Retinoschisis
Reading File
Finding Sources
Finding Sources
Searching PubMed
retinoschisis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of Retinoschisis — a splitting of the neurosensory retina — which exists in two distinct forms.
Retinoschisis
Retinoschisis is defined as a splitting (schisis) of the neurosensory retina (NSR) into inner and outer layers. It occurs in two fundamentally different forms: X-linked (juvenile) and age-related (degenerative).
1. X-Linked (Juvenile) Retinoschisis
Genetics & Pathophysiology
- Rare, X-linked recessive condition caused by mutations in the RS1 gene (Xp22.13), which encodes retinoschisin — a protein secreted by photoreceptors involved in intercellular adhesion
- The basic defect involves splitting of the retinal nerve fibre layer (NFL) from the rest of the sensory retina (though recent evidence shows outer plexiform layer separation is also frequent)
- Males are affected; female carriers are asymptomatic with no retinal changes
Clinical Features
Symptoms:
- Typically presents in boys aged 5–10 years with difficulty reading / reduced vision
- Less commonly: squint or nystagmus in infancy (associated with advanced peripheral retinoschisis + vitreous haemorrhage)
Signs:
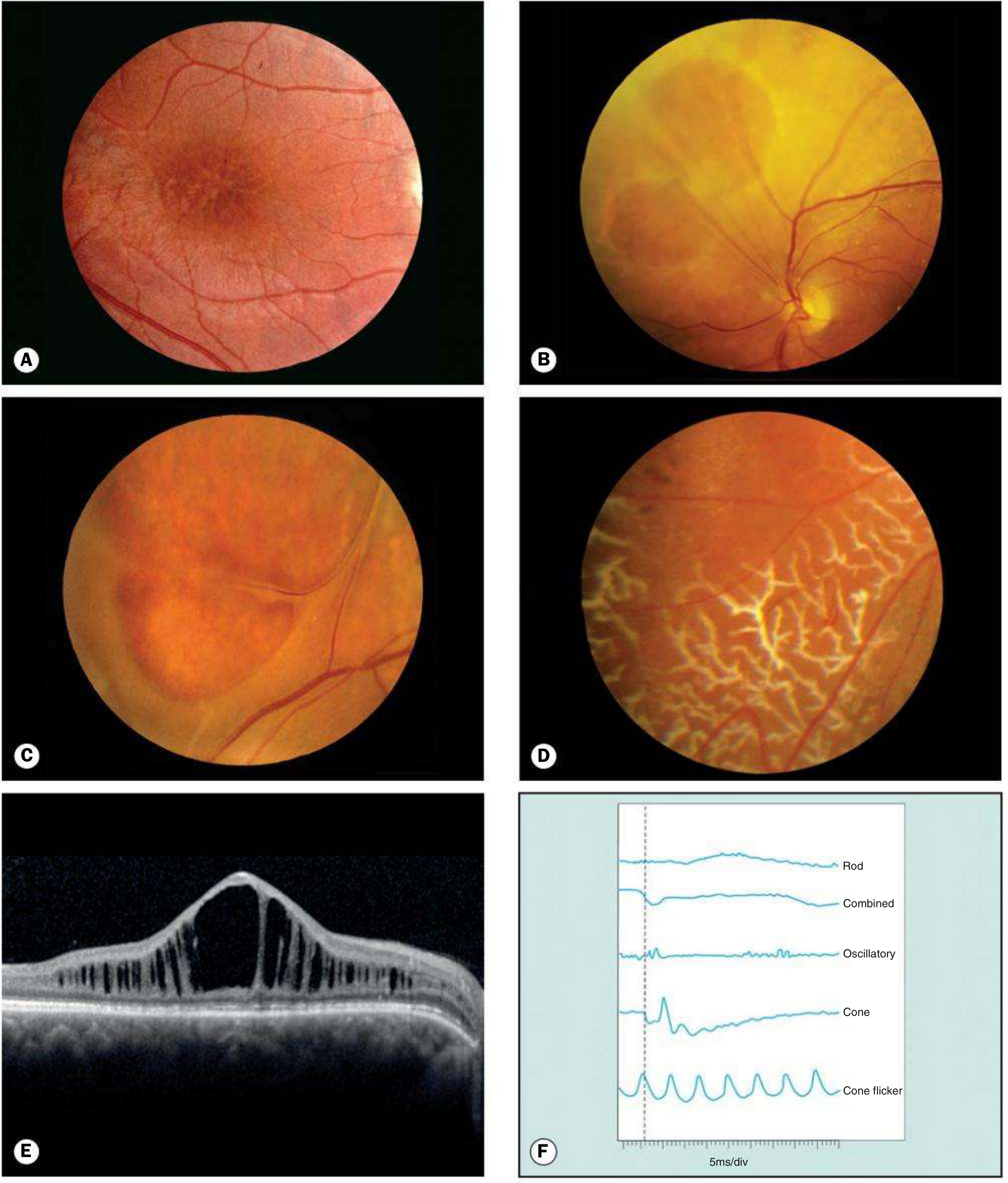
- Macular (foveal) schisis — the hallmark: spoke-like ("bicycle wheel" / petaloid) striae radiating from the foveola with underlying cystoid changes; the most common appearance
- Peripheral schisis (in ~50%): predominantly inferotemporal; inner layer (ILM + NFL only) can develop oval defects, and in extreme cases vessels float as "vitreous veils"
- Silvery peripheral dendritic figures, vascular sheathing, pigmentary changes, retinal flecks, nasal dragging of retinal vessels
- Drusen-like dots at the macula
Complications:
- Vitreous / intra-schisis haemorrhage
- Neovascularization
- Subretinal exudation
- Rhegmatogenous or tractional retinal detachment (uncommon)
- Visual acuity deteriorates during the first two decades, may then stabilize until the 5th–6th decade
Investigations
| Test | Finding |
|---|---|
| OCT | Cystic spaces in inner nuclear + outer plexiform layers; foveal disorganization |
| ERG | Characteristic electronegative ERG (selective ↓ b-wave amplitude with preserved a-wave) — occurs in eyes with peripheral schisis |
| IVFA | No leakage (unlike CMO) |
| FAF | Variable macular abnormality; spoke-like pattern; central hypoautofluorescence with surrounding hyperautofluorescence |
| Genetic testing | Mutations in RS1 gene |
Treatment
- Topical or oral carbonic anhydrase inhibitors (e.g. dorzolamide TDS, acetazolamide) — reduce foveal schisis and may improve visual acuity in some patients
- Vitrectomy for non-clearing vitreous haemorrhage or retinal detachment (technically challenging)
- Patching for superimposed amblyopia in children < 11 years
- Gene therapy under investigation (aiming to restore retinoschisin function)
- Follow-up: every 6 months (more frequently if treating amblyopia)
2. Age-Related (Degenerative) Retinoschisis
Epidemiology & Pathology
- Present in ~5% of the population over age 20; particularly prevalent in hypermetropes
- Develops from coalescence of microcystoid degeneration → splitting of NSR into inner and outer layers with permanent loss of visual function in the affected area
- Typical form: split at the outer plexiform layer (most common)
- Reticular form: split at the nerve fibre layer — rarer, more prone to complications
Clinical Features
Symptoms:
- Usually asymptomatic (photopsia and floaters absent — no vitreoretinal traction)
- Occasionally: decreased vision, vitreous haemorrhage, or progressive RD
Signs:
- Bilateral in up to 80%
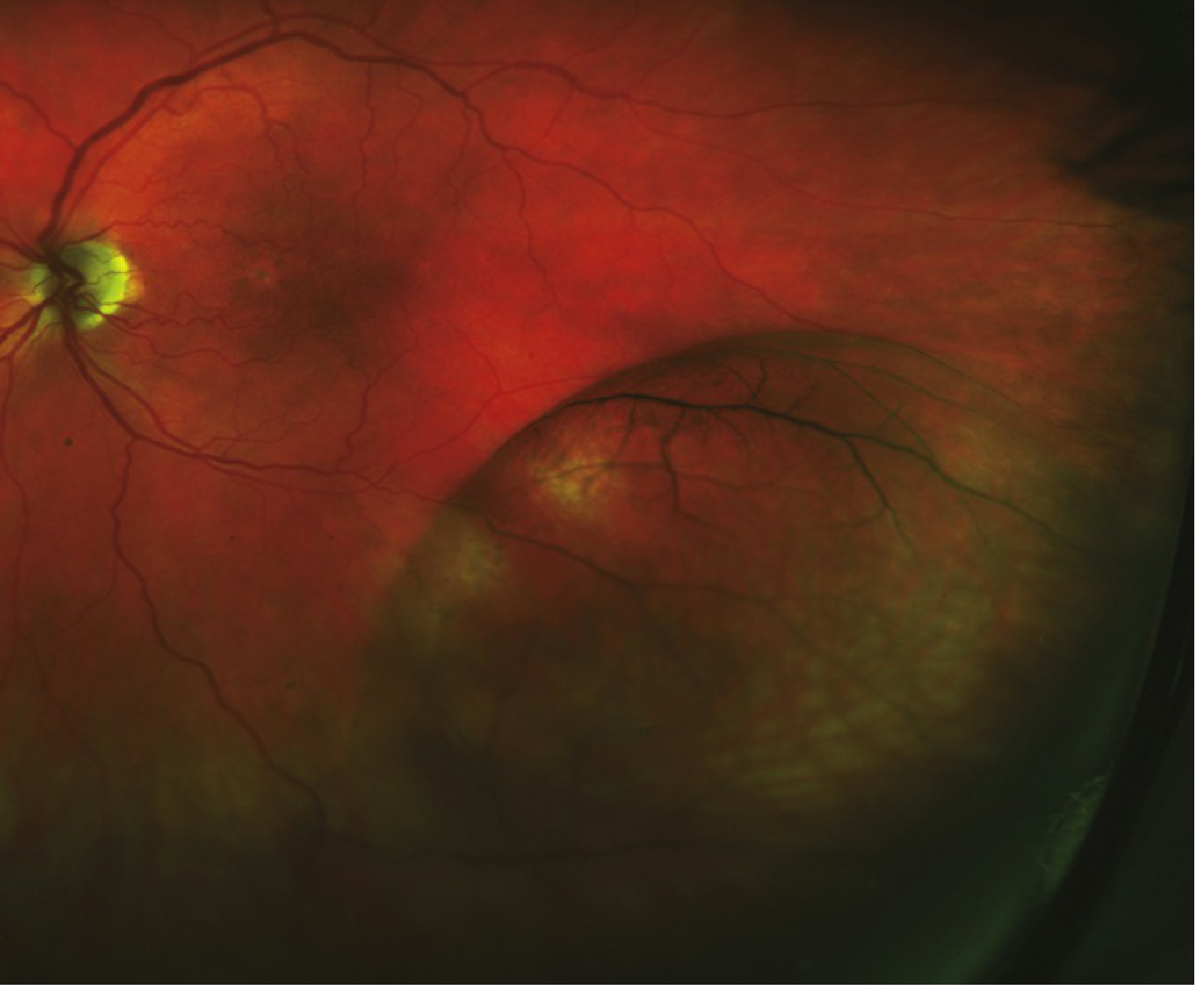
- Smooth, dome-shaped, convex, relatively immobile elevation — typically inferotemporally
- Inner leaf surface may show "snowflakes" (whitish Müller cell footplate remnants) and vascular sclerosis
- Bridging grey-white tissue strands across the schisis cavity
- Prominent cystoid degeneration near the ora serrata
- Inner leaf breaks: small and round
- Outer leaf breaks: larger, rolled edges, behind the equator — higher risk of RD
- Absolute scotoma corresponding to the schisis area (cf. relative scotoma in RRD)
- No pigment cells or haemorrhage in vitreous; no demarcation line (unless associated RD)
Complications:
- RD is rare (~1% even with breaks in both layers); usually asymptomatic and rarely progressive
- Posterior extension to involve fovea — very rare
Investigations
| Test | Finding |
|---|---|
| Slit lamp | No anterior chamber inflammation; no vitreous pigment |
| OCT | Confirms layer of retinal splitting; helps distinguish from RD |
| Visual fields | Absolute scotoma (vs. relative in RD) |
| Scleral depression | Rules out outer layer breaks and concomitant RD |
Treatment
- Usually observation — discuss RD symptoms with all patients; return if floaters, flashing lights, or visual curtain appear
- Surgery only when a clinically significant RD develops
- A small RD walled off by a demarcation line is typically not treated
- Follow-up: every 6 months
Key Differentiating Features
| Feature | X-linked Juvenile RS | Age-related Degenerative RS | RRD (for comparison) |
|---|---|---|---|
| Age | Boys 5–10 yrs | Adults >20 yrs | Any |
| Genetics | RS1 mutation (X-linked) | Acquired / sporadic | — |
| Laterality | Bilateral | Bilateral (80%) | Usually unilateral |
| Location | Macular + inferotemporal periphery | Inferotemporal periphery | Variable |
| Splitting level | NFL (and outer plexiform) | Outer plexiform layer | Sub-retinal space |
| Surface | Smooth | Smooth, immobile | Corrugated, mobile |
| Vitreous | VH may occur | Clear — no pigment cells | Pigmented cells (Shafer's) |
| Scotoma | Absolute | Absolute | Relative |
| IVFA | No leakage | — | Leakage possible |
| ERG | Electronegative (↓ b-wave) | Normal | — |
| Demarcation line | May be present (even without RD) | Absent (unless associated RD) | Present (old RD) |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 670–671, 685–686 | Wills Eye Manual, pp. 772–776
Recent evidence note (PMID 41760155): A 2026 umbrella systematic review on inherited retinal diseases (including X-linked RS) highlights gene therapy as an emerging approach — consistent with the textbook note that RS1 gene replacement therapy is under active investigation.
B scan
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
B-Scan Ultrasonography (Ophthalmic)
Principle
B-scan (brightness-modulated scan) uses high-frequency sound waves that produce echoes at interfaces between acoustically distinct structures. It provides real-time, two-dimensional (cross-sectional) images of the eye, spanning from the posterior aspect of the cornea to the posterior wall of the globe.
Probe Placement
The probe can be applied:
- Directly on the globe (topical anaesthetic applied) — preferred for locating specific pathology (e.g. retinal tear, tumour)
- Over the closed eyelid with sterile methylcellulose coupling gel — preferred in trauma or poorly cooperative patients (avoids pressure on the globe)
A coupling agent (methylcellulose or ophthalmic gel) is always used at the probe tip.
Technique
| Scan Type | Probe Marker Orientation |
|---|---|
| Vertical scan | Marker pointing superiorly (towards brow) |
| Horizontal scan | Marker pointing nasally (towards nose) |
- The eye is examined with the patient looking straight ahead, up, down, left, right
- The probe moves in the opposite direction to gaze — e.g., patient looks left → probe moves nasally to scan the nasal fundus
- Dynamic scanning: patient moves the eye while the probe is held still — critical for assessing membrane mobility
Gain:
- High gain → amplifies weak echoes (e.g., vitreous opacities, subtle haemorrhage)
- Low gain → shows only strong echoes (retina, sclera); improves resolution
Clinical Uses in Ophthalmology
| Indication | What B-Scan Shows |
|---|---|
| Opaque media (dense VH, mature cataract, corneal opacity, hyphema) | Evaluate posterior segment when not directly visible |
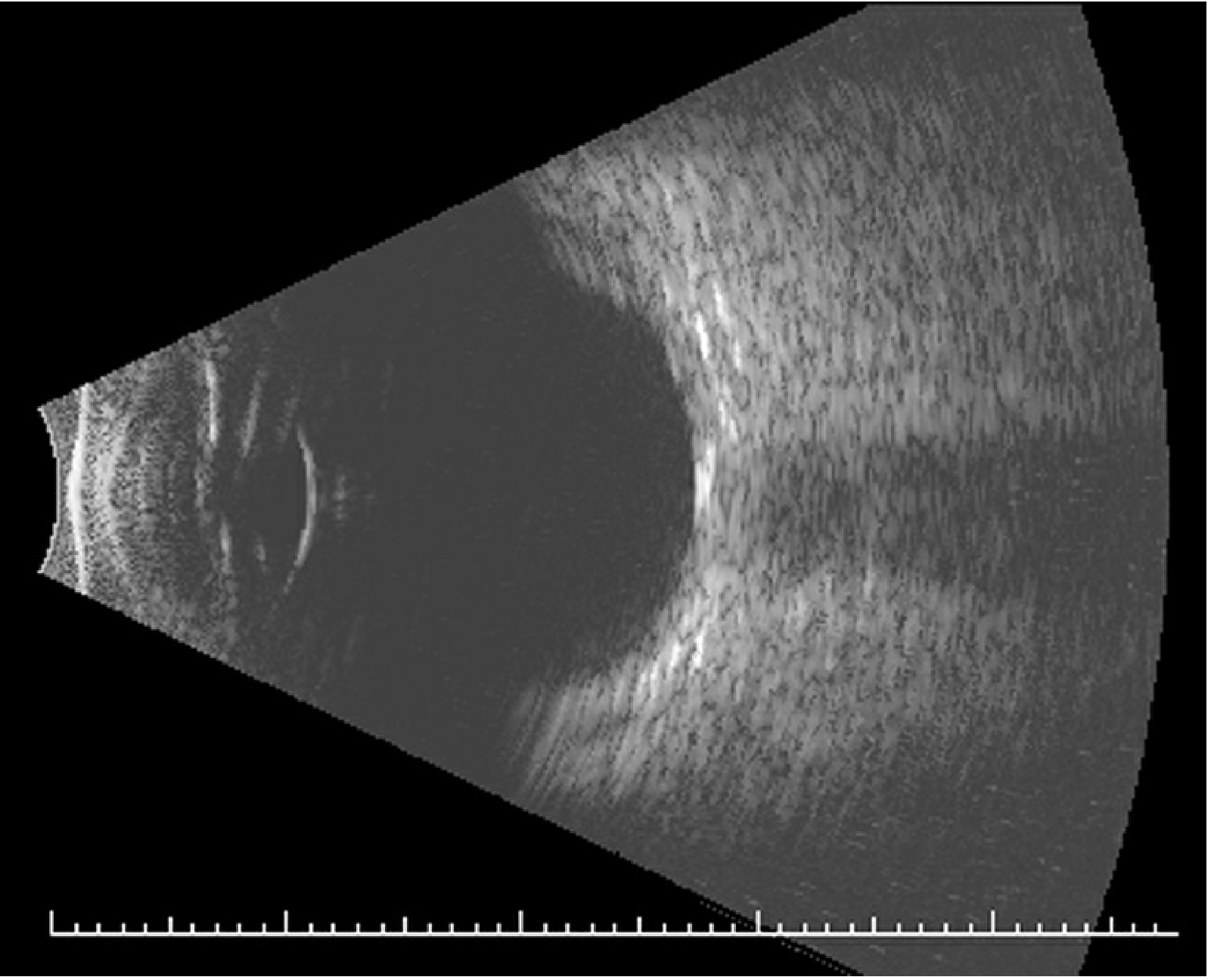
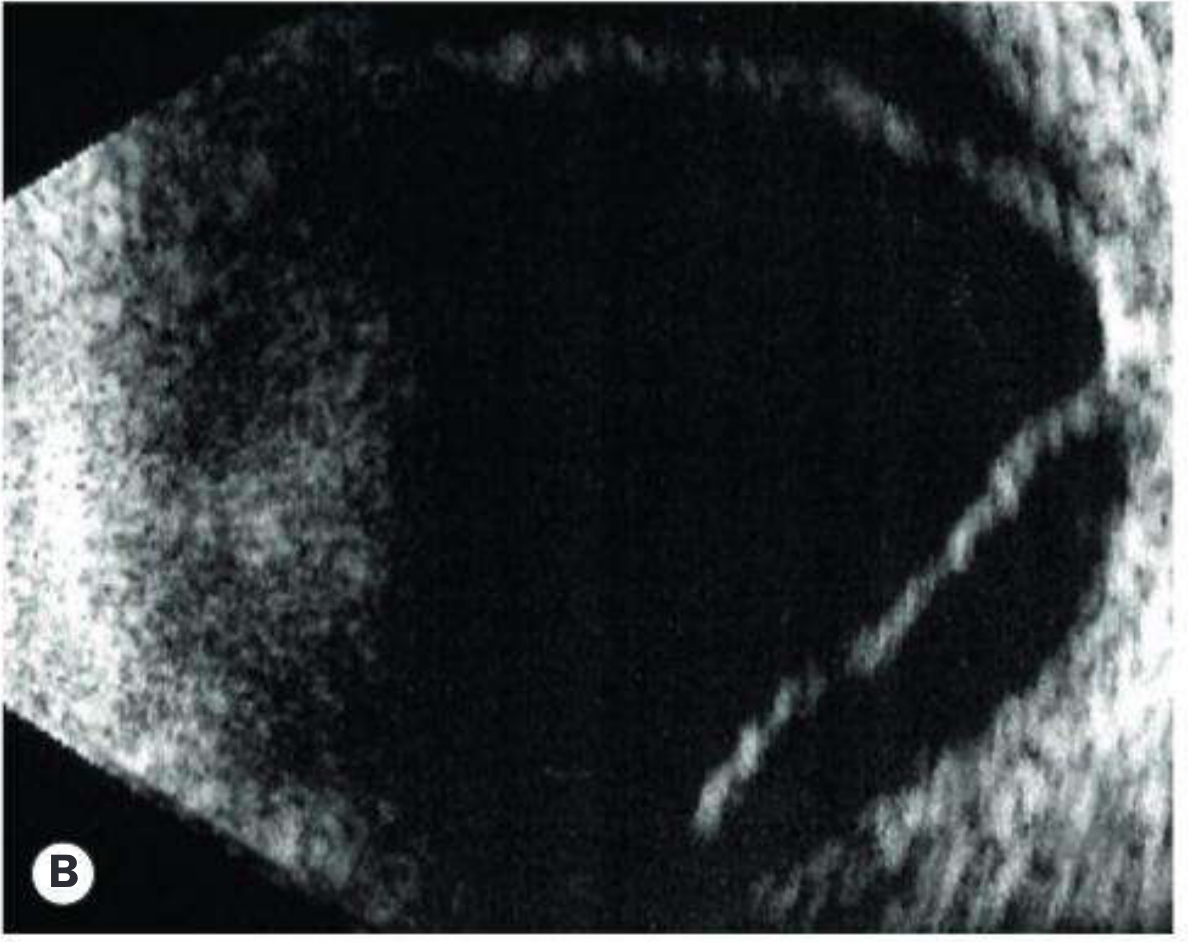
| Retinal detachment | Highly reflective, mobile membrane; "good mobility" on dynamic scan; SRF extends to ora serrata |
| Retinoschisis vs. RD | Schisis cavity: smooth, immobile, no mobility on dynamic scan; RD: mobile, corrugated |
| PVD | Incomplete PVD: relatively immobile membrane; complete PVD: highly mobile |
| Vitreous haemorrhage | Non-clotted: uniform appearance; clotted: small particulate echoes |
| Choroidal detachment | Differentiate serous vs. haemorrhagic; peripheral dome-shaped elevations that "kiss" anteriorly |
| Posterior scleritis | Scleral thickening + fluid in sub-Tenon space → characteristic "T-sign" |
| Intraocular tumour | Assess consistency, size, vascularity (e.g. choroidal melanoma — low internal reflectivity; retinoblastoma — calcification echoes) |
| Intraocular foreign body | Metallic/glass → strong echo with shadow; wood variable |
| Optic disc abnormalities | Optic disc drusen (buried), coloboma |
| Scleral rupture | Posterior to muscle insertions or when media opacities prevent direct view |
B-Scan Findings in Specific Conditions
Retinal Detachment (RRD)
- High-reflectivity membrane with good mobility of retina and vitreous on dynamic scan
- Subretinal fluid (SRF) extending to the ora serrata
- Membrane tethered at optic disc
Retinoschisis vs. RD
| Feature | Retinoschisis | RRD |
|---|---|---|
| Surface | Smooth, convex | Corrugated |
| Mobility (dynamic scan) | Immobile | Mobile |
| Extent | Usually anterior to equator | Can extend to posterior pole |
| After-movement | Absent | Present |
| Scotoma type | Absolute | Relative |
Vitreous Haemorrhage
- Non-clotted: uniform, low-level echoes filling vitreous cavity
- Clotted/organising: particulate echoes; may show strand formation
- Critical use: to exclude underlying RD or choroidal melanoma behind a dense haemorrhage — always perform B-scan in dense VH
Posterior Scleritis
- Scleral thickening with fluid in the sub-Tenon space posterior to the globe → "T-sign" (the fluid creates a perpendicular dark line alongside the optic nerve shadow)
Choroidal Detachment
- Serous: smooth, dome-shaped elevations, low internal reflectivity
- Haemorrhagic: higher internal reflectivity, less mobile, may "kiss" (touch each other) anteriorly
Limitations / Pitfalls
- Dense intraocular calcifications (e.g. phthisis bulbi) → poor image quality
- Silicone oil or intraocular gas → distorts image; scan the patient upright to improve quality
- Known ruptured globe → relative contraindication to direct probe placement on globe; use over closed lid with copious gel and no pressure
- Anterior orbit / retrobulbar structures → B-scan has limited anterior orbital penetration; CT/MRI preferred for deeper orbital pathology
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 683–684 | Wills Eye Manual, pp. 1093–1095
This is a shared conversation. Sign in to Orris to start your own chat.