Supine hypotension syndrome from anaesthesia textbooks standard as an exam answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
I have everything needed for a comprehensive exam answer. Here it is:
Supine Hypotension Syndrome (Aortocaval Compression Syndrome)
Definition
Supine hypotension syndrome is defined as a decrease in mean arterial pressure of >15 mmHg with a compensatory increase in heart rate of >20 beats/min when a term parturient lies supine, caused by compression of the inferior vena cava (IVC) and aorta by the gravid uterus.
— Miller's Anesthesia 10e
Incidence
- IVC compression occurs in nearly all term parturients in the supine position
- Symptomatic supine hypotension syndrome occurs in only 8–10% of women (Miller's) — also quoted as ~5% (Morgan & Mikhail's)
- Significant aortoiliac artery compression occurs in 15–20% of pregnant patients
Mechanism / Pathophysiology
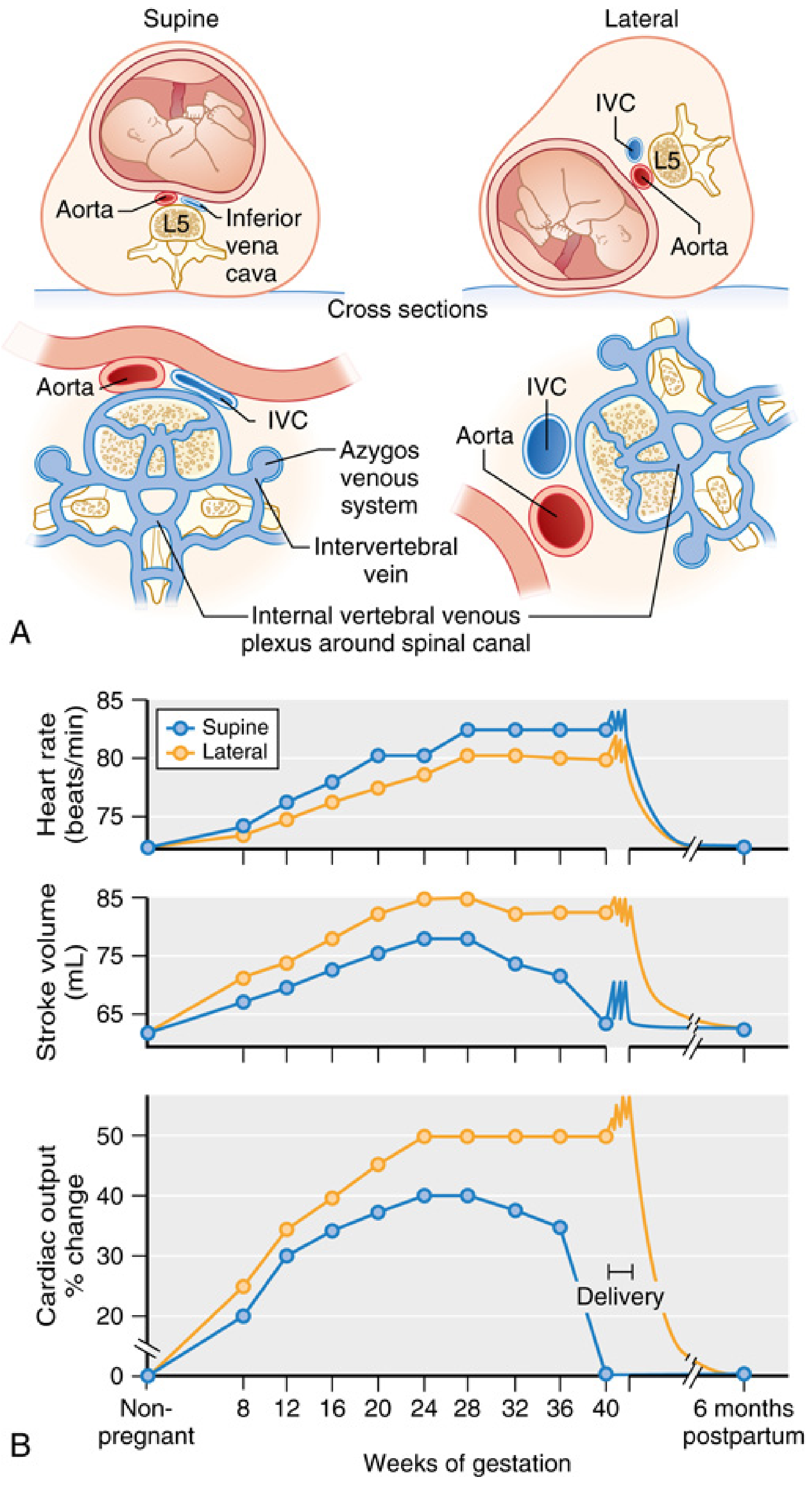
- IVC compression by the gravid uterus at L5 → ↓ venous return → ↓ preload → ↓ stroke volume → ↓ cardiac output (10–20% reduction vs upright position)
- Aortic compression → ↓ uteroplacental blood flow (independent of the BP at the brachial artery — femoral and uterine artery pressures may be critically low even when arm BP appears maintained)
- Collateral venous return: Blood from the lower extremities is diverted via the epidural venous plexus, azygos, and vertebral veins, which become engorged → contributes to distension of epidural veins (relevant to neuraxial blocks)
- Uterine contraction: Reduces caval compression but exacerbates aortic compression
Onset from approximately 20 weeks' gestation, worst at term.
Compensatory Responses
Most women do not become symptomatic because of intact compensatory mechanisms:
- Reflex sympathetic activation → ↑ systemic vascular resistance → maintains arterial blood pressure despite reduced cardiac output
- Therefore brachial artery BP may be falsely reassuring — uteroplacental flow can still be compromised
Key anaesthetic implication: Neuraxial and general anaesthesia abolish sympathetic compensation, unmasking the full haemodynamic effect of aortocaval compression. This is the principal reason supine positioning under anaesthesia is dangerous.
Clinical Features
- Hypotension
- Pallor
- Diaphoresis
- Nausea and vomiting
- Changes in mentation / dizziness
- Fetal bradycardia and acidosis (uteroplacental insufficiency)
Sequelae of Chronic Partial IVC Obstruction (Third Trimester)
- Venous stasis in lower limbs → oedema, varicosities, deep vein thrombosis
- Engorgement of epidural venous plexus → increased risk of intravascular injection during epidural placement; reduced epidural space volume → lower dose requirements for neuraxial blockade (30% reduction in local anaesthetic dose)
Prevention & Management
Positioning
- Avoid supine position whenever neuraxial blockade is used
- Left uterine displacement (LUD): Place a wedge or tilt table >15° under the right hip, displacing the uterus to the left
- Classic teaching: 15° tilt. This has been challenged — MRI studies show IVC volume is not significantly different between supine and 15° tilt; 30° tilt significantly increases IVC volume
- A randomised trial of spinal anaesthesia + phenylephrine infusion: no difference in neonatal acid-base status between supine and 15° tilt, but supine patients had lower cardiac output and required more phenylephrine
- Current recommendation (Miller's): Continue to use LUD during induction of neuraxial anaesthesia and during any episode of maternal hypotension or fetal compromise; further studies are needed to define optimal tilt angle
Vasopressors
- Phenylephrine (α-agonist): now preferred first-line vasopressor for neuraxial hypotension in obstetrics — more effective and associated with less fetal acidosis than ephedrine
- Ephedrine (mixed α/β): traditionally first-line but clinical evidence shows greater fetal acidosis (β-adrenergic effect increases fetal metabolism)
Morgan & Mikhail's Clinical Anesthesiology 7e, Key Concept 6
Immediate treatment of acute episode
- Turn patient to left lateral decubitus or full lateral position
- IV fluid bolus (co-load with spinal anaesthesia)
- Vasopressor (phenylephrine infusion preferred)
- Supplemental oxygen
- Assess fetal heart rate
Special Considerations Under Anaesthesia
| Anaesthetic type | Risk |
|---|---|
| Spinal (e.g., for LSCS) | Highest risk — sudden sympathectomy + aortocaval compression → precipitous hypotension |
| Epidural | Slower onset allows partial compensation; still significant |
| General anaesthesia | Volatile agents ↓ SVR; loss of sympathetic tone unmasks compression |
Exam Summary Points
- Mechanism = IVC + aorta compressed by gravid uterus at L5 after 20 weeks
- Incidence of symptomatic syndrome = ~5–10%; IVC compression = nearly all term patients
- Most women are asymptomatic because of intact sympathetic compensation — anaesthesia abolishes this
- CO drops 10–20% supine vs upright; aortic compression causes uteroplacental ischaemia even when arm BP is maintained
- Epidural vein engorgement (from IVC compression) = reduced epidural volume → lower LA doses needed + ↑ intravascular injection risk
- Treatment = LUD (>15–30°), lateral positioning, phenylephrine, IV fluid
- Left uterine displacement: 15° tilt is contested; 30° tilt is more effective; current practice maintains its use
Sources: Miller's Anesthesia 10e (Ch. 58 — Aortocaval Compression, pp. 8805–8809) | Morgan & Mikhail's Clinical Anesthesiology 7e (Ch. 40 — Maternal & Fetal Physiology, pp. 1571–1576)
This is a shared conversation. Sign in to Orris to start your own chat.