I now have comprehensive, detailed content from both Fishman's and Murray & Nadel's. Let me compile the full 15-mark MD exam answer.
Pulmonary Sarcoidosis - Comprehensive MD Exam Answer (15 Marks)
Sources: Fishman's Pulmonary Diseases and Disorders (Chapter 53 - Systemic Sarcoidosis) and Murray & Nadel's Textbook of Respiratory Medicine (Chapter 93)
1. DEFINITION
Sarcoidosis is a systemic disorder characterized by noncaseating (non-necrotizing) granulomatous inflammation at sites of disease. Although any organ can be involved, the disease most commonly affects the lungs and intrathoracic lymph nodes. The diagnosis requires a compatible clinical and radiographic presentation, confirmed by biopsy showing noncaseating epithelioid granulomas in more than one organ, with exclusion of granulomatous disorders of known cause.
- Fishman's Pulmonary Diseases and Disorders, p. 922
2. HISTORICAL EPONYMS (High-Yield for Exams)
| Eponym | Description |
|---|
| Hutchinson/Boeck disease | Original description of cutaneous "Mortimer's malady" (1870s-1890s) |
| Löfgren syndrome | Acute sarcoidosis triad: erythema nodosum + bilateral hilar adenopathy + periarticular ankle inflammation/arthritis; high rate of spontaneous remission |
| Heerfordt (uveoparotid fever) | Uveitis + parotitis + fever + bilateral hilar adenopathy; diagnosis without biopsy |
| Panda sign | Bilateral parotid + lacrimal gland uptake on gallium-67 scan |
| Lambda sign | Bilateral hilar + right paratracheal lymph node uptake on gallium-67 |
| Kveim test | Intradermal injection of sarcoidosis tissue extract - forms granuloma in 4-6 weeks; >80% sensitivity; historically used, now abandoned due to biosafety concerns |
| Schaumann bodies | Lamellated calcified inclusions in giant cells |
| Asteroid bodies | Star-shaped inclusions in giant cells |
| Hamazaki-Wesenberg bodies | Pigmented oval inclusions |
- Fishman's, p. 922; Murray & Nadel's, p. 2134
3. EPIDEMIOLOGY
-
Worldwide distribution: highest prevalence in Scandinavia (Sweden: 160/100,000 prevalence); geographic clustering in Ireland and Italy suggests environmental triggers
-
United States: highest prevalence in southeastern coastal states
-
Racial disparities: Black Americans have higher incidence (17.8/100,000/year) vs. white Americans (8.1/100,000), higher mortality, and more severe disease (lupus pernio, cardiac involvement more common)
-
Age of onset: Peak 40-55 years (not young adulthood as previously thought); possibly bimodal - younger males and older females
-
Gender: Males have higher prevalence in Sweden but Black American women in the US have the highest risk
-
Genetics: Higher prevalence among first-degree relatives; HLA genes (MHC locus) show strongest genetic association; NOD2 mutations linked to Blau syndrome (pediatric granulomatous disease)
-
Mortality: Lung fibrosis, pulmonary hypertension, and older age are risk factors for death; deaths significantly higher in Black Americans
-
Fishman's, pp. 922-924
4. ETIOLOGY AND PATHOGENESIS
Proposed Etiology
Sarcoidosis results from the combined effects of genetic susceptibility and environmental/microbial exposures, triggering aberrant immune responses. No single causative agent identified.
Candidate antigens include:
- Mycobacterial antigens: mKatG (mycobacterial catalase-peroxidase) and ESAT-6 are the most-studied candidate pathogenic antigens, provoking adaptive T-cell responses in subsets of patients
- Propionibacterium acnes (especially in Japanese patients)
- Organic dusts, metals (beryllium), and inorganic particles
Immunopathogenesis (Key Steps)
Step 1 - Innate immune activation:
- Microbial/environmental antigens activate innate receptors: TLR2 (Toll-like receptor 2) and NOD1/NOD2 pathways
- Serum amyloid A (SAA) is an endogenous TLR2 ligand expressed in sarcoidosis tissues - drives TNF production, creating a positive feedback loop of granulomatous inflammation
- Enhanced TLR2 responsiveness found in blood and BAL cells from sarcoidosis patients
Step 2 - Adaptive immune response (granuloma formation):
- CD4+ T helper cells (Th1 skewed) predominate: produce IFN-γ, TNF, IL-2, IL-12
- IFN-γ and TNF (from "multifunctional" CD4+ T cells) drive macrophage activation into epithelioid cells
- CD4:CD8 ratio in BAL is elevated (>3.5:1) - a characteristic finding (normal ~1.7:1)
- Granuloma forms: central core of epithelioid macrophages + multinucleated giant cells surrounded by CD4+ T lymphocytes peripherally, with CD8+ suppressor T cells in the outer rim
Step 3 - Lung fibrosis:
-
TGF-β (transforming growth factor-beta) is the key mediator of fibrosis in sarcoidosis
-
Disease-specific T-cell and macrophage activation promotes progressive fibrosing inflammation in a subset of patients
-
Th17 pathway has also been implicated in fibrotic sarcoidosis
-
Fishman's, pp. 925-931; Murray & Nadel's
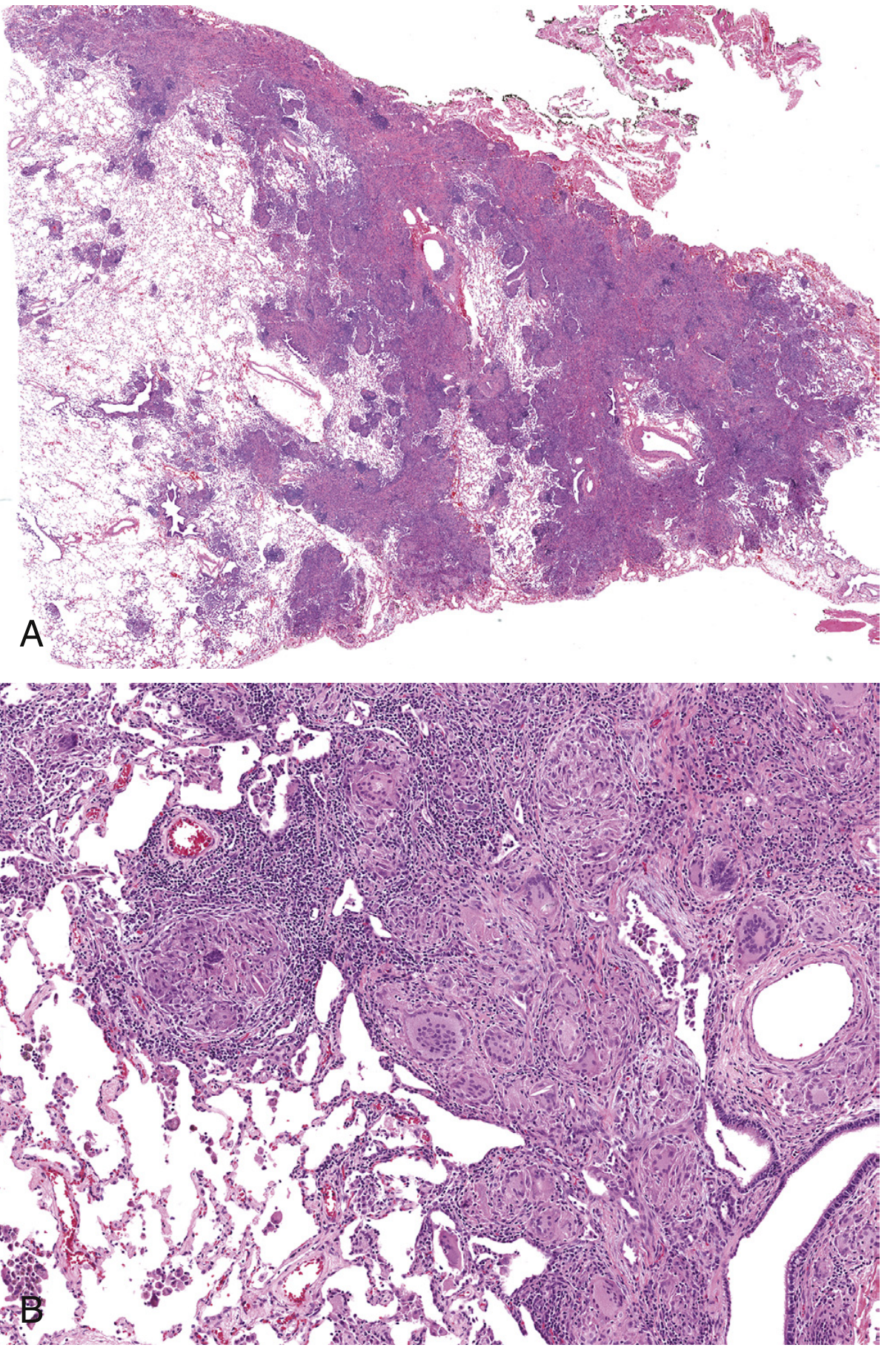
5. PATHOLOGY
The histologic hallmark is the non-necrotizing (non-caseating) granuloma:
- Compact, well-formed rounded aggregates of epithelioid macrophages
- Multinucleated giant cells (formed by macrophage fusion)
- Peripheral rim of lymphocytes (CD4+ T cells)
- No significant necrosis - necrosis strongly favors infection
- Inclusions (non-specific, non-diagnostic): Schaumann bodies, asteroid bodies, Hamazaki-Wesenberg bodies, birefringent crystals
- Surrounded by variable fibrosis/sclerotic stroma in established lesions
Pulmonary Distribution - The "Lymphangitic" Pattern (Pathognomonic)
Sarcoidal granulomas follow lymphatic routes in the lung, producing the characteristic "perilymphatic" distribution seen on HRCT:
- Along bronchovascular bundles
- Along interlobular septa
- Along the pleura (subpleural)
- Mediastinal lymph node involvement in most cases
Figure: Pulmonary sarcoidosis histopathology - Murray & Nadel's Textbook of Respiratory Medicine
Special stains routinely performed: Acid-fast bacilli (AFB) stain to exclude mycobacteria; Gomori methenamine silver (GMS) to exclude fungi.
- Murray & Nadel's, pp. (block 6); Fishman's, p. 931
6. CLINICAL FEATURES
Presentation Patterns
A. Asymptomatic (30-50%): Discovered incidentally on chest X-ray (e.g., bilateral hilar adenopathy on pre-employment screening)
B. Acute (Löfgren syndrome): Erythema nodosum + bilateral hilar adenopathy + periarticular ankle inflammation; fever; predominantly in white Europeans and Puerto Ricans; excellent prognosis with spontaneous remission >90%
C. Subacute/chronic: Insidious dyspnea, dry cough, chest tightness; constitutional symptoms (fatigue, weight loss, fever, night sweats)
Pulmonary Features
- Dyspnea (most common symptom in pulmonary disease)
- Dry cough
- Chest pain (pleuritic or atypical)
- Wheezing (from endobronchial involvement or airway hyperresponsiveness)
- Hemoptysis (uncommon; occurs with fibrocystic disease or Aspergillus colonization)
- Respiratory failure (advanced fibrotic disease)
Extrapulmonary Manifestations
| Organ | Frequency | Key Features |
|---|
| Lymph nodes | >90% (intrathoracic); peripheral ~30% | Bilateral hilar adenopathy; painless peripheral lymphadenopathy |
| Eye | 20-30% | Anterior uveitis most common; also conjunctivitis, optic neuritis; can cause blindness |
| Skin | 20-30% | Lupus pernio (violaceous nasal plaques - specific to sarcoidosis), erythema nodosum (non-granulomatous), plaques, subcutaneous nodules |
| Liver | ~50-70% (pathologic); <30% symptomatic | Hepatomegaly, elevated ALP, portal hypertension (rare) |
| Spleen | ~40% (pathologic) | Splenomegaly, cytopenias |
| Bone marrow | variable | Cytopenias, hypercalcemia |
| Cardiac | <10% clinical; >20% autopsy (US); >50% autopsy (Japan) | Arrhythmias, AV block, sudden death, dilated cardiomyopathy |
| Neurologic (Neurosarcoidosis) | ~5-10% | Cranial nerve palsies (CN VII most common), aseptic meningitis, hypothalamic/pituitary involvement (diabetes insipidus), myelopathy |
| Upper respiratory | 5-10% | Nasal congestion, epistaxis, saddle nose deformity; laryngeal sarcoidosis (hoarseness, stridor) |
| Musculoskeletal | ~10-15% | Acute polyarthropathy (Löfgren), bone cysts (punched-out lesions), myopathy |
| Renal | ~5% | Hypercalciuria → nephrolithiasis; granulomatous nephritis; nephrocalcinosis |
| Endocrine | rare | Hypercalcemia (activated macrophages produce 1,25-OH vitamin D), diabetes insipidus (pituitary/hypothalamic involvement) |
| Parotid/Lacrimal | rare | Heerfordt syndrome (uveoparotid fever): diagnostic without biopsy |
Note on Hypercalcemia: Caused by ectopic production of 1,25-dihydroxyvitamin D (calcitriol) by activated macrophages within granulomas - a key high-yield mechanism.
7. CHEST RADIOGRAPHIC STAGING (Scadding Classification)
| Stage | Radiographic Finding | Prevalence at Presentation | Remission Rate |
|---|
| Stage 0 | Normal chest radiograph | ~5-10% | - |
| Stage I | Bilateral hilar lymphadenopathy (BHL) alone | ~50% | 60-80% (high spontaneous remission) |
| Stage II | BHL + pulmonary infiltrates/parenchymal opacities | ~25% | 40-70% |
| Stage III | Pulmonary infiltrates WITHOUT hilar adenopathy | ~15% | 10-20% |
| Stage IV | Pulmonary fibrosis (fibrocystic stage) | ~5% | Poor; irreversible |
Stage I has the best prognosis - up to 80% spontaneous remission. Staging does not perfectly predict progression or treatment response.
- Fishman's; Murray & Nadel's
8. HIGH-RESOLUTION CT (HRCT) FINDINGS
The HRCT pattern reflects the perilymphatic distribution:
- Bilateral upper lobe predominance of micronodules (2-5 mm)
- Perilymphatic/bronchovascular distribution - nodules cluster along bronchovascular bundles, interlobular septa, and pleura
- Bilateral hilar and mediastinal lymphadenopathy - often "eggshell" calcification in chronic disease
- "Galaxy sign" - large conglomerate masses with satellite micronodules (highly specific)
- "Sarcoid cluster sign" / beaded fissures
- Ground-glass opacity (active alveolitis)
- Advanced/stage IV: traction bronchiectasis, honeycombing, bullae, cysts, fibrocystic upper lobe scarring with hilar retraction upward
9. PULMONARY FUNCTION TESTS (PFTs)
| Pattern | Finding | Explanation |
|---|
| Restrictive (most common) | ↓ FVC, ↓ TLC, FEV1/FVC normal or ↑ | Granulomatous infiltration + fibrosis |
| Obstructive (~30%) | ↓ FEV1/FVC | Endobronchial involvement, airway granulomas, large-airway compression by nodes |
| Mixed | Both patterns | Advanced disease |
| DLCO (diffusing capacity) | Reduced (early sensitive marker) | Gas exchange impairment, alveolitis |
| 6-minute walk test | ↓ Distance, desaturation | Exercise-induced hypoxemia |
Spirometry, diffusing capacity (DLCO), and lung volumes are the recommended initial PFTs for all sarcoidosis patients.
10. DIAGNOSIS
Diagnostic Criteria
- Compatible clinical + radiographic presentation
- Histologic confirmation: Noncaseating epithelioid granulomas in ≥1 organ
- Exclusion of other causes: especially infections (tuberculosis, fungal) and other granulomatous diseases (berylliosis, hypersensitivity pneumonitis, Crohn disease, etc.)
Situations Where Biopsy Can Be Avoided (Clinical Diagnosis)
- Löfgren syndrome: erythema nodosum + bilateral hilar adenopathy + ankle periarthritis
- Heerfordt syndrome: uveoparotid fever (uveitis + parotitis + fever + BHL)
- Bilateral hilar adenopathy on chest radiograph without symptoms (after excluding lymphoma/TB)
Biopsy Sites (in order of preference - least invasive)
- Transbronchial biopsy (TBB) - diagnostic in 40-90% of pulmonary sarcoidosis; preferred first-line approach
- Endobronchial biopsy - even without visible lesions, yield ~40-60%
- EBUS-guided transbronchial needle aspiration (EBUS-TBNA) - high yield for mediastinal nodes (>80%)
- Skin, conjunctival biopsy (if lesions present - easy access)
- Surgical lung biopsy (VATS) - reserved for diagnostic uncertainty
- Liver, lymph node biopsy when clinically indicated
Laboratory Investigations
| Test | Finding | Comment |
|---|
| Serum ACE (sACE) | Elevated in 30-80% | Produced by epithelioid macrophages; low specificity (also elevated in TB, histoplasmosis, diabetes, cirrhosis, silicosis); useful for monitoring, NOT diagnosis |
| Serum calcium | Elevated in ~10-15% | Due to ectopic 1,25-(OH)2 vitamin D by macrophages |
| Urinary calcium (24-hr) | Elevated (hypercalciuria) | More common than hypercalcemia |
| 1,25-(OH)2 vitamin D | Elevated | Pathognomonic mechanism |
| LFTs (ALP) | Elevated in hepatic involvement | |
| CBC | Lymphopenia, anemia, thrombocytopenia | |
| LDH | Elevated in active disease | Non-specific |
| IFN-γ release assay (IGRA) | Done to exclude TB | Recommended at initial evaluation |
| BAL CD4:CD8 ratio | >3.5:1 (elevated) | Supportive (normal ~1.7:1); lymphocytosis in BAL |
| Gallium-67 scan | Panda sign + lambda sign | Replaced by FDG-PET in modern practice |
| FDG-PET | Identifies active inflammatory sites | Used to guide biopsy, assess disease activity, detect cardiac/extrapulmonary disease |
No diagnostic biomarker currently exists for sarcoidosis - it remains a diagnosis of exclusion.
- Fishman's, pp. 935-936; Murray & Nadel's, pp. 2130-2138
11. PROGNOSIS AND DISEASE COURSE
- ~50-60% of patients have spontaneous remission within 1-3 years, especially Stage I disease
- ~20-30% have chronic persistent disease requiring long-term therapy
- ~5-10% have progressive disease with irreversible organ damage
- Prognostic indicators of poor outcome:
- Black race, older age at diagnosis
- Stage III/IV radiographic disease
- Lupus pernio (indicates chronic systemic disease)
- Cardiac sarcoidosis
- Neurosarcoidosis
- Pulmonary hypertension
- Requirement for treatment at diagnosis
- Patients needing treatment at diagnosis have a 2-fold increased risk of death (Swedish registry data)
12. TREATMENT
When to Treat
Many patients are asymptomatic and do not require immediate treatment; spontaneous remission is common in the first 6 months. Treatment decision is based on:
- Significant symptoms
- Decline in pulmonary function (FVC or DLCO)
- Threatened vital organ function (cardiac, neurologic, ocular, renal)
- Hypercalcemia
First-Line: Corticosteroids
Prednisone remains the mainstay of treatment for sarcoidosis:
- Initial dose: 20-40 mg/day (some guidelines use 0.5 mg/kg/day)
- Response usually within 1 month
- Taper slowly over months once improvement achieved
- 50% relapse rate when withdrawn after >2 years of therapy
- Patients not responding to prednisone 40 mg/day are considered steroid-refractory
Second-Line: Steroid-Sparing (Cytotoxic) Agents
Used when:
-
1 year of corticosteroid therapy required
- Significant steroid side effects
- Steroid-refractory disease
| Drug | Dose/Route | Main Uses | Key Toxicity |
|---|
| Methotrexate | 10-15 mg/week (oral) | Most widely used; effective for pulmonary, ocular, cutaneous, neurologic, sinonasal disease | Hepatotoxicity, pulmonary toxicity, bone marrow suppression |
| Azathioprine | 50-200 mg/day | Steroid-sparing, pulmonary and systemic disease | Hepatotoxicity, bone marrow suppression |
| Leflunomide | 10-20 mg/day | Often combined with methotrexate | Peripheral neuropathy, hepatotoxicity |
| Mycophenolate mofetil | 1-3 g/day | Pulmonary, cutaneous disease | GI side effects |
Third-Line: Antimalarial Agents
- Hydroxychloroquine (preferred) or chloroquine
- Effective for: cutaneous disease, sinonasal disease, hypercalcemia, fatigue
- Dose: hydroxychloroquine <5 mg/kg real body weight to minimize ocular toxicity
- Routine ophthalmologic monitoring required
Biologic Agents
- Anti-TNF agents: Infliximab and adalimumab are used for refractory sarcoidosis
- Infliximab: Level 1 evidence from RCTs for pulmonary sarcoidosis (improves FVC)
- Reserved for patients failing conventional immunosuppressive therapy
Other Interventions
-
Lung transplantation: For end-stage stage IV sarcoidosis; sarcoidosis can recur in transplanted lung
-
Cardiac pacemaker/ICD: For cardiac sarcoidosis with AV block or ventricular arrhythmias
-
Pulmonary rehabilitation: For patients with chronic pulmonary disability
-
Murray & Nadel's, pp. 2134-2138; Fishman's, pp. 940-944
13. SPECIAL SUBTYPES
Fibrocystic (Stage IV) Sarcoidosis
- Extensive mid and upper lung scarring with bullous and cystic changes
- Hilar retraction upward
- Complicated by Aspergillus colonization (aspergilloma in bullae) and hemoptysis
- Pulmonary hypertension is common in this stage
Sarcoidosis-Associated Pulmonary Hypertension (SAPH)
- More common than previously recognized
- Mechanisms: pulmonary vascular granulomas, extrinsic compression of pulmonary arteries by mediastinal nodes, hypoxic vasoconstriction, cardiac sarcoidosis, porto-pulmonary hypertension
- Carries a particularly poor prognosis
- Responds poorly to pulmonary arterial hypertension (PAH)-specific therapy
Necrotizing Sarcoid Granulomatosis
- Rare variant with extensive necrosis within granulomas + vasculitis
- Usually presents as lung nodules; generally a benign course
Parasarcoidosis Syndromes
- Inflammatory manifestations not due to direct granulomatous involvement
- Include: fatigue/sarcoidosis-associated fatigue (most common complaint, often refractory), small-fiber neuropathy, cognitive impairment
- Refractory to standard anti-inflammatory treatment
14. DIFFERENTIAL DIAGNOSIS
| Condition | Key Differentiating Feature |
|---|
| Tuberculosis | Caseating (necrotizing) granulomas; AFB positive; positive TST/IGRA |
| Hypersensitivity pneumonitis | Upper lobe granulomas + centrolobular nodules on HRCT; antigen exposure history; CD4:CD8 <1 in BAL |
| Berylliosis | Clinically/histologically identical to sarcoidosis; beryllium lymphocyte proliferation test (BeLPT) distinguishes |
| Lymphoma | No granulomas on biopsy; Reed-Sternberg cells; PET/CT pattern different |
| Histoplasmosis/Coccidioidomycosis | Fungal staining positive; serology |
| Wegener's/GPA | Necrotizing granulomatous vasculitis; c-ANCA/PR3-ANCA positive |
| Löfgren syndrome mimics | Always confirm with clinical criteria; erythema nodosum can occur in other conditions |
15. SUMMARY MEMORY AIDS (High-Yield Points for Exams)
- Noncaseating granuloma = pathologic hallmark - NO necrosis
- Perilymphatic distribution on HRCT = most specific radiologic pattern
- BAL CD4:CD8 >3.5:1 = characteristic immunological finding
- sACE elevated in 30-80% but NOT specific; used for monitoring
- Hypercalcemia = ectopic 1,25-(OH)2 Vit D from activated macrophages
- Stage I = best prognosis (80% spontaneous remission); Stage IV = irreversible fibrosis
- Löfgren syndrome = erythema nodosum + BHL + ankle arthritis = diagnose without biopsy
- Heerfordt syndrome = uveoparotid fever = diagnose without biopsy
- EBUS-TBNA = preferred bronchoscopic approach for mediastinal node sampling (>80% yield)
- Prednisone 20-40 mg/day = first-line treatment; taper slowly; 50% relapse on withdrawal
- Methotrexate = most used steroid-sparing agent
- Infliximab = anti-TNF biologic for refractory disease (level 1 evidence)
- Lupus pernio = chronic severe sarcoidosis marker; violaceous facial plaques
- Cardiac sarcoidosis = can cause sudden death from arrhythmia; requires screening ECG in all patients
- Disease results from genetic susceptibility (HLA genes) + environmental/microbial triggers → aberrant Th1-driven immune response → noncaseating granulomatous inflammation
Sources:
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set (Chapter 53: Systemic Sarcoidosis), pp. 922-944
- Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume (Chapter 93), pp. 2128-2145