hydatid cyst
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hydatid cyst" OR "echinococcosis"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive information to provide a thorough answer. Let me compile it.
Hydatid Cyst (Echinococcosis)
Definition & Causative Agent
A hydatid cyst is the larval stage of Echinococcus granulosus (a small, three-segmented tapeworm) found in the tissues of accidental intermediate hosts, including humans. Three species cause hydatid disease:
- E. granulosus — most common
- E. multilocularis — causes alveolar echinococcosis, more aggressive
- E. ligartus — rare
Epidemiology & Life Cycle
Definitive host: Dogs and other canids (adult tapeworm lives in the ileum, shedding thousands of ova daily in feces).
Natural intermediate host: Sheep (and other grazing animals).
Accidental intermediate host: Humans — an end stage to the parasite; no human-to-human transmission.
Endemic regions: Mediterranean, Middle East, Far East, South America, Australia, New Zealand, East Africa. Particularly associated with sheep-farming communities.
Infection in humans: Ingested ova hatch in the duodenum → oncosphere with hooklets penetrates the mucosa → enters portal bloodstream → settles in the liver (most common) or lungs. Within 3 weeks, a visible cyst develops and grows slowly and spherically (1–7 cm/year).
Cyst Structure
| Layer | Name | Origin | Function |
|---|---|---|---|
| Outer fibrous capsule | Pericyst | Host tissues | Host reaction |
| Outer cyst layer | Ectocyst (gelatinous) | Parasite | Structural |
| Inner cyst layer | Endocyst (germinal) | Parasite | Produces brood capsules |
- Brood capsules — intracystic masses containing developing scoleces (protoscolices)
- Hydatid sand — freed brood capsules + scoleces floating in hydatid fluid
- Daughter cysts — true replicas of the mother cyst, produced endogenously
- Calcification of the wall may occur but does not always mean the cyst is dead
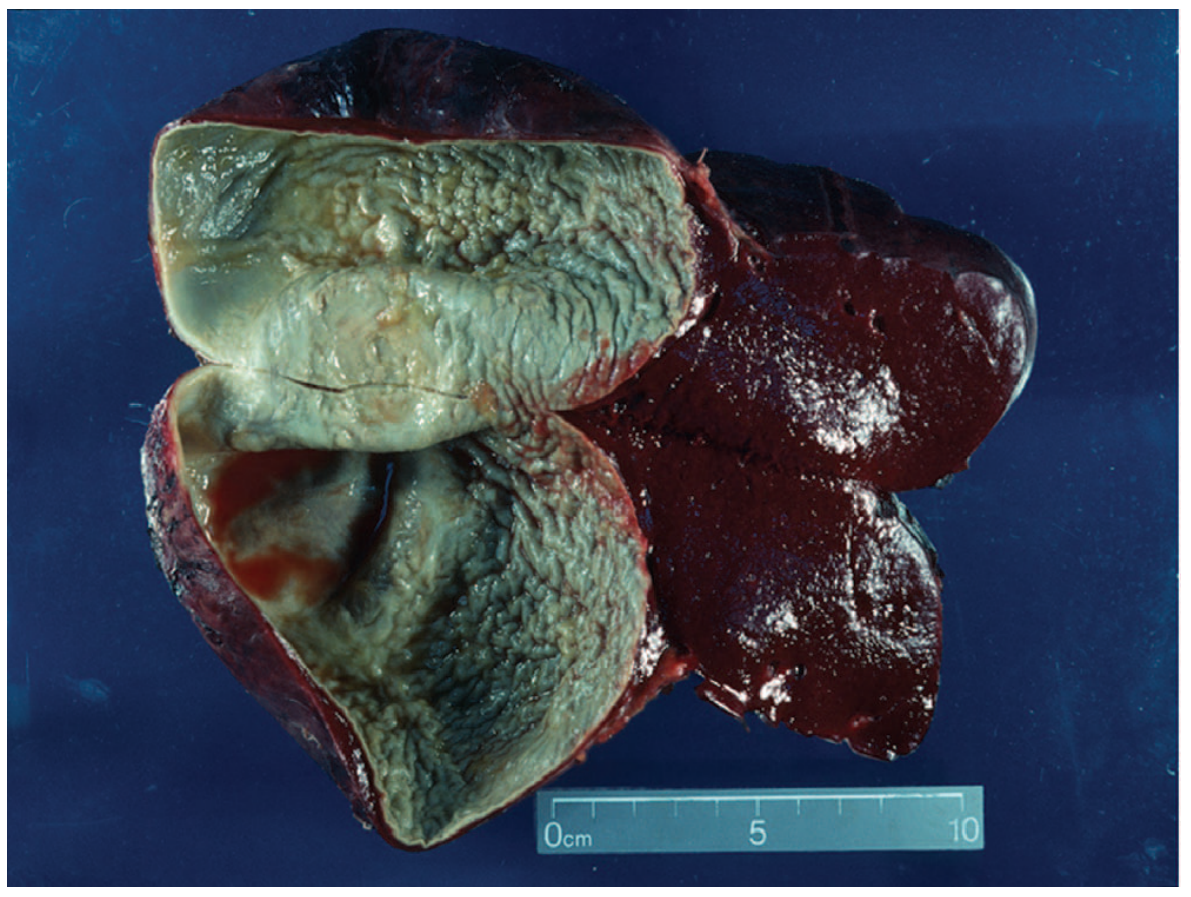
Gross pathology — 14 cm hydatid cyst from a splenectomized patient:
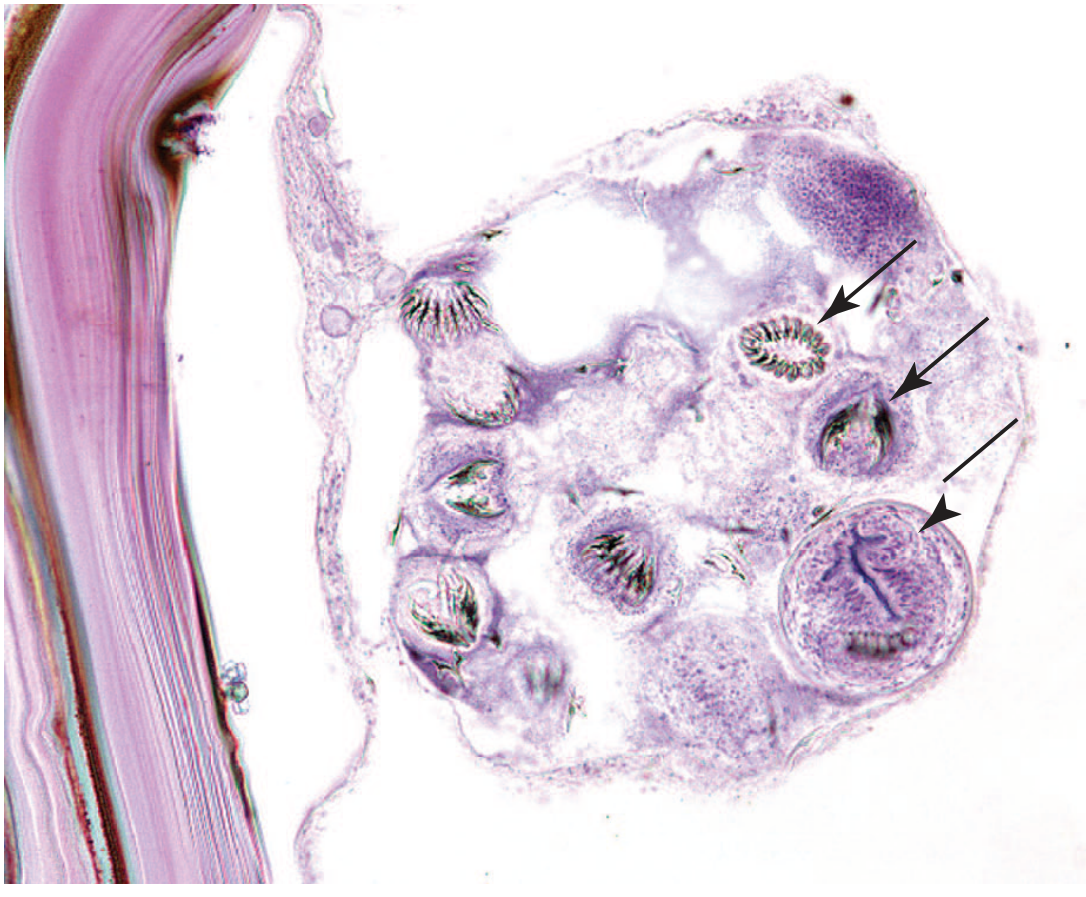
Histology — protoscolices within brood capsules:
Sites of Involvement
| Site | Frequency |
|---|---|
| Liver (right lobe, 75% solitary) | Most common |
| Lungs | 2nd most common |
| Spleen, kidney, pancreas, adrenal | Less common |
| Brain, bone, heart, pericardium | Rare |
Any organ can be involved. Multiple cysts in the same patient are possible.
CT showing large hydatid cyst of the right adrenal gland:
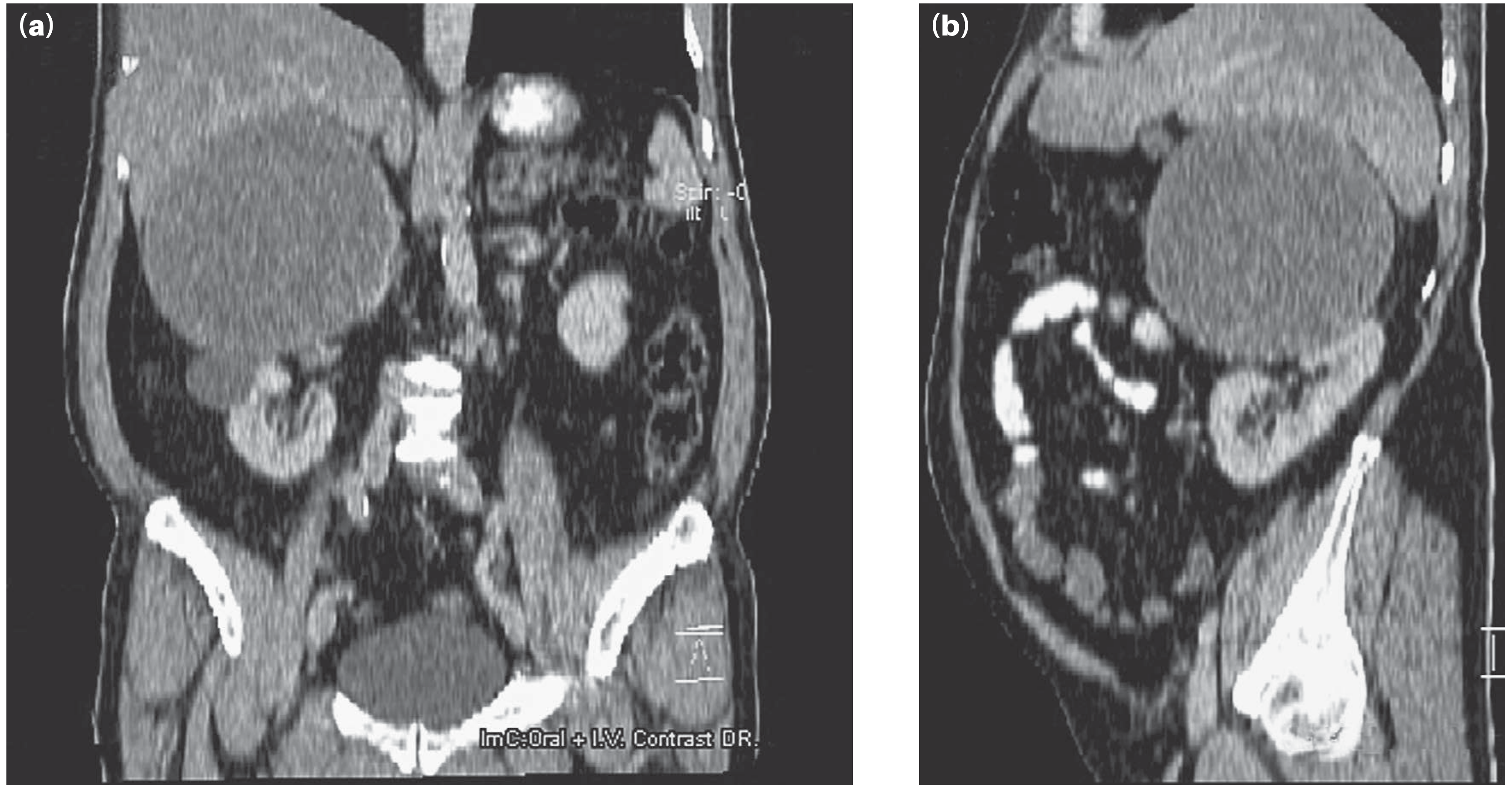
CT showing disseminated abdominal hydatid cysts:

Clinical Features
- Usually asymptomatic until complications occur or incidental discovery
- Right upper quadrant mass + hepatomegaly (most common presentation)
- Abdominal pain, dyspepsia, vomiting
- Jaundice (~8%) — biliary tree involvement
- Fever (~8%) — bacterial superinfection (mimics pyogenic abscess)
- Anaphylactic shock — rupture of cyst (life-threatening emergency)
- Dyspnoea — pulmonary cysts
- Raised ICP / headaches — cerebral cysts (rare, but must be suspected in sheep-farming communities)
Complications of Rupture
- Into biliary tree → obstructive jaundice, biliary colic, cholangitis
- Into bronchial tree → patient coughs up white material (scoleces)
- Into peritoneal/pleural/pericardial cavities → disseminated echinococcosis or fatal anaphylaxis
- Bacterial superinfection → pyogenic abscess picture
Diagnosis
Bloods
- Eosinophilia (raised eosinophil count)
- Serology: ELISA, immunoelectrophoresis — raise suspicion but plagued by low sensitivity and specificity
- LFTs abnormal if biliary involvement
Imaging (investigation of choice)
Ultrasound — most widely used (available, affordable, accurate). The WHO-IWGE classification (CE stages) is based on ultrasound:
| Stage | Finding |
|---|---|
| CL | Unilocular anechoic lesion, no internal echoes |
| CE1 | Anechoic cyst with "hydatid sand" (fine internal echoes) |
| CE2 | Multivesicular with daughter cysts; honeycomb/rosette appearance |
| CE3a | Detached laminated membrane ("water-lily" sign) |
| CE3b | Daughter cysts inside solid matrix |
| CE4 | Degenerative — no daughter cysts visible; "bag of wool" appearance |
| CE5 | Partial or complete wall calcification |
CT / MRI — better for extrahepatic disease, anatomical relationships, and surgical planning. CT: smooth space-occupying lesion with septa; calcification highly suggestive.
MRCP / ERCP — when biliary communication is suspected (multiple cysts communicating with bile ducts causing biliary obstruction and dilatation).
WHO Clinical Groups (for management decisions)
| Group | Activity |
|---|---|
| Group 1 (Active) | Cysts >2 cm, often fertile |
| Group 2 (Transitional) | Degenerating due to host resistance or treatment; may contain viable protoscolices |
| Group 3 (Inactive) | Degenerated, partially or totally calcified; unlikely to be viable |
Treatment
Management depends on group, number of cysts, anatomical location, and patient fitness. Best done in a tertiary unit with hepatobiliary surgery, hepatology, and interventional radiology.
1. Medical Therapy
- Albendazole — primary drug; used pre- and post-procedure to reduce recurrence
- Praziquantel — also used (both may be available on a "named patient" basis in some countries)
2. PAIR (minimally invasive)
Puncture → Aspiration → Injection (scolicidal agent) → Re-aspiration
Done under US/CT guidance after pre-treatment with albendazole.
3. Surgical Options
- Radical total pericystectomy with omentoplasty
- Partial pericystectomy
- Hepatic segmentectomy (for peripheral lesions)
- Laparoscopic approaches are increasingly used
Scolicidal agents used intraoperatively:
- Hypertonic saline (15–20%)
- Ethanol (75–95%)
- 5% povidone-iodine (10% also used)
⚠️ Scolicidal agents can cause sclerosing cholangitis if biliary radicals communicate with the cyst wall.
4. Watch and Wait
Asymptomatic, inactive (Group 3/CE4-5) cysts may be left alone with surveillance.
Key Dangers
- Rupture + anaphylaxis — medical emergency; potentially fatal
- Daughter cyst dissemination — if cyst ruptures, brood capsules can metastasize and form multiple new cysts throughout the body
- Incomplete surgery without scolicidal agents can lead to recurrence and dissemination
Sources: Sabiston Textbook of Surgery; Bailey and Love's Short Practice of Surgery, 28th ed.; Jawetz, Melnick & Adelberg's Medical Microbiology, 28th ed.
This is a shared conversation. Sign in to Orris to start your own chat.