Explain me 10 cardiac heart disease with ecg changes and explain it
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
ECG changes myocardial infarction STEMI ST elevation leads
Searching Images
atrial fibrillation ECG irregularly irregular no P waves
Searching Images
acute pericarditis ECG diffuse ST elevation PR depression four stages
Searching Images
complete heart block third degree AV block ECG P wave dissociation
Searching Images
hypertrophic cardiomyopathy ECG LVH deep Q waves voltage criteria
Searching Images
pulmonary embolism ECG S1Q3T3 right axis deviation sinus tachycardia
Searching Images
left ventricular hypertrophy LVH ECG voltage criteria Sokolow strain pattern
Searching Images
Wolff-Parkinson-White WPW syndrome ECG delta wave short PR interval
Searching Images
long QT syndrome QTc prolongation torsades de pointes ECG
I now have comprehensive material from the textbooks and image library. Let me compile the full answer.
10 Cardiac Heart Diseases with ECG Changes
1. ST-Elevation Myocardial Infarction (STEMI)
Disease overview: STEMI results from complete occlusion of a coronary artery causing transmural (full-thickness) myocardial infarction. The affected myocytes suffer ischemia, injury, and ultimately necrosis in sequence.
ECG Evolution (classic 4-stage sequence):
| Stage | ECG Finding | Timeframe |
|---|---|---|
| Hyperacute | Tall, peaked "hyperacute" T-waves | Minutes |
| Acute injury | ST-segment elevation (convex/tombstone) | Hours |
| Evolving infarction | T-wave inversion, Q-wave formation | Hours–days |
| Old infarction | Pathological Q waves persist | Weeks–permanent |
Lead localisation of STEMI:
| Territory | ST Elevation Leads | Artery |
|---|---|---|
| Anteroseptal | V1, V2, (V3) | Proximal LAD |
| Anterior | V1–V4 | LAD |
| Anterolateral | V1–V6, I, aVL | Proximal LAD |
| Lateral | I, aVL | LCx |
| Inferior | II, III, aVF | RCA |
| Posterior | Tall R in V1–V2, R/S ≥1 | RCA/LCx |
| Right ventricular | II, III, aVF + ST elevation in V3R–V6R | Proximal RCA |
Mechanism of ST elevation: Epicardial myocytes depolarize from ischemic injury, creating a current of injury. The resulting voltage difference between injured and normal cells depresses the rest of the tracing relative to the ST segment — making ST appear elevated. — Medical Physiology (Boron & Boulpaep)
Pathological Q waves develop because the infarcted zone becomes electrically silent; the net depolarisation vector points away from the dead tissue, inscribing a deep negative deflection in overlying leads. — Medical Physiology

(Acute anterolateral STEMI: convex ST elevation V1–V6, I, aVL; reciprocal ST depression II, III, aVF)
2. Non-ST-Elevation Myocardial Infarction (NSTEMI) / Unstable Angina
Disease overview: Partial coronary occlusion causes subendocardial (non-transmural) ischaemia. Biomarkers rise in NSTEMI; they remain normal in unstable angina.
ECG Changes:
- ST-segment depression (horizontal or downsloping) in ischaemic territory
- T-wave inversion — symmetrical, deep ("Wellens' sign" in V1–V3 warns of critical LAD stenosis)
- No pathological Q waves (non-transmural)
- ECG may be normal in 30–50% at presentation
Wellens' syndrome (critical proximal LAD stenosis):
- Type A: Biphasic T waves in V2–V3
- Type B: Deep symmetric T-wave inversions in V2–V3
"The diagnosis of NSTEMI depends on abnormal elevation of cardiac biomarkers but may include ECG changes not meeting criteria for STEMI." — Tintinalli's Emergency Medicine
3. Atrial Fibrillation (AF)
Disease overview: Disorganised, chaotic atrial electrical activity at 350–600 impulses/min; the AV node acts as a filter, allowing irregular ventricular conduction.
ECG Features (classic triad):
- Absent P waves — replaced by fine, irregular fibrillatory (f) waves on the baseline (best seen in V1 and lead II)
- Irregularly irregular R-R intervals — no two consecutive R-R intervals are equal
- Narrow QRS complexes — unless pre-existing bundle branch block or accessory pathway (WPW) causes aberrant conduction
ECG features: "Absence of discernible P waves with flat or chaotic isoelectric baseline; QRS complexes narrow unless preexisting bundle branch block or preexcitation syndrome; irregularly irregular ventricular rhythm." — Tintinalli's Emergency Medicine
4. Acute Pericarditis
Disease overview: Inflammation of the pericardial sac, most commonly viral (Coxsackie B). The electrically silent pericardium produces ECG changes via involvement of the superficial myocardium.
ECG — 4 Classic Stages:
| Stage | ECG Finding |
|---|---|
| Stage 1 | Diffuse concave ("saddle-shaped") ST elevation in nearly all leads except aVR and V1; PR-segment depression in same leads; PR elevation + ST depression in aVR |
| Stage 2 | ST and PR segments normalise |
| Stage 3 | T-wave inversion (with or without ST depression) |
| Stage 4 | Complete normalisation |
Key distinguishing features vs STEMI:
- ST elevation is diffuse (not localised to one coronary territory)
- ST morphology is concave upward (saddle-shaped), not convex
- PR depression present in pericarditis; absent in STEMI
- No reciprocal ST depression except in aVR and V1
- No Q waves
"Typical ECG evolution follows four stages: (1) PR depression and/or diffuse ST segment elevation, (2) normalization of ST segment, (3) T wave inversion with or without ST segment depression, and (4) normalization." — Braunwald's Heart Disease

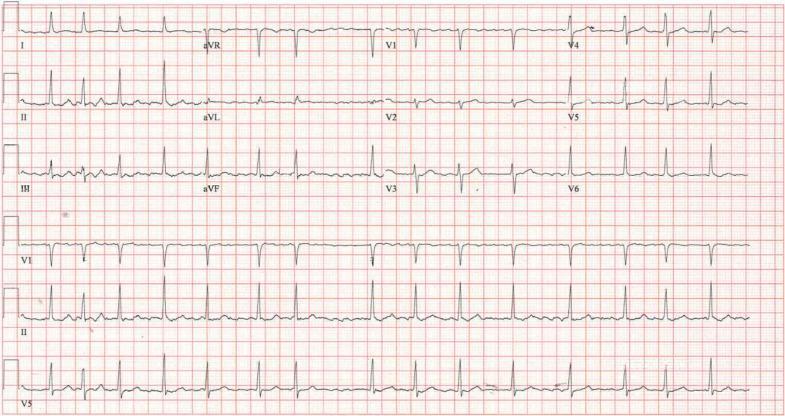
5. Complete (Third-Degree) AV Block
Disease overview: All atrial impulses fail to conduct to the ventricles. The atria and ventricles beat independently — driven by separate pacemakers. Causes include ischaemia (inferior MI → AV nodal block; anterior MI → infra-Hisian block), Lyme disease, autoimmune disease, infiltrative cardiomyopathy.
ECG Features:
- Complete AV dissociation: P waves and QRS complexes occur at independent rates (P rate > QRS rate)
- P waves "march through" QRS complexes and T waves with no fixed PR interval
- Escape rhythm QRS: Narrow (junctional, ~40–60 bpm) if block is at AV node level; Wide (ventricular, ~20–40 bpm, QRS > 120ms) if block is infra-Hisian
- Slow ventricular rate → risk of syncope (Stokes-Adams attack)
Second-degree blocks (precursor):
- Mobitz I (Wenckebach): PR progressively lengthens → dropped beat; benign, usually at AV node
- Mobitz II: Fixed PR interval, abrupt dropped beats; more serious, infra-Hisian, risks progression to complete block
"First-degree AV block — conduction delay results in PR interval >200ms. Mobitz type II block carries less favourable long-term prognosis and is characterised by abrupt AV conduction block without evidence of progressive conduction delay." — Washington Manual of Medical Therapeutics

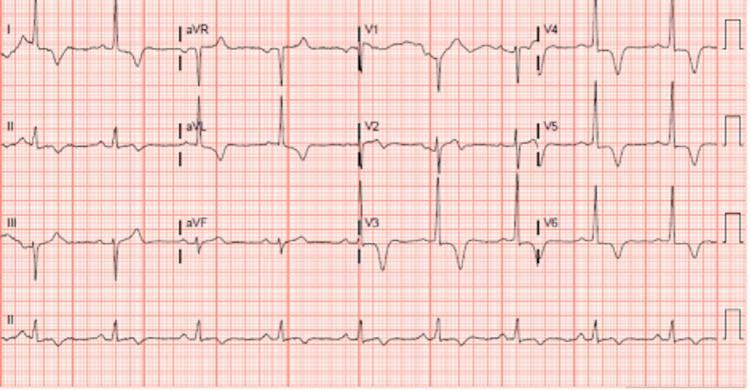
6. Hypertrophic Cardiomyopathy (HCM)
Disease overview: Genetic sarcomeric protein mutation (most commonly β-myosin heavy chain) causing asymmetric septal hypertrophy. The leading cause of sudden cardiac death in young athletes. Hypertrophied muscle creates abnormal depolarisation and repolarisation.
ECG Features:
- Left ventricular hypertrophy (LVH) voltage criteria: Deep S in V1 + tall R in V5/V6 ≥35 mm (Sokolow-Lyon)
- Narrow ("septal") Q waves in lateral leads (I, aVL, V5, V6) — from exaggerated septal depolarisation
- T-wave abnormalities: Upright T waves in leads with septal Q waves (in obstructive HCM); giant deep T-wave inversions (>10 mm) in apical HCM (Yamaguchi variant)
- ST depression / strain pattern in lateral leads
- Left axis deviation
- Atrial fibrillation or flutter may coexist
"Deep S-wave voltage (28 mm in V3) signifies LVH, and narrow septal Q waves in V5 and V6 are noted. T waves are upright in the leads with the septal Q waves." — Tintinalli's Emergency Medicine, describing the HCM ECG
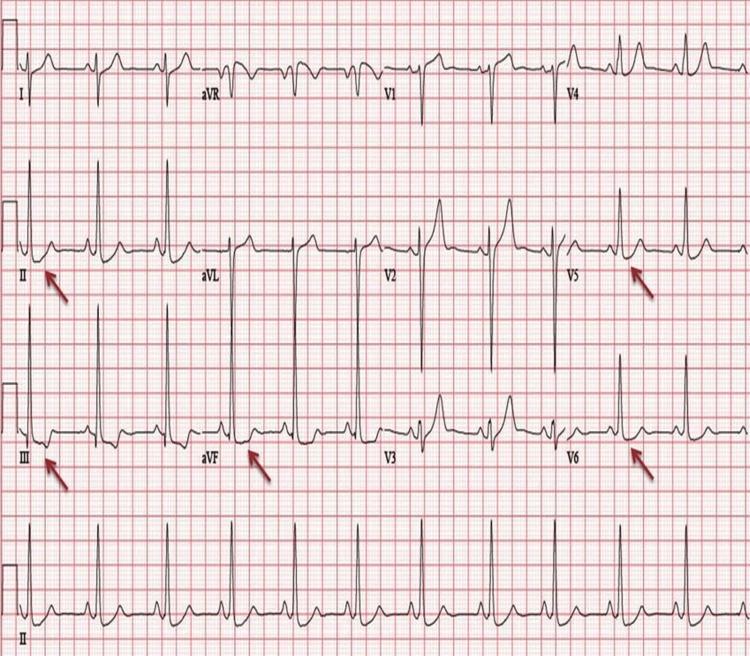
7. Left Ventricular Hypertrophy (LVH) — Hypertensive Heart Disease
Disease overview: Chronic pressure overload (hypertension, aortic stenosis) causes concentric LV hypertrophy. The increased muscle mass generates higher-amplitude electrical potentials.
ECG Features:
- High QRS voltage (Sokolow-Lyon criteria): S in V1 + R in V5 or V6 ≥35 mm
- Cornell criteria: R in aVL >11 mm; or R aVL + S V3 >20 mm (women) / >28 mm (men)
- "Strain pattern": ST depression + asymmetric T-wave inversion in lateral leads (I, aVL, V4–V6) — a marker of severe LVH/subendocardial ischaemia
- Left axis deviation
- Left atrial enlargement (P mitrale: broad, notched P in lead II; biphasic P in V1)
8. Pulmonary Embolism (PE)
Disease overview: Acute obstruction of the pulmonary circulation causes sudden right ventricular pressure overload (acute cor pulmonale). This shifts the cardiac electrical axis rightward and strains the RV.
ECG Features:
- Sinus tachycardia — the most common ECG finding (seen in ~44% of PE patients)
- S1Q3T3 pattern (McGinn-White sign): Deep S wave in lead I + Q wave in lead III + T-wave inversion in lead III (present in ~20%; sensitive but not specific)
- Right axis deviation
- Right bundle branch block (RBBB) — complete or incomplete
- T-wave inversions in V1–V4 (right ventricular strain pattern)
- ST elevation in aVR
- Sinus tachycardia is often the only finding in smaller emboli
The S1Q3T3 pattern reflects a rightward axis shift and clockwise rotation from acute right heart pressure overload.
9. Wolff-Parkinson-White (WPW) Syndrome
Disease overview: An accessory conduction pathway (Bundle of Kent) bypasses the AV node, causing pre-excitation of part of the ventricle. This creates the characteristic ECG triad and predisposes to re-entrant tachyarrhythmias (SVT, AF with rapid ventricular response — potentially fatal).
ECG Features — Classic Triad:
| Feature | Description |
|---|---|
| Short PR interval | <120 ms — AV node delay is bypassed |
| Delta wave | Slurred, slow upstroke at the start of QRS — ventricular myocardium pre-excited before normal His-Purkinje activation |
| Wide QRS | >120 ms — fusion of delta wave + normal conduction creates a widened complex |
Secondary changes: ST-T wave abnormalities (discordant to QRS) are secondary to abnormal depolarisation — do not indicate ischaemia.
Pathway localisation from delta wave polarity:
- Positive delta in V1 → left-sided pathway
- Negative delta in inferior leads (II, III, aVF) → posteroseptal pathway
- May produce "pseudoinfarction" Q waves mimicking inferior MI

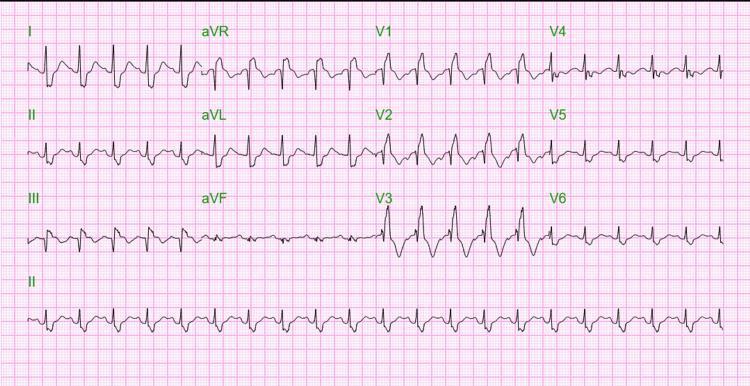
10. Long QT Syndrome (LQTS)
Disease overview: Congenital (mutations in cardiac ion channel genes — KCNQ1, KCNH2, SCN5A) or acquired (drugs, electrolyte disturbances) prolongation of ventricular repolarisation. Predisposes to the life-threatening polymorphic ventricular tachycardia torsades de pointes (TdP), which can degenerate to ventricular fibrillation.
ECG Features:
- Prolonged QTc interval: QTc >450 ms (men), >460 ms (women) — corrected using Bazett formula (QTc = QT ÷ √RR)
- T-wave morphology varies by subtype:
- LQTS1: Broad, prolonged T wave
- LQTS2: Low-amplitude, notched/bifid T wave
- LQTS3: Long flat ST segment → late-onset narrow T wave
- Torsades de Pointes: Polymorphic VT with a classic "twisting" of QRS complexes around the isoelectric baseline; initiated by a long-short R-R sequence ("R-on-T")

Summary Table
| # | Disease | Key ECG Finding | Leads Most Affected |
|---|---|---|---|
| 1 | STEMI | ST elevation → Q waves | Territory-specific (II,III,aVF / V1–V6) |
| 2 | NSTEMI/UA | ST depression, T inversion | Ischaemic territory |
| 3 | Atrial Fibrillation | No P waves, irregularly irregular | All leads |
| 4 | Acute Pericarditis | Diffuse saddle ST elevation, PR depression | All except aVR, V1 |
| 5 | Complete AV Block | AV dissociation, slow escape rhythm | All leads |
| 6 | Hypertrophic Cardiomyopathy | LVH voltage, narrow Q waves, giant T inversions | V5–V6, lateral leads |
| 7 | LVH (Hypertensive) | High voltage, strain pattern | V1, V5–V6, I, aVL |
| 8 | Pulmonary Embolism | S1Q3T3, sinus tachycardia, RBBB | I, III, V1–V4 |
| 9 | WPW Syndrome | Short PR, delta wave, wide QRS | All leads |
| 10 | Long QT Syndrome | Prolonged QTc, torsades de pointes | All leads |
Sources: Tintinalli's Emergency Medicine; Medical Physiology (Boron & Boulpaep); Braunwald's Heart Disease; Washington Manual of Medical Therapeutics; Fuster and Hurst's The Heart, 15th Ed; Goldman-Cecil Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.