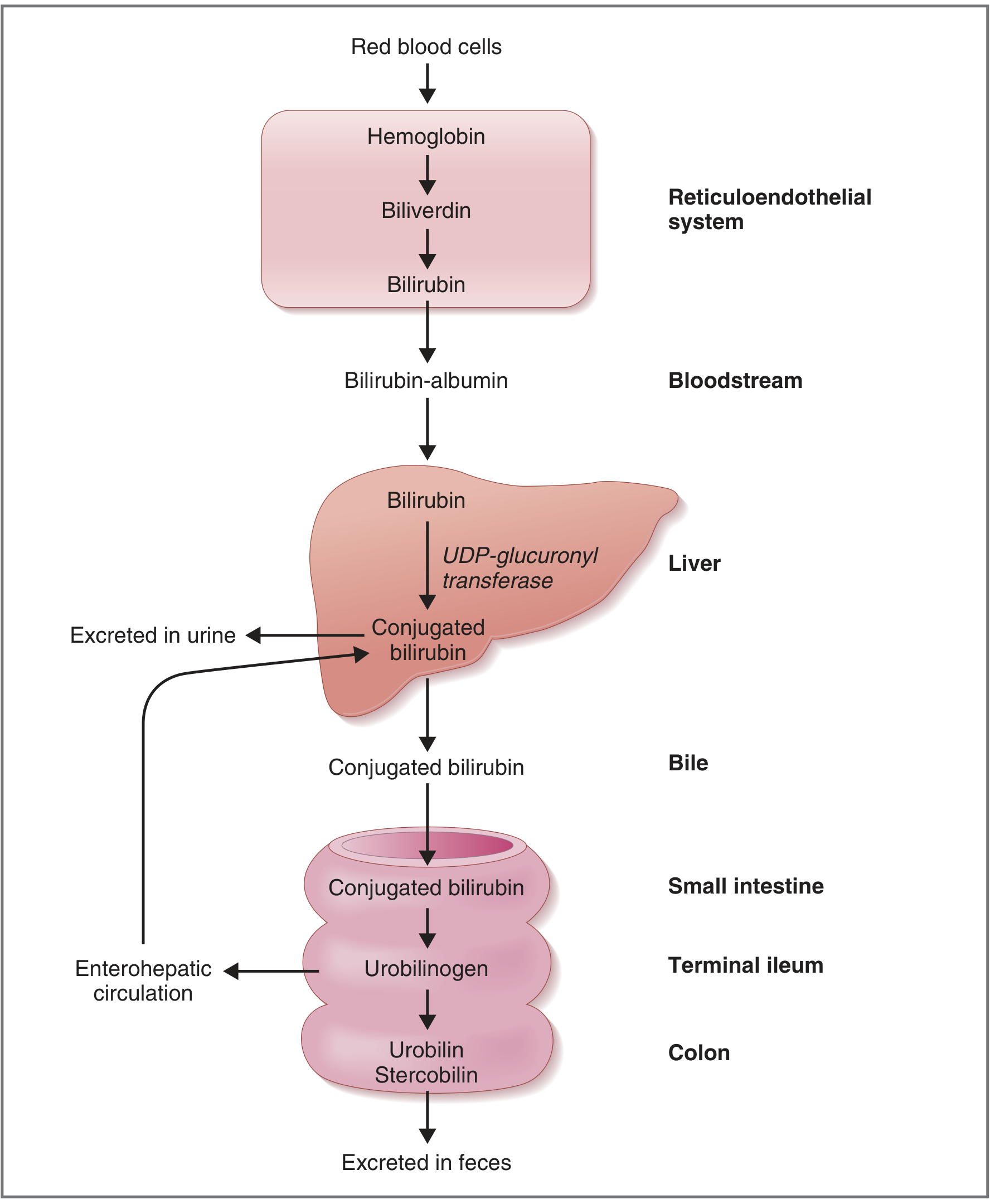
| Step | What Happens |
|---|---|
| 1. Production | Old RBCs are broken down in the reticuloendothelial system (spleen/liver). Hemoglobin → Biliverdin → Unconjugated bilirubin (free, insoluble, bound to albumin in blood) |
| 2. Hepatic uptake | Liver takes up unconjugated bilirubin and via the enzyme UDP-glucuronyltransferase (UDPGT), conjugates it with glucuronic acid → Conjugated bilirubin (water-soluble) |
| 3. Excretion | Conjugated bilirubin is excreted into bile → small intestine → converted by gut bacteria to urobilinogen → some reabsorbed (enterohepatic circulation), some excreted in urine; remainder → stercobilin (gives stool its brown color) |
3. Classification of Jaundice (3 Types)
Jaundice is categorized by where in the bilirubin pathway the problem occurs:
A. Pre-hepatic (Hemolytic) Jaundice
- Problem: Excessive RBC breakdown overwhelms the liver's conjugation capacity
- Type of bilirubin elevated: Unconjugated (indirect)
- Causes:
- Hemolytic anemias (sickle cell disease, thalassemia, G6PD deficiency)
- Malaria
- Transfusion reactions
- Autoimmune hemolysis
- Urine: Normal color (urobilinogen increased, but no bilirubin)
- Stool: Normal/dark
B. Hepatic (Intrahepatic) Jaundice
- Problem: Liver cells (hepatocytes) are damaged and cannot take up, conjugate, or excrete bilirubin properly
- Type of bilirubin: Mixed (both unconjugated and conjugated)
- Causes:
- Viral hepatitis (A, B, C, D, E)
- Alcoholic hepatitis
- Drug-induced liver injury (paracetamol/acetaminophen, isoniazid)
- Cirrhosis
- Autoimmune hepatitis, Wilson's disease
- Genetic disorders:
- Gilbert's syndrome - reduced UDPGT (3-7% of population, mild, benign, triggered by fasting/stress)
- Crigler-Najjar syndrome - absent (type I) or severely reduced (type II) UDPGT; severe neonatal jaundice
- Dubin-Johnson / Rotor syndrome - defective excretion of conjugated bilirubin (benign)
C. Post-hepatic (Obstructive/Cholestatic) Jaundice
- Problem: Bile cannot flow from the liver to the intestine (blocked bile ducts)
- Type of bilirubin: Conjugated (direct)
- Causes:
- Gallstones in common bile duct (choledocholithiasis)
- Pancreatic cancer (head of pancreas - "painless jaundice")
- Cholangiocarcinoma
- Primary sclerosing cholangitis (PSC)
- Primary biliary cholangitis (PBC)
- Strictures, parasites
- Urine: Dark ("tea-colored" - conjugated bilirubin spills into urine)
- Stool: Pale/clay-colored (no stercobilin reaching gut)
- Additional symptom: Pruritus (itching) from bile salt deposition in skin
Schwartz's Principles of Surgery; Harrison's Principles of Internal Medicine 22E (2025)
4. Symptoms & Clinical Diagnosis
Classic Symptoms
| Symptom | Notes |
|---|---|
| Yellow skin/eyes | Most obvious sign; sclera yellows first (sensitive) |
| Dark urine | Suggests conjugated hyperbilirubinemia (hepatic/post-hepatic) |
| Pale stools | Suggests bile duct obstruction |
| Pruritus (itching) | Especially in cholestatic/obstructive jaundice |
| Fatigue, malaise | Common in hepatitis |
| Abdominal pain | Right upper quadrant pain in gallstones/hepatitis; painless in pancreatic cancer |
| Fever, rigors | Suggests cholangitis (bacterial infection of bile ducts - medical emergency) |
| Weight loss | Suggests malignancy |
| Nausea/vomiting | Common with hepatitis |
Key History Points to Elicit
- Alcohol use
- Drug/medication history (including herbal preparations)
- IV drug use, tattoos, sexual history (viral hepatitis risk)
- Travel history
- Family history (hemolytic disorders, Gilbert's)
- Associated pain? (colicky pain = gallstones; painless = cancer until proved otherwise)
- Duration and progression
Physical Examination Clues
| Finding | Suggests |
|---|---|
| Hepatomegaly (tender) | Hepatitis, right heart failure |
| Splenomegaly | Hemolysis, portal hypertension, cirrhosis |
| Ascites | Advanced cirrhosis/portal hypertension |
| Spider angiomata, palmar erythema | Chronic liver disease |
| Courvoisier's sign (palpable, non-tender gallbladder) | Pancreatic/biliary malignancy |
| Kayser-Fleischer rings (eye) | Wilson's disease |
| Cachexia | Malignancy |
5. Investigations (Work-Up)
The diagnostic flowchart from Harrison's is the gold standard approach:
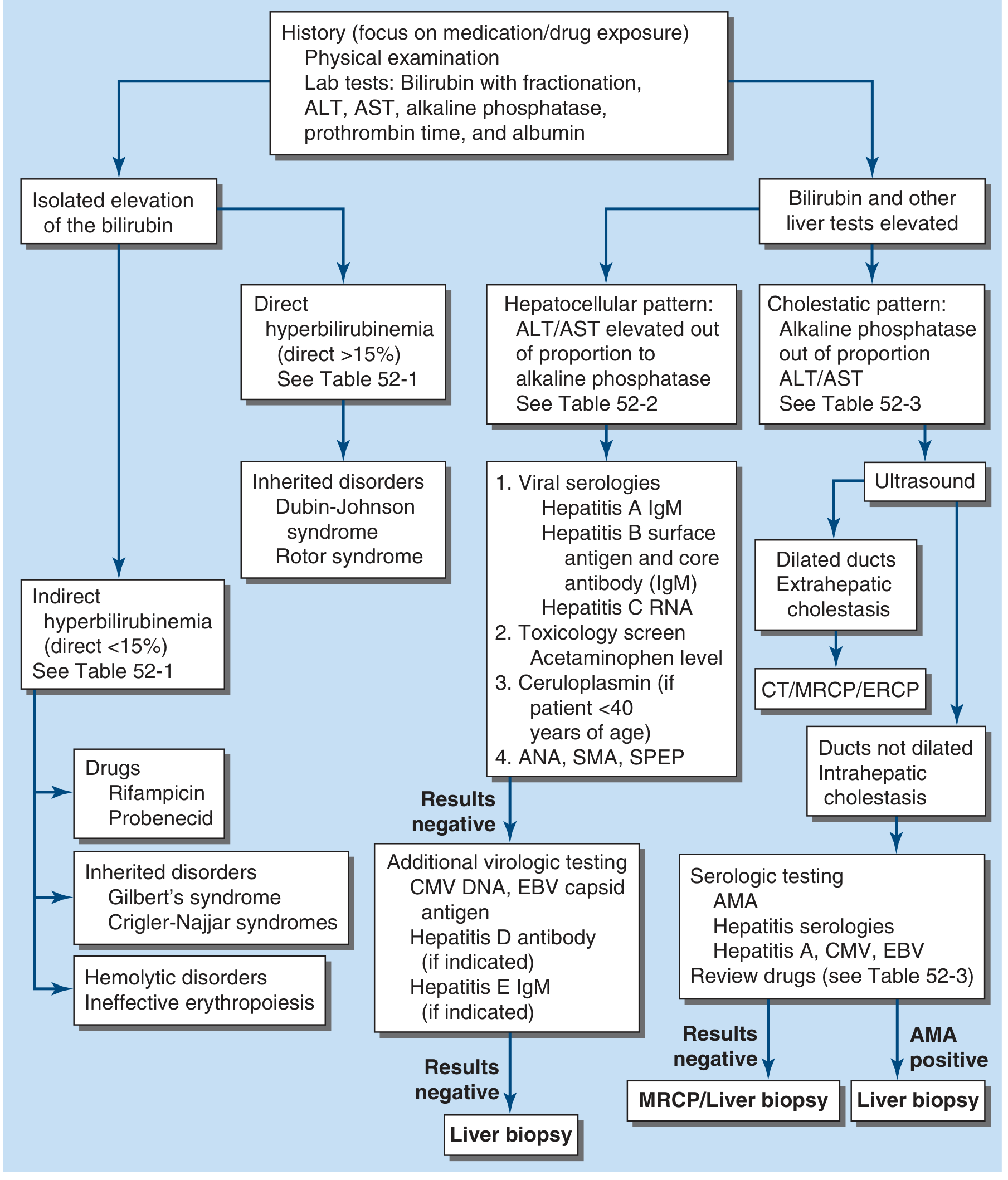
Step-by-Step Lab Approach
Step 1: Bilirubin fractionation
- Predominantly indirect (unconjugated) → pre-hepatic or genetic cause
- Predominantly direct (conjugated) → hepatic or post-hepatic cause
- Direct bilirubin >15% of total → consider Dubin-Johnson/Rotor or obstruction
Step 2: Liver function pattern
| Pattern | What It Suggests | Key Enzymes |
|---|---|---|
| Hepatocellular | ALT/AST elevated out of proportion to ALP | ALT ≥ AST; ALT >500 U/L in viral; AST:ALT ratio ≥2:1 in alcoholic hepatitis |
| Cholestatic | ALP elevated out of proportion to ALT/AST | High ALP, GGT |
| Isolated hyperbilirubinemia | Bilirubin elevated, all else normal | Gilbert's, hemolysis |
Step 3: Additional tests based on pattern
- Hepatocellular: Hepatitis A IgM, HBsAg + core IgM, HCV RNA, CMV/EBV, ceruloplasmin (Wilson's in <40 yr), ANA/SMA (autoimmune hepatitis), toxicology screen
- Cholestatic with dilated ducts on ultrasound: CT/MRCP/ERCP to identify obstruction
- Cholestatic with non-dilated ducts: AMA (anti-mitochondrial antibody - PBC), hepatitis serologies
Imaging:
- Ultrasound - First-line for obstructive jaundice; detects gallstones, dilated bile ducts
- CT scan - Better for pancreatic/periampullary masses
- MRCP - Non-invasive view of biliary tree
- ERCP - Diagnostic + therapeutic (can remove stones, place stents)
- Liver biopsy - When diagnosis remains unclear after imaging/serology
6. Treatment & Management
Treatment depends entirely on the underlying cause:
Pre-hepatic (Hemolytic)
- Treat the underlying hemolytic disorder
- Folic acid supplementation
- Blood transfusions for severe anemia
- In sickle cell: hydroxyurea, exchange transfusion, curative bone marrow transplant
- Gilbert's and Crigler-Najjar Type II: phenobarbital (induces UDPGT enzyme)
- Crigler-Najjar Type I: phototherapy (breaks down bilirubin in skin) + liver transplant is the only cure
Hepatic (Hepatocellular)
| Cause | Management |
|---|---|
| Viral hepatitis A/E | Supportive care (self-limiting) |
| Viral hepatitis B | Antiviral therapy (tenofovir, entecavir) |
| Viral hepatitis C | Directly-acting antivirals (DAAs, e.g., sofosbuvir + ledipasvir) - >95% cure rate |
| Alcoholic hepatitis | Alcohol cessation, corticosteroids (prednisolone) in severe cases, nutritional support |
| Drug-induced | Stop the offending drug; N-acetylcysteine for paracetamol toxicity |
| Autoimmune hepatitis | Corticosteroids + azathioprine |
| Wilson's disease | Penicillamine (copper chelation) or trientine, zinc |
| Acute liver failure | Supportive ICU care; liver transplant evaluation |
Post-hepatic (Obstructive)
| Cause | Management |
|---|---|
| Choledocholithiasis (gallstones) | ERCP with sphincterotomy + stone removal; laparoscopic cholecystectomy |
| Pancreatic cancer | Surgical resection (Whipple procedure) if operable; biliary stent (ERCP) for palliation |
| Cholangiocarcinoma | Surgery, biliary stenting, chemotherapy |
| PSC | Ursodeoxycholic acid, endoscopic dilation of strictures; ultimately liver transplant |
| PBC | Ursodeoxycholic acid (UDCA); obeticholic acid (second-line) |
| Cholangitis (Charcot's triad: fever + RUQ pain + jaundice) | IV antibiotics + urgent ERCP - medical emergency |
Symptomatic Treatment
- Pruritus: Cholestyramine (bile acid sequestrant), antihistamines, rifampicin, naltrexone (opioid antagonist)
- Nutritional support: Fat-soluble vitamin supplementation (A, D, E, K) in chronic cholestasis
- Vitamin K: For coagulopathy due to impaired absorption
- Avoid hepatotoxic drugs, alcohol
7. Special Situations
Neonatal Jaundice
- Physiological in most newborns (days 2-5; immature UDPGT)
- Pathological if appears within 24 hours, persists >2 weeks, or bilirubin is very high
- Risk: Kernicterus (bilirubin crosses blood-brain barrier → brain damage)
- Treatment: Phototherapy (blue light converts bilirubin to water-soluble isomers); exchange transfusion in severe cases
Obstructive Jaundice Quick Summary
"Painless jaundice + weight loss + palpable gallbladder = pancreatic head cancer until proven otherwise" (Courvoisier's law)
Quick Summary Table
| Type | Bilirubin | Urine | Stool | Urobilinogen | Key Enzyme |
|---|---|---|---|---|---|
| Pre-hepatic | ↑ Unconjugated | Normal | Normal/dark | ↑↑ Urine | Normal ALP/ALT |
| Hepatic | ↑ Both | Dark | Pale/normal | Variable | ↑ ALT/AST |
| Post-hepatic | ↑ Conjugated | Dark (tea-colored) | Pale/clay | Absent | ↑ ALP, GGT |
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Schwartz's Principles of Surgery 11th Ed. | Costanzo Physiology 7th Ed. | Tietz Textbook of Laboratory Medicine 7th Ed. | Sleisenger & Fordtran's GI and Liver Disease
Tell me the drug of choice with different different associatted symptoms
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
I now have enough authoritative source material. Let me compile the full drug-of-choice answer organized by symptoms.
Drug of Choice for Jaundice: By Associated Symptom & Cause
The underlying cause of jaundice dictates the drug used. Below is a symptom-by-symptom breakdown with the drug of choice (DOC) for each scenario.
1. Pruritus (Itching) - Most Common Symptom of Cholestatic Jaundice
Affects 20-50% of patients with obstructive/cholestatic jaundice.
| Line | Drug | Dose | Notes |
|---|---|---|---|
| 1st line | Cholestyramine (bile acid sequestrant) | 4-16 g/day | Binds bile acids in gut; must be given 4 hours apart from other drugs |
| 2nd line | Rifampicin | 150-300 mg/day | Induces hepatic enzymes; use with caution - can itself cause hepatitis |
| 3rd line | Naltrexone | Start 12.5 mg → up to 50 mg/day | Opioid antagonist; reverses analgesia if on opioids |
| 4th line | Sertraline | 75-100 mg/day | SSRI; useful if other options fail |
| Special case | Ursodeoxycholic acid (UDCA) | 10-15 mg/kg/day | DOC for pruritus in intrahepatic cholestasis of pregnancy specifically; also first-line for PBC |
| Definitive | Liver transplant | - | End-stage cholestatic disease |
Andrews' Diseases of the Skin; Sleisenger & Fordtran's GI and Liver Disease
2. Jaundice from Viral Hepatitis
Hepatitis A & E (Acute, Self-Limiting)
- DOC: Supportive care - no antivirals needed
- Rest, hydration, avoid alcohol and hepatotoxic drugs
- Vaccination available for prevention (Hep A)
Hepatitis B (Chronic)
| Situation | DOC |
|---|---|
| Active chronic HBV | Tenofovir alafenamide (TAF) or Tenofovir disoproxil fumarate (TDF) |
| Alternative | Entecavir |
| Acute severe HBV | Consider antiviral (tenofovir/entecavir) if fulminant |
Hepatitis C (Chronic)
| Genotype | DOC (Direct-Acting Antiviral) |
|---|---|
| Genotype 1-6 (pan-genotypic) | Sofosbuvir + Velpatasvir (Epclusa) - 12 weeks |
| Genotype 1 | Ledipasvir + Sofosbuvir (Harvoni) - 12 weeks |
| All genotypes | Glecaprevir + Pibrentasvir (Mavyret) - 8 weeks (treatment-naive) |
- Cure rate >95% with modern DAAs
Goodman & Gilman's Pharmacological Basis of Therapeutics; Harrison's 22E
3. Jaundice from Alcoholic Hepatitis
| Symptom/Feature | Drug | Notes |
|---|---|---|
| Severe alcoholic hepatitis (MDF ≥32 or MELD ≥20) | Prednisolone 40 mg/day x 28 days | Reduces short-term mortality; assess response at 7 days (Lille score) |
| If steroids contraindicated | Pentoxifylline (controversial - less used now) | TNF-alpha inhibitor |
| Nutritional support | Thiamine (B1) IV/IM first, then oral | Prevent Wernicke's encephalopathy |
| Encephalopathy | Lactulose + Rifaximin | Reduce ammonia |
| All patients | Alcohol cessation | Mandatory |
4. Jaundice from Biliary Obstruction / Gallstones (Choledocholithiasis)
| Symptom | Drug/Intervention | Notes |
|---|---|---|
| Biliary colic (RUQ pain) | NSAIDs (diclofenac, ketorolac) | DOC for pain; better than opioids for biliary spasm |
| Pain alternative | Opioids (morphine/pethidine) | Second-line if NSAIDs fail |
| Nausea/vomiting | Ondansetron (5-HT3 antagonist) | DOC antiemetic; or metoclopramide |
| Definitive | ERCP + stone removal then laparoscopic cholecystectomy | Not a drug - procedural |
5. Jaundice from Acute Cholangitis (Fever + RUQ Pain + Jaundice = Charcot's Triad)
This is a medical emergency requiring IV antibiotics + biliary drainage.
| Severity | Antibiotic DOC | Notes |
|---|---|---|
| Mild | Piperacillin-tazobactam IV OR Amoxicillin-clavulanate | Broad-spectrum, covers gram-negatives & anaerobes |
| Moderate-Severe | Piperacillin-tazobactam + Metronidazole | Or carbapenem (meropenem) if resistant organisms suspected |
| Septic shock | Meropenem ± Vancomycin | ICU + urgent ERCP |
| Biliary drainage | ERCP (endoscopic decompression) | Mandatory in moderate-severe; life-saving |
Current Surgical Therapy 14e; Tokyo Guidelines 2018
6. Jaundice from Wilson's Disease (Kayser-Fleischer Rings + Neuropsychiatric Symptoms)
| Drug | Mechanism | Notes |
|---|---|---|
| D-Penicillamine | Copper chelation (1st-line historically) | SE: renal, bone marrow suppression, worsens neuro initially |
| Trientine (preferred 1st-line now) | Copper chelation | Better tolerated than penicillamine; DOC in most guidelines |
| Zinc acetate/sulfate | Blocks intestinal copper absorption | Used as maintenance or in pre-symptomatic/pregnant patients |
| Liver transplant | Curative | For acute liver failure or end-stage Wilson's |
Yamada's Textbook of Gastroenterology 7th Ed.
7. Jaundice from Autoimmune Hepatitis (Young women, + ANA/SMA)
| Drug | Notes |
|---|---|
| Prednisolone 40-60 mg/day | Induction - rapid remission |
| Azathioprine 50-100 mg/day | Added after 2 weeks; allows steroid taper (steroid-sparing) |
| Maintenance | Low-dose prednisolone + azathioprine indefinitely |
| Non-responders | Mycophenolate mofetil (MMF) |
8. Jaundice from Primary Biliary Cholangitis - PBC (AMA-positive)
| Drug | Dose | Notes |
|---|---|---|
| Ursodeoxycholic acid (UDCA) | 13-15 mg/kg/day | DOC - slows disease progression |
| Obeticholic acid | 5-10 mg/day | 2nd line if inadequate UDCA response |
| Bezafibrate | 400 mg/day | 3rd line; used in combination |
| Pruritus management | Cholestyramine (see above) |
9. Jaundice from Drug-Induced Liver Injury (DILI)
| Cause | DOC |
|---|---|
| Paracetamol (Acetaminophen) overdose | N-Acetylcysteine (NAC) IV - start ASAP |
| All other DILI | Stop the offending drug |
| Coagulopathy (↓ clotting factors) | Vitamin K IV |
10. Neonatal Jaundice (Physiological / Hemolytic)
| Severity | Treatment |
|---|---|
| Mild-Moderate | Phototherapy (blue light 460-490 nm) |
| Severe | Exchange transfusion |
| Crigler-Najjar Type II | Phenobarbital |
| Rh hemolytic disease | Anti-D immunoglobulin (prevention in mother) + phototherapy/exchange transfusion in neonate |
11. Jaundice from Pancreatic Cancer / Malignant Obstruction
| Symptom | Drug/Intervention |
|---|---|
| Jaundice (palliation) | Biliary stent via ERCP (endoscopic) |
| Pruritus | Cholestyramine / naltrexone |
| Pain | Strong opioids (morphine, oxycodone) + adjuvants |
| Chemotherapy | Gemcitabine + Nab-paclitaxel OR FOLFIRINOX |
Quick Reference Summary Table
| Associated Symptom/Feature | Cause | DOC |
|---|---|---|
| Pruritus (itching) | Cholestasis | Cholestyramine → Rifampicin → Naltrexone |
| Fever + jaundice + RUQ pain | Cholangitis | Pip-tazo IV + urgent ERCP |
| Painless jaundice + weight loss | Pancreatic cancer | ERCP stent (palliation) |
| Jaundice + alcohol history | Alcoholic hepatitis | Prednisolone 40 mg |
| Jaundice + encephalopathy | Liver failure/cirrhosis | Lactulose + Rifaximin |
| Jaundice + Kayser-Fleischer rings | Wilson's disease | Trientine or Penicillamine |
| Jaundice + ANA/SMA positive | Autoimmune hepatitis | Prednisolone + Azathioprine |
| Jaundice + AMA positive | PBC | Ursodeoxycholic acid (UDCA) |
| Jaundice + HBsAg positive | Chronic Hep B | Tenofovir / Entecavir |
| Jaundice + HCV RNA positive | Chronic Hep C | Sofosbuvir-based DAA |
| Jaundice + paracetamol overdose | DILI | N-Acetylcysteine IV |
| Jaundice in newborn | Neonatal | Phototherapy |
| Jaundice + coagulopathy | Liver disease / cholestasis | Vitamin K IV |
| Nausea/vomiting with jaundice | Any cause | Ondansetron (DOC antiemetic) |
| Abdominal pain (biliary colic) | Gallstones | Diclofenac/Ketorolac (NSAIDs) |
Sources: Andrews' Diseases of the Skin | Yamada's Textbook of Gastroenterology 7th Ed. | Current Surgical Therapy 14e | Goodman & Gilman's Pharmacological Basis of Therapeutics | Harrison's Principles of Internal Medicine 22E (2025) | Sleisenger & Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.