Discuss the uterus under the following headings: position, parts, external features, relation, blood supply, lymphatic drainage and clinical anatomy for 10 marks. MBBS Anatomy.
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
I now have all the content needed for a comprehensive 10-mark MBBS Anatomy answer on the uterus. Let me compile the full answer.
THE UTERUS
Sources: Color Atlas of Human Anatomy Vol. 2 (Thieme) | Gray's Anatomy for Students | Campbell-Walsh Urology
1. POSITION
The uterus is situated in the lesser (true) pelvis, in the midline, between the urinary bladder anteriorly and the rectum posteriorly. Its normal position is:
- Anteverted - the whole uterus is tilted forward (anteriorly) relative to the vaginal axis, so that the long axis of the uterus and the long axis of the vagina form an angle of about 90° (the angle of version).
- Anteflexed - the body of the uterus is bent anteriorly on the cervix at the level of the internal os (the angle of flexion, normally about 170°).
This combined anteverted-anteflexed position is the normal position in a woman with an empty bladder.
Position varies with bladder filling: When the bladder is full, the uterus is pushed posteriorly (retroversion). When the rectum is distended, the uterus moves anteriorly.
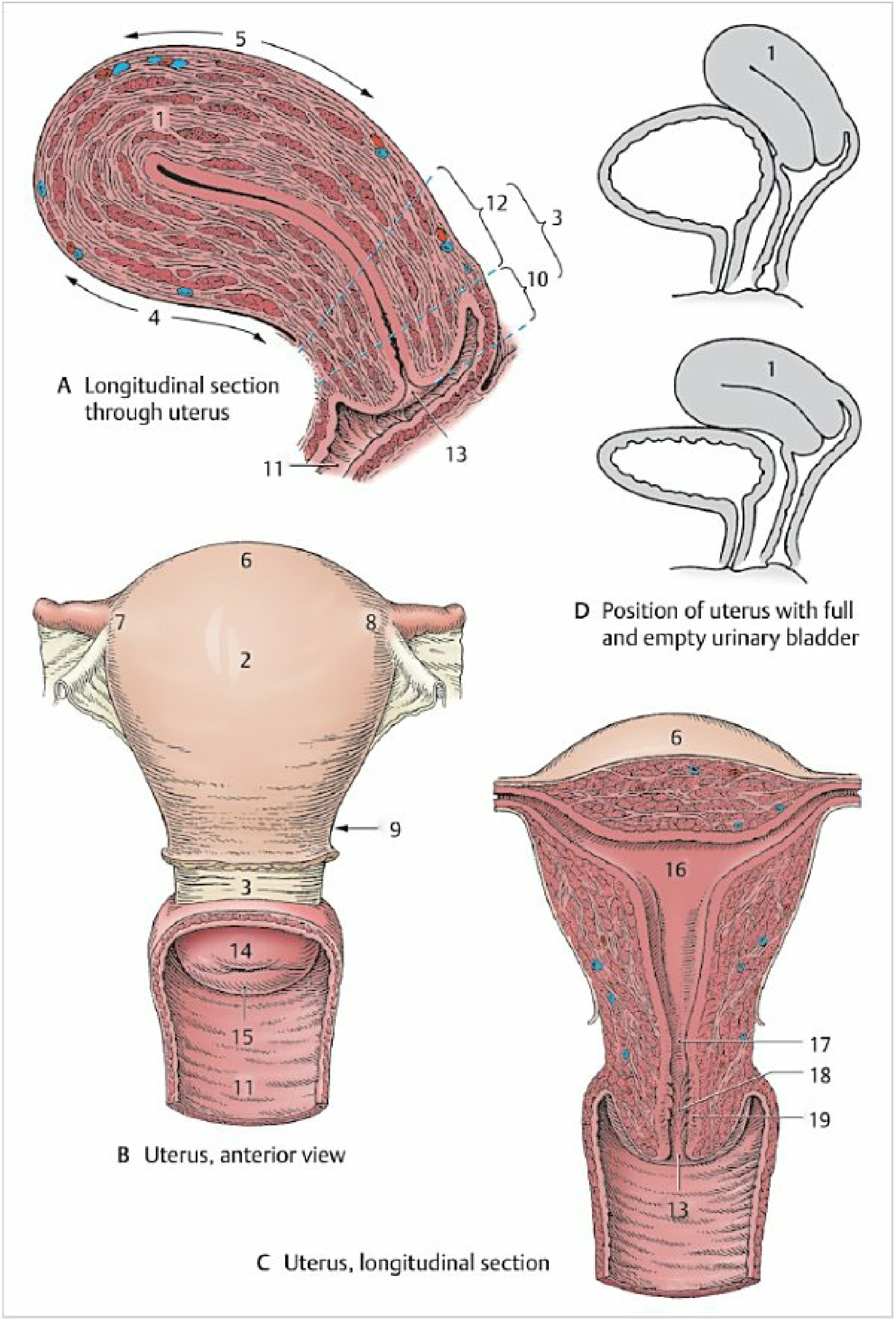
2. PARTS
The uterus is a thick-walled, pear-shaped muscular organ, approximately 7-8 cm long, 5 cm wide, and 2.5 cm thick, weighing 50-70 g in the nulliparous adult female. It has two main parts:
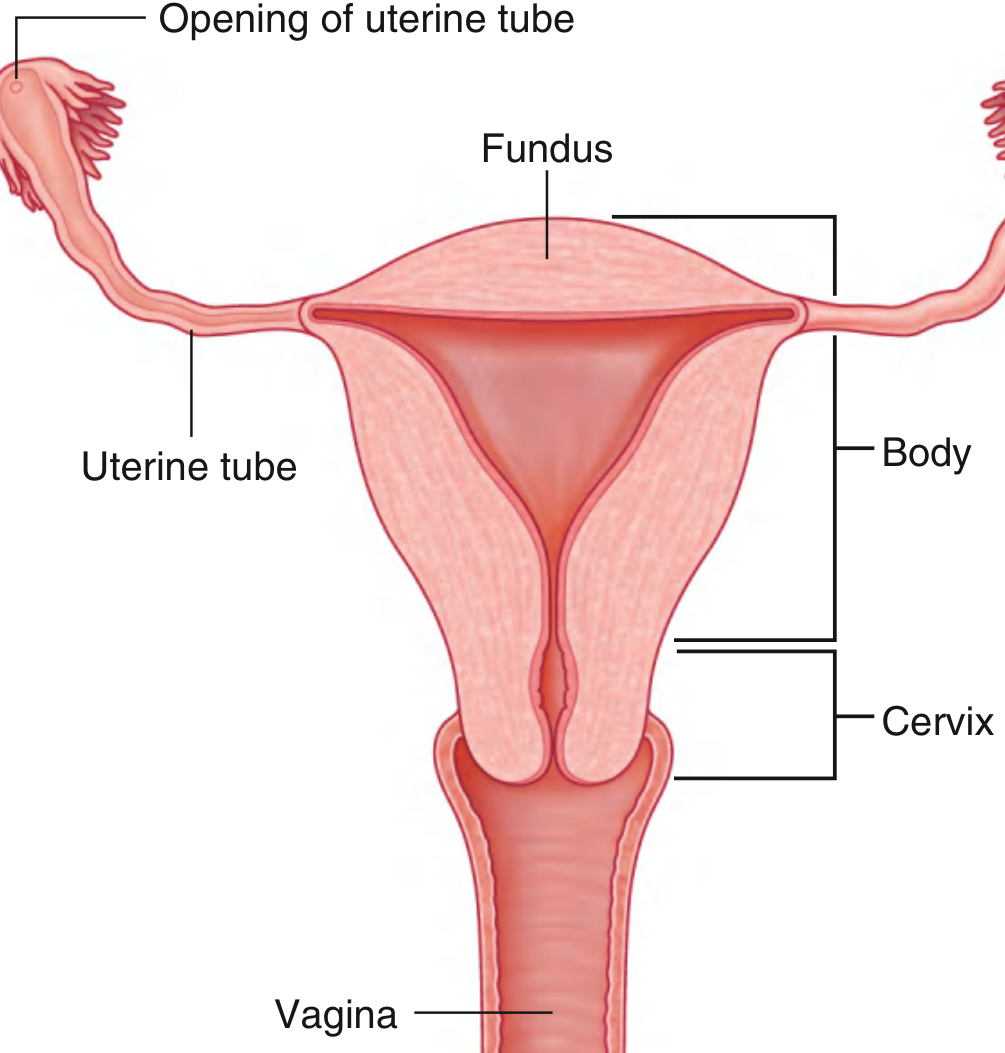
A. Body (Corpus Uteri) - Upper Two-Thirds
- Fundus - the rounded dome-shaped superior portion that lies above the openings of the uterine tubes (cornua). The fundus projects beyond the level of the uterine horns.
- Uterine Horns (Cornua) - the right and left upper corners of the body where the uterine tubes open into the uterine cavity.
- Isthmus - a narrow constriction between the body and the cervix, about 1 cm long. During pregnancy this expands to form the lower uterine segment.
- Uterine Cavity - the lumen of the body is a narrow triangular slit (in the frontal plane). The cavity measures about 6 cm from the external os to the fundus. The superior two corners open into the uterine tubes; the inferior apex narrows into the cervical canal.
B. Cervix (Neck) - Lower One-Third
- About 2.5 cm long.
- Divided into:
- Supravaginal part - lies above the vaginal attachment; related to the bladder anteriorly and to the parametrium laterally.
- Vaginal part (portio vaginalis) - projects into the vault of the vagina; visible on speculum examination.
- External os - the aperture of the cervical canal opening into the vagina. In a nulliparous woman it is circular; after vaginal delivery it becomes a horizontal slit.
- Cervical canal - spindle-shaped, lined by mucous membrane with palmate folds (arbor vitae). Contains cervical glands that produce mucus, acting as a plug (mucus plug).
3. EXTERNAL FEATURES (Surfaces and Layers)
Surfaces
| Surface | Description |
|---|---|
| Anterior (vesical) surface | Flattened; covered by peritoneum only above the isthmus (peritoneum reflects onto bladder as vesicouterine pouch) |
| Posterior (intestinal) surface | Convex; covered by peritoneum down to the posterior vaginal fornix |
| Lateral borders | Where the broad ligaments are attached; uterine tubes, round ligaments, and ovarian ligaments are attached here |
| Fundus | Rounded superior dome; fully covered by peritoneum |
Layers of the Uterine Wall (from inside out)
- Endometrium - the mucosal lining; undergoes cyclical changes during the menstrual cycle. Divided into a superficial stratum functionalis (shed at menstruation) and a deep stratum basalis (not shed; regenerates the functionalis).
- Myometrium - the thickest layer; composed of interlacing smooth muscle bundles arranged in three poorly defined layers (inner longitudinal, middle circular/oblique, outer longitudinal). Contracts powerfully during labour.
- Perimetrium (Serosa) - partial peritoneal covering. The body and fundus are fully covered; the supravaginal cervix is covered only posteriorly.
4. RELATIONS
Anterior
- Vesicouterine pouch (between uterus and bladder) - a shallow peritoneal recess formed between the anterior surface of the uterus and the posterior surface of the bladder. The floor of this pouch lies at the level of the junction of body and cervix.
- Below the pouch: the supravaginal cervix is in direct contact with the base of the urinary bladder (separated by loose areolar tissue only).
Posterior
- Rectouterine pouch (Pouch of Douglas) - a deep peritoneal depression between the posterior surface of the uterus/posterior vaginal fornix and the anterior surface of the rectum. It is the deepest point of the female peritoneal cavity.
- The pouch is bounded laterally by the rectouterine folds (uterosacral ligaments), which contain the sacrouterine ligaments and the inferior hypogastric nerve plexus.
Lateral
- Broad ligament (peritoneal fold) enclosing the uterine tubes, round ligament, and ovarian ligament.
- Ureter - crosses beneath the uterine artery (the clinical "water under the bridge" relationship) at the level of the supravaginal cervix, approximately 2 cm lateral to the cervix.
- Uterine vessels (in the parametrium).
Superior
- The fundus is related to coils of small intestine and sigmoid colon.
Inferior
- The cervix opens into the vagina through the external os.
Supports of the Uterus
| Ligament | Description |
|---|---|
| Round ligament | From uterine horn → inguinal canal → labium majus; maintains anteversion |
| Broad ligament | Peritoneal fold from lateral uterus to lateral pelvic wall |
| Uterosacral (sacrouterine) ligaments | Cervix → sacrum; strongest supports; maintain anteflexion |
| Transverse cervical (cardinal/Mackenrodt's) ligaments | Most important supports; from cervix and upper vagina to lateral pelvic wall |
| Pubocervical ligaments | Cervix → back of pubis |
| Pelvic floor (levator ani) | Main mechanical support |
5. BLOOD SUPPLY
Arterial Supply
The uterus receives its blood supply mainly from the uterine artery, a branch of the anterior division of the internal iliac artery.
- The uterine artery courses medially in subperitoneal connective tissue, crossing over the ureter (ureter lies below the uterine artery) to reach the lateral wall of the uterus near the cervix.
- At the lateral wall, it divides into:
- Ascending branch - runs tortuously along the lateral border of the uterus up to the fundus; gives off numerous arcuate and radial branches to the myometrium and endometrium.
- Descending branch (vaginal artery) - supplies the cervix and upper vagina.
- At the fundus, the ascending branch anastomoses with the ovarian artery (from the abdominal aorta) and gives off a tubal branch.
Additional supply from:
- Ovarian artery (supplies upper body and fundus via anastomosis)
- Vaginal artery (supplies cervix)
Venous Drainage
- A network of valveless veins forming the uterine venous plexus (in the parametrium) drains via the uterine veins into the internal iliac veins.
- The plexus connects with the vesical, vaginal, and rectal venous plexuses.
6. LYMPHATIC DRAINAGE
Lymph drains in three main directions, reflecting the three parts of the uterus:
| Region | Drainage |
|---|---|
| Body and Fundus (main route) | Along the suspensory ligament of the ovary (infundibulopelvic ligament) → para-aortic (lumbar) lymph nodes |
| Fundus (secondary route) | Along the round ligament through the inguinal canal → superficial inguinal lymph nodes |
| Body (lateral route) | Via the broad ligament → external iliac lymph nodes at the division of the common iliac artery |
| Cervix | External iliac, internal iliac, and obturator lymph nodes (via broad ligament); also to sacral lymph nodes posteriorly |
Clinical implication: Carcinoma of the cervix spreads to iliac nodes; carcinoma of the body/fundus spreads primarily to para-aortic nodes. This determines the field of lymph node dissection in gynaecological malignancies.
7. CLINICAL ANATOMY
1. Uterine (Fibroid) Leiomyoma
The most common benign tumour in women. Arises from smooth muscle of the myometrium. Based on location: submucosal (projects into cavity → menorrhagia), intramural (within myometrium), or subserosal (projects outward). Presents with menorrhagia, dysmenorrhoea, or pressure symptoms.
2. Cancer of the Cervix (Carcinoma Cervicis)
- Squamous cell carcinoma arises at the squamocolumnar junction (transformation zone) of the cervix.
- Associated with HPV types 16 and 18.
- Pap smear (cervical cytology) screens for precancerous changes.
- Spreads directly to parametrium, bladder, rectum, and lymphatically to external and internal iliac nodes.
3. Cancer of the Uterine Body (Endometrial Carcinoma)
- Most common gynaecological malignancy in developed countries.
- Presents with postmenopausal bleeding.
- Spreads lymphatically to para-aortic nodes.
4. Uterine Prolapse
Caused by weakness/damage to the supports - particularly the transverse cervical ligaments, pelvic floor, and perineal body (often from childbirth trauma). The uterus descends into or outside the vagina.
- Grade I: cervix within vagina
- Grade II: cervix at introitus
- Grade III (Procidentia): complete prolapse outside vagina
5. Retroversion of the Uterus
In about 20% of women the uterus is retroverted (tilted backward). Usually asymptomatic. Can cause dyspareunia. A retroverted gravid uterus may become incarcerated in the pelvis.
6. Hysterectomy - Danger of Ureteric Injury
During hysterectomy (especially during ligation of the uterine artery), the ureter is at risk of being ligated, cut, or crushed, as it passes only ~2 cm lateral to the cervix, beneath the uterine artery. The surgical principle "water under the bridge" reminds the surgeon to identify the ureter before ligating the uterine artery.
7. Ectopic Pregnancy
Although not in the uterus itself, a failed uterine implantation results in tubal (98%) or other ectopic implantation. The uterus may be slightly enlarged (from decidual change) even in ectopic pregnancy, which can mislead on examination.
8. Pouch of Douglas
The deepest recess of the female peritoneal cavity. Pathological fluid (blood from ruptured ectopic pregnancy or ovarian cyst, pus from PID, ascitic fluid, malignant cells) collects here. It can be accessed by culdocentesis (needle aspiration through the posterior vaginal fornix). It is also palpable on rectal examination.
9. Lower Uterine Segment
The isthmus expands during pregnancy to form the lower uterine segment (LUS), which is thin and relatively avascular. Lower segment caesarean section (LSCS) is performed through the LUS because it heals better and has less risk of rupture in subsequent pregnancies compared to classical (upper segment) caesarean section.
References: Color Atlas of Human Anatomy Vol. 2, Internal Organs (Thieme) pp. 453-460 | Gray's Anatomy for Students pp. 554-555 | Campbell-Walsh Urology
Adductor canal
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
I now have all the information needed for a thorough answer. Let me compile it.
THE ADDUCTOR CANAL
(Also called: Hunter's Canal | Subsartorial Canal | Crural Canal)
Sources: Thieme Atlas of General Anatomy & Musculoskeletal System | Fischer's Mastery of Surgery | Imaging Anatomy Vol. 3 | Barash Clinical Anesthesia
Definition
The adductor canal is an aponeurotic intermuscular tunnel in the middle third of the medial thigh. It transmits the femoral vessels (and related nerves) from the apex of the femoral triangle above, to the adductor hiatus below, where the femoral artery becomes the popliteal artery.
- Length: approximately 15 cm
- Shape: triangular in cross-section
- Eponym: named after John Hunter (Scottish surgeon, 18th century) who ligated the femoral artery within it to treat popliteal aneurysm
Location / Extent
| Above (upper opening / inlet) | Apex of the femoral triangle - where the sartorius muscle crosses over the adductor longus |
| Below (lower opening / outlet) | Adductor hiatus - a gap in the distal attachment of the adductor magnus muscle |
The canal lies deep to the sartorius muscle in the medial aspect of the anterior compartment of the thigh.
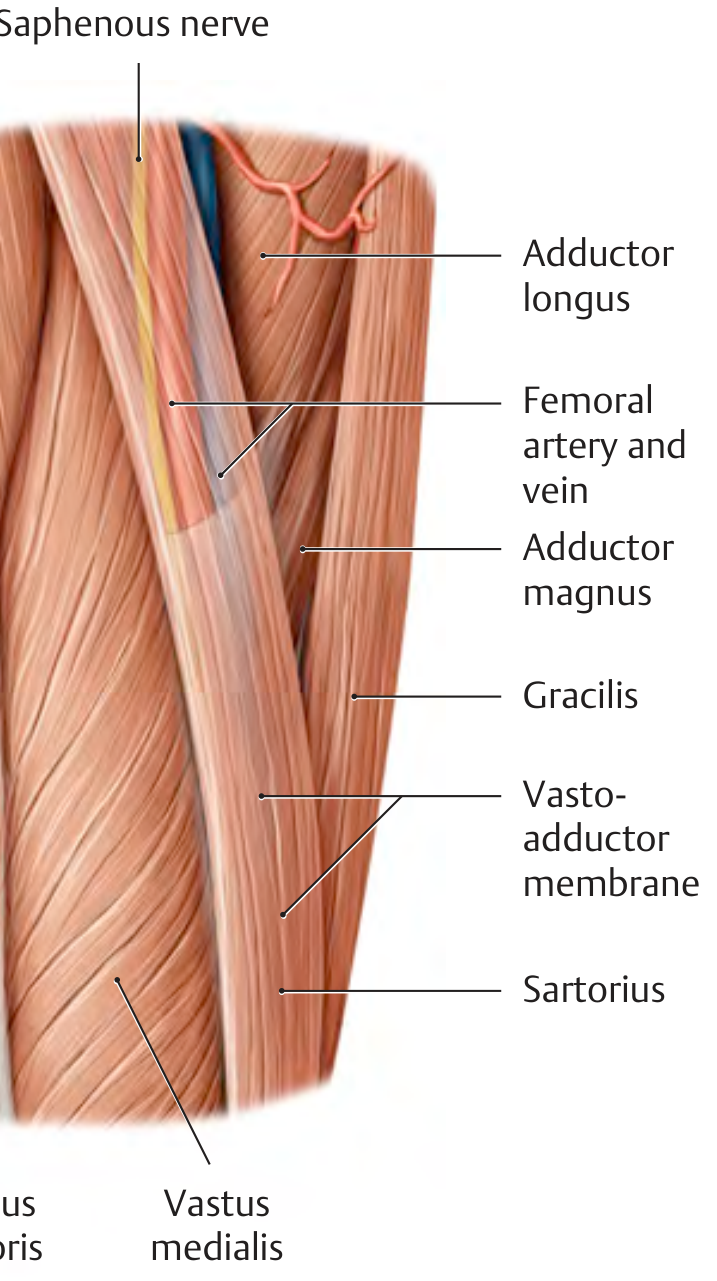
Boundaries
The canal is triangular in cross-section with four walls:
| Wall | Structure |
|---|---|
| Anterior wall (roof) | Sartorius muscle (superficial); Vastoadductor membrane (deep to sartorius) |
| Antero-lateral wall | Vastus medialis muscle |
| Postero-medial wall | Adductor longus (upper part) and adductor magnus (lower part) |
The Vastoadductor Membrane
A key anatomical feature of the canal. It is a fibrous aponeurotic sheet (~7 cm long, 2 cm at its base) that:
- Bridges between the medial edge of vastus medialis and the lateral edge of adductor magnus (and its distal tendon)
- Is a continuation of the medial intermuscular septum
- Forms the actual "roof" of the canal (sartorius is superficial to it)
- Is pierced by the saphenous nerve and the descending genicular artery as they leave the canal
Contents
The canal contains (from anterior to posterior, laterally to medially):
| Structure | Notes |
|---|---|
| Femoral artery | Also called superficial femoral artery (SFA) in imaging/vascular surgery; lies anterior in the canal |
| Femoral vein | Posterior to the artery at the hiatus; changes to medial in the upper canal |
| Saphenous nerve | Branch of the femoral nerve (L3, L4); the largest purely sensory nerve of the lower limb. Enters the canal with the vessels but exits by piercing the vastoadductor membrane in the lower part of the canal (does NOT pass through the adductor hiatus). Becomes superficial between sartorius and gracilis to supply the medial side of the knee, leg, and foot |
| Descending genicular artery | A branch of the femoral artery that exits through the vastoadductor membrane alongside the saphenous nerve to supply the knee joint |
| Nerve to vastus medialis | Branch of the femoral nerve; present in the upper canal (separated from the main bundle by a fascial layer) |
Memory aid: "FVS" - Femoral artery, Vein, Saphenous nerve (from lateral to medial)
Adductor Hiatus
The lower opening of the canal. It is a gap in the tendinous insertion of adductor magnus (between its adductor and hamstring parts). Through the hiatus:
- Femoral artery passes posteriorly → becomes the popliteal artery
- Femoral vein passes anteriorly (ascending from popliteal fossa)
- The saphenous nerve does NOT pass through - it exits via the vastoadductor membrane more proximally
Relations
- Superficial: Sartorius muscle, deep fascia of thigh, skin
- Deep: Femur (lower shaft)
- Lateral: Vastus medialis
- Medial: Adductor longus, adductor magnus, gracilis
Clinical Anatomy
1. Hunter's Operation (Historical)
John Hunter ligated the femoral artery within the canal to treat popliteal aneurysm - taking advantage of the collateral circulation around the knee. This avoided the more dangerous ligation at the femoral triangle.
2. Femoral Artery Occlusion (PAD)
The femoral artery is a common site of atherosclerotic occlusion (superficial femoral artery, within the adductor canal). The vessel's path through the canal makes it prone to kinking and turbulent flow. Presents as intermittent claudication of the calf. Treated by angioplasty, stenting, or femoro-popliteal bypass.
3. Compression of Femoral Artery at Adductor Hiatus
In young athletes, compression of the femoral artery at the adductor hiatus or by an overlying vastoadductor membrane following exercise is a recognised condition causing exertional leg pain simulating vascular disease.
4. Saphenous Nerve Entrapment
The saphenous nerve is most susceptible to entrapment at two points:
- Within the adductor canal (compression by fibrous bands)
- At the point where it pierces the vastoadductor membrane
Presents as medial knee/leg pain (burning, paraesthesia), simulating a vascular disorder. Often misdiagnosed. In one-third of cases, branches to the medial thigh skin also pierce the membrane.
5. Adductor Canal Block (ACB)
A peripheral nerve block used for postoperative analgesia after knee surgery (especially total knee arthroplasty). Local anaesthetic is injected into the canal under ultrasound guidance, targeting the saphenous nerve and nerves to the knee joint. Key advantage over femoral nerve block: it spares quadriceps motor function (because the nerve to vastus medialis lies in a separate fascial layer), allowing earlier mobilisation. The canal is identified on ultrasound by visualising the femoral artery (SFA) deep to the sartorius, with adductor magnus posteriorly.
6. Access for Femoro-Popliteal Bypass
The adductor canal provides surgical access to the superficial femoral artery for femoro-popliteal bypass grafting. The incision is made along the medial thigh, sartorius is retracted, and the SFA is approached through the vastoadductor membrane.
7. Saphenous Vein Harvest
The great saphenous vein runs just superficial to the canal (subcutaneous, medial thigh). It is harvested here for coronary artery bypass grafting - care must be taken not to damage the saphenous nerve which accompanies it distally.
Summary Table
| Feature | Detail |
|---|---|
| Location | Middle third of medial thigh |
| Extent | Apex of femoral triangle → Adductor hiatus |
| Roof | Sartorius + Vastoadductor membrane |
| Anterior wall | Vastus medialis |
| Posterior wall | Adductor longus + Adductor magnus |
| Contents | Femoral artery, femoral vein, saphenous nerve, descending genicular artery, nerve to vastus medialis |
| Lower outlet | Adductor hiatus (femoral artery → popliteal artery) |
| Saphenous nerve exit | Pierces vastoadductor membrane (does NOT go through hiatus) |
| Clinical importance | SFA disease, saphenous nerve entrapment, adductor canal block |
References: Thieme Atlas of General Anatomy & Musculoskeletal System, pp. 575-576 | Fischer's Mastery of Surgery, 8e, pp. 6721-6722 | Imaging Anatomy Vol. 3, p. 435
Ischiorectal fossa and its applied anatomy
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Loading Image
I now have all the material for a comprehensive answer. Let me compile it.
ISCHIORECTAL (ISCHIOANAL) FOSSA & APPLIED ANATOMY
Nomenclature note: The term ischiorectal fossa is the classical and still widely used name in clinical and surgical literature. Modern Terminologia Anatomica renames it the ischioanal fossa because it is related more directly to the anal canal than to the rectum. Both terms are acceptable in examinations.
Sources: Color Atlas of Human Anatomy Vol. 2 (Thieme) | Thieme Atlas of General Anatomy | Campbell-Walsh Urology | Bailey & Love's Surgery | Sabiston Textbook of Surgery
Definition
The ischiorectal (ischioanal) fossa is a wedge-shaped (pyramidal) fat-filled space situated on either side of the anal canal in the anal triangle of the perineum, lateral to the pelvic floor. It lies between the skin of the buttock below and the pelvic diaphragm above.
Shape
- Pyramidal / wedge-shaped
- The apex (tip of the pyramid) points upward toward the union of levator ani and obturator internus fascia
- The base faces inferiorly and is covered by perineal skin
- The anterior angle (anterior recess) extends forward above the urogenital diaphragm into the anterior part of the perineum
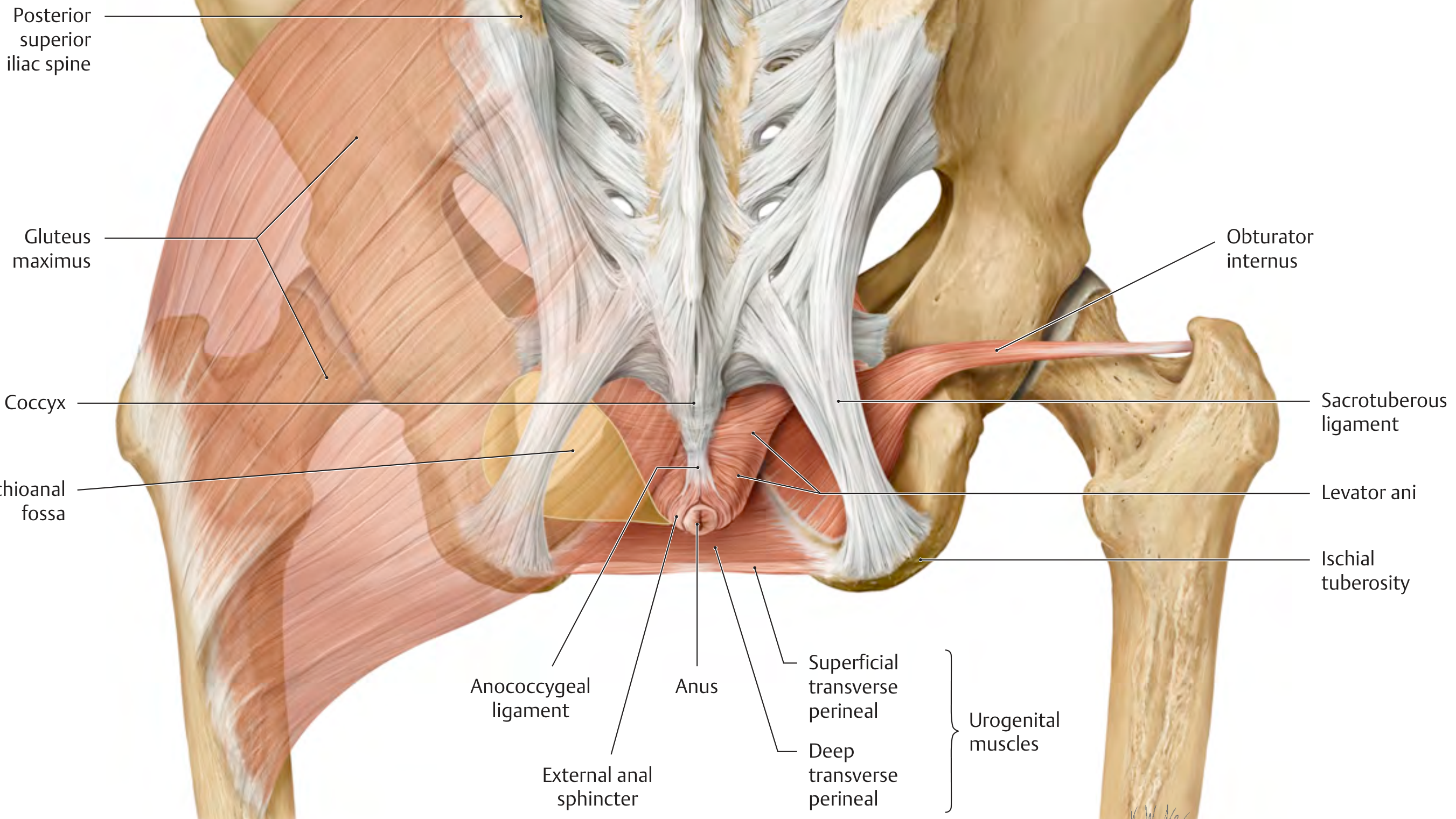
Boundaries
| Wall | Structure |
|---|---|
| Medial wall (superomedial) | Levator ani (and its inferior fascia - the inferior fascia of the pelvic diaphragm); External anal sphincter below |
| Lateral wall | Obturator internus muscle covered by its fascia (obturator fascia); ischial tuberosity |
| Roof (apex) | Junction of levator ani and obturator internus - the tendinous arch of levator ani |
| Floor (base) | Perineal skin and superficial fascia |
| Posterior boundary | Gluteus maximus muscle and sacrotuberous ligament |
| Anterior boundary | Posterior border of the urogenital diaphragm (perineal membrane); the space continues as the anterior recess above the urogenital diaphragm |
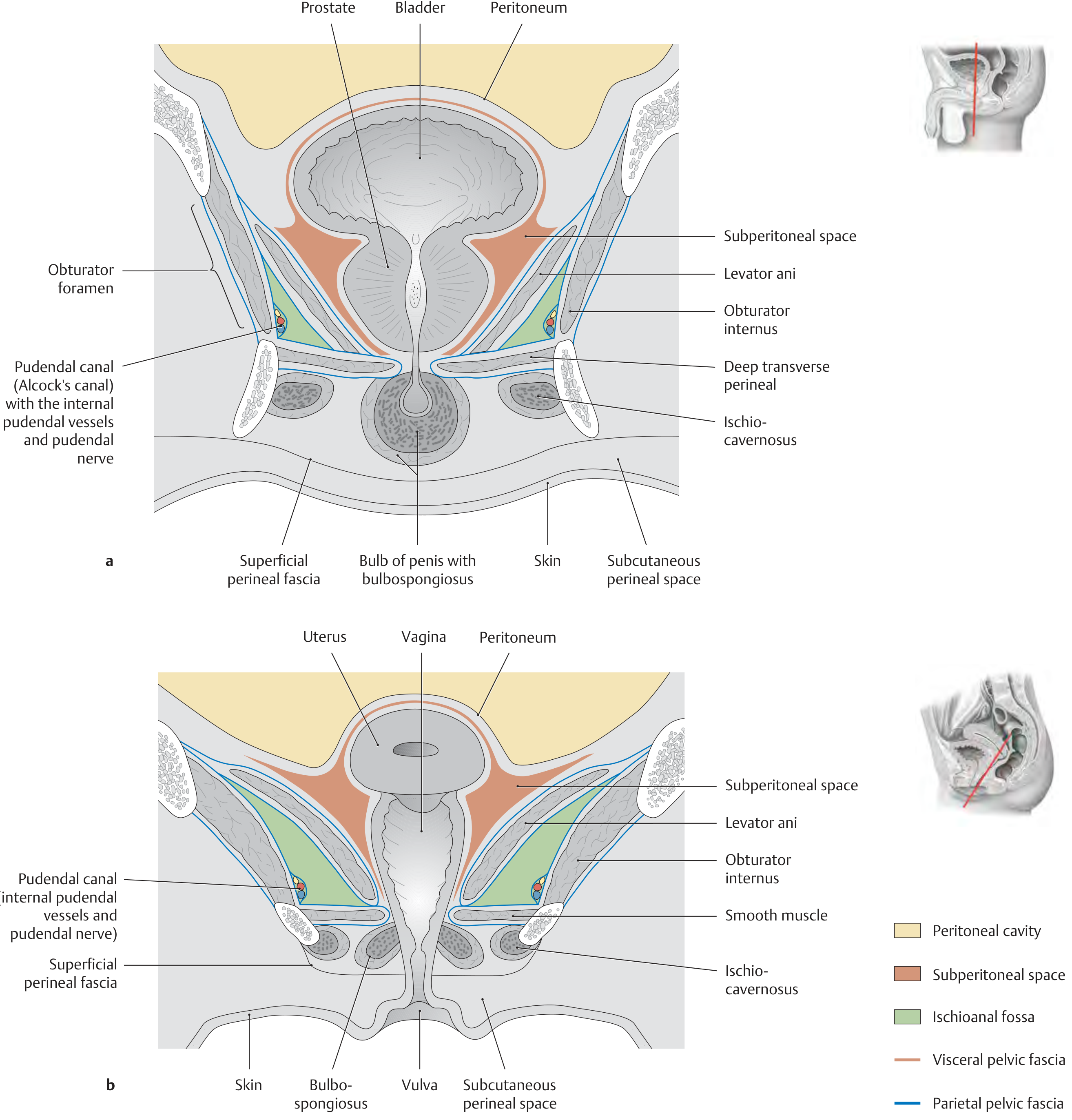
Contents
1. Fat Body of the Ischioanal Fossa
- The fossa is largely filled with a mass of fatty fibroaereolar tissue (the ischioanal fat pad)
- This fat pad is mobile - it can slide downward and backward during defecation and labour, allowing expansion of the anal canal
- It is traversed by the branches of the pudendal nerve and internal pudendal vessels
2. Pudendal Canal (Alcock's Canal)
- A fascial tunnel (a split in the obturator fascia) on the lateral wall of the fossa
- Runs from just below the ischial spine, forward along the lateral wall, toward the posterior border of the urogenital diaphragm
- Contents: Internal pudendal artery and vein, Pudendal nerve (S2, S3, S4)
3. Inferior Rectal (Haemorrhoidal) Nerve and Vessels
- Inferior rectal artery - branch of the internal pudendal artery; exits the pudendal canal, crosses the ischioanal fat body to reach the external anal sphincter and perianal skin
- Inferior rectal veins - drain to the internal pudendal veins and ultimately to the internal iliac veins
- Inferior rectal nerve - branch of the pudendal nerve; supplies the external anal sphincter (motor) and perianal skin (sensory)
4. Perineal Branch of S4 Spinal Nerve
- Crosses the fossa to supply the external anal sphincter and perianal skin
5. Lymphatics
- Drain to the superficial inguinal lymph nodes
Pudendal Nerve and Internal Pudendal Artery - Course Through the Fossa
The pudendal nerve (S2, S3, S4) and internal pudendal artery leave the pelvis through the greater sciatic foramen (below piriformis), hook around the ischial spine/sacrospinous ligament, and re-enter the perineum through the lesser sciatic foramen - entering the pudendal canal on the lateral wall of the ischioanal fossa.
Within the canal, the pudendal nerve gives off (in sequence):
- Inferior rectal nerve - crosses the fossa to the external anal sphincter
- Perineal nerve - supplies muscles and skin of the urogenital triangle
- Dorsal nerve of penis/clitoris - terminal branch
Communication / Extensions
The ischioanal fossae of the two sides are separate from each other in front of the anal canal, but communicate behind the anal canal through the deep postanal space (between the anococcygeal body/ligament and the external anal sphincter). This communication is of critical surgical significance (see horseshoe abscess, below).
Each fossa also has an anterior recess that extends forward above the posterior border of the urogenital diaphragm.
The fossa communicates posteriorly with the pelvic cavity through the greater and lesser sciatic foramina, which is why pelvic infections can spread to the perineum and vice versa.
Applied / Clinical Anatomy
1. Ischiorectal (Perianal) Abscess
The most common perianal abscess. Arises from infection of anal glands (cryptoglandular origin) at the dentate line, spreading into the intersphincteric space and then into the ischiorectal fossa.
Clinical features:
- Severe, throbbing, constant perianal pain
- Tender, erythematous, fluctuant swelling lateral to the anus
- Fever and systemic sepsis if neglected
Types of anorectal abscess (Park's classification by anatomical space):
| Type | Location | % |
|---|---|---|
| Perianal | Subcutaneous, adjacent to anal verge | ~40% |
| Ischiorectal | Within the ischiorectal fat body | ~20-25% |
| Intersphincteric | Between internal and external sphincters | ~20-25% |
| Supraelevator | Above the levator ani | ~5% |
Treatment: Prompt incision and drainage as close to the anus as possible (to shorten any subsequent fistula tract). Cruciate incision. CT pelvis if diagnosis uncertain.
2. Horseshoe Abscess
A horseshoe abscess arises when an ischiorectal abscess tracks posteriorly through the deep postanal space (behind the anal canal) and extends into the contralateral ischiorectal fossa - forming a U-shaped (horseshoe) collection.
Internal opening is typically at the posterior midline of the anal canal.
Treatment (Modified Hanley procedure):
- Posterior midline drainage of the deep postanal space (incising the anococcygeal ligament)
- Counterincisions over each ischiorectal fossa
- Seton placement for the posterior midline fistula tract
- Penrose drains connecting the incisions
3. Anal Fistula (Fistula-in-Ano)
Infection originating in the ischiorectal fossa frequently results in a fistula-in-ano after spontaneous or surgical drainage. The track of the fistula relative to the sphincter complex determines Parks' classification:
| Type | Course | % |
|---|---|---|
| Intersphincteric | Between internal and external sphincters to perianal skin | ~45% |
| Transsphincteric | Through both sphincters, traversing the ischiorectal fossa, to skin of buttock | ~30% |
| Suprasphincteric | Up through intersphincteric plane, over puborectalis, down through ischiorectal fossa to skin | ~20% |
| Extrasphincteric | From high rectum to perianal skin, completely outside sphincters | ~5% |
Goodsall's Rule: Fistulae with external openings posterior to a transverse line through the anus have a curved tract with an internal opening at the posterior midline. Fistulae with external openings anterior to this line have a straight radial tract to the nearest crypt.
4. Pudendal Nerve Block
The pudendal nerve is blocked at the ischial spine (where it enters the pudendal canal), either transvaginally (in obstetrics) or transperineally. This provides analgesia for:
- Episiotomy repair
- Instrumental (forceps/vacuum) delivery
- Perineal procedures
Landmark: the ischial spine, palpated transvaginally. Local anaesthetic is injected just medial and posterior to the ischial spine.
5. Fournier's Gangrene (Necrotising Fasciitis of the Perineum)
A life-threatening polymicrobial necrotising fasciitis spreading through the perineal fascial spaces including the ischiorectal fossa. The loose fat in the fossa offers little resistance to spread. Treatment is aggressive surgical debridement, broad-spectrum antibiotics, and often hyperbaric oxygen.
6. Spread of Pelvic Infections
Because the ischioanal fossa communicates with the pelvic cavity through the sciatic foramina, pelvic abscesses (e.g., supraelevator abscess from pelvic inflammatory disease or Crohn's disease) can track downward into the ischiorectal fossa and present as a perianal swelling. Understanding the origin is critical to correct surgical drainage:
- Supraelevator abscess from upward extension of an ischiorectal abscess → drain through the ischiorectal fossa
- Supraelevator abscess from an intersphincteric source → drain transrectally (NOT through the ischiorectal fossa, as this would create a suprasphincteric fistula)
7. Pudendal Nerve Injury
During vaginal delivery, the pudendal nerve traversing the lateral wall of the ischiorectal fossa can be stretched or compressed against the ischial spine by the descending fetal head. This may result in:
- Faecal incontinence (damage to external anal sphincter innervation)
- Urinary incontinence (damage to external urethral sphincter innervation)
- Perineal numbness / dyspareunia
Summary Table
| Feature | Detail |
|---|---|
| Shape | Pyramidal (wedge-shaped), apex upward |
| Medial wall | Levator ani + external anal sphincter |
| Lateral wall | Obturator internus + obturator fascia |
| Posterior boundary | Gluteus maximus + sacrotuberous ligament |
| Anterior | Urogenital diaphragm (anterior recess above it) |
| Filled with | Fat body (ischioanal fat pad) |
| Neurovascular sheath in lateral wall | Pudendal canal (Alcock's canal) containing internal pudendal vessels + pudendal nerve |
| Key nerve crossing fossa | Inferior rectal nerve |
| Communication between two fossae | Deep postanal space (behind anal canal) |
| Key clinical importance | Ischiorectal abscess, horseshoe abscess, anal fistula, pudendal nerve block |
References: Color Atlas of Human Anatomy Vol. 2 pp. 476-477 | Thieme Atlas of General Anatomy pp. 580-583 | Campbell-Walsh Urology, Ch. 109 | Sabiston Textbook of Surgery, Ch. 97 | Bailey & Love's Surgery, Ch. 75
This is a shared conversation. Sign in to Orris to start your own chat.