Management of rheumatoid arthritis
"rheumatoid arthritis"[MeSH Terms] AND "therapeutics"[MeSH Terms]
"rheumatoid arthritis" AND "treatment"
Management of Rheumatoid Arthritis
Overview and Goals of Therapy
- RA can and should be diagnosed early; DMARD therapy should be initiated at the time of diagnosis
- Treatment should follow a treat-to-target (T2T) strategy - either remission or low disease activity
- The cornerstone of therapy for most patients is methotrexate (MTX)
- Over 20 DMARDs are now available, including biosimilar biologics
- All DMARDs, especially biologics, are more effective when administered with MTX
- Comorbidities - particularly cardiovascular disease - must always be addressed aggressively
Treat-to-Target (T2T) Strategy
- 71% of subjects in the intensive group achieved ACR70 improvement vs. 18% in routine care (p < 0.0001)
- Significantly less radiographic progression (median erosion score 0.5 vs. 3.0; p = 0.002)
- No increase in adverse events
- Achieved using conventional DMARDs alone
| Instrument | Remission | Low Activity | Moderate | High |
|---|---|---|---|---|
| DAS28 | ≤2.6 | ≤3.2 | >3.2 to ≤5.1 | >5.1 |
| SDAI | ≤3.3 | ≤11 | >11 to ≤26 | >26 |
| CDAI | ≤2.8 | ≤10 | >10 to ≤22 | >22 |
Medical Therapy: Three Pillars
1. NSAIDs
- COX-2 inhibitors (e.g., celecoxib) are less likely to cause GI bleeding; celecoxib was non-inferior to naproxen/ibuprofen for cardiovascular outcomes in an RCT
- Concomitant proton pump inhibitor (PPI) should be considered for all RA patients on NSAIDs
- NSAIDs raise blood pressure and reduce renal blood flow - monitor accordingly
- Once DMARDs achieve adequate disease control, NSAIDs should be discontinued
2. Glucocorticoids
- 25% increased risk of serious infection at doses as low as 5 mg/day
- Doubling of infection risk at 5-10 mg/day
- Bridge therapy only - to control inflammation while slower-acting DMARDs begin working
- Prednisone should rarely exceed 10 mg/day for articular manifestations
- Taper to the lowest effective dose; "the best dose of glucocorticoids for chronic use is zero"
- Intramuscular depot injections for DMARD escalation bridging
- Intra-articular injections useful for individual joint flares; ultrasound guidance for difficult joints
- Higher doses may be needed for extra-articular manifestations (vasculitis, scleritis)
3. Disease-Modifying Antirheumatic Drugs (DMARDs)
Conventional Synthetic DMARDs (csDMARDs)
| Drug | Dose | Key Points |
|---|---|---|
| Methotrexate (first-line) | 7.5-25 mg weekly (oral or SC) | Cornerstone; more effective SC; co-administer folic acid; monitor LFTs, CBC |
| Hydroxychloroquine | 200-400 mg/day (5 mg/kg) | Least toxicity; no blood monitoring needed; yearly ophthalmology after 5 yrs; lowers cholesterol; reduces diabetes risk |
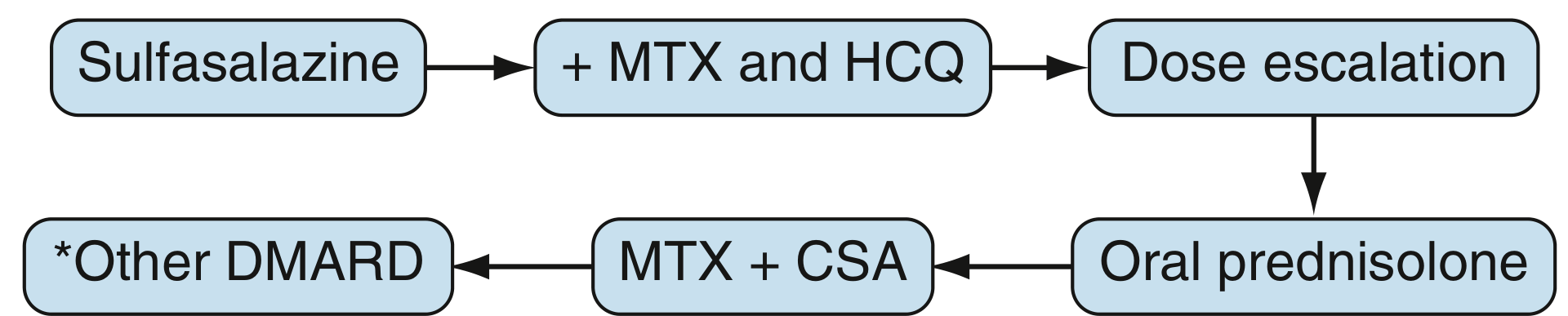
| Sulfasalazine | 500 mg-3 g/day | Monitor WBC first 6 months; frequently combined with MTX + HCQ ("triple therapy") |
| Leflunomide | 10-20 mg/day | Pyrimidine antagonist; very long half-life; teratogenic - check blood levels before pregnancy; washout with cholestyramine |
| Azathioprine | 1-2.5 mg/kg/day | Monitor CBC and LFTs |
| Minocycline | 100 mg twice daily | Effective in early RF-positive RA; chronic use can cause skin hyperpigmentation; risk of drug-induced lupus |
Biologic DMARDs (bDMARDs)
- Etanercept - soluble TNF receptor fusion protein
- Infliximab - chimeric monoclonal antibody; IV infusion
- Adalimumab - fully human mAb; SC injection
- Golimumab - SC or IV monthly
- Certolizumab pegol - PEGylated Fab fragment; no Fc region (useful in pregnancy)
- Tocilizumab (IL-6R inhibitor) - early treatment with tocilizumab + MTX results in greater sustainable clinical, functional, and radiographic outcomes than MTX alone; appears superior to rituximab; causes a rise in serum cholesterol
- Sarilumab (IL-6R inhibitor)
- Abatacept (CTLA4-Ig) - blocks CD80/86 co-stimulation (second signal for T-cell activation)
- Rituximab (anti-CD20) - depletes B cells; preferred in patients with prior malignancy; used if TNF inhibitor fails
Targeted Synthetic DMARDs (tsDMARDs) - JAK Inhibitors
| Drug | Dose | Notes |
|---|---|---|
| Tofacitinib | 5 mg twice daily | Effective as initial DMARD therapy combined with MTX; also works in TNF-inhibitor failures; monitor CBC, LFTs |
| Baricitinib | 2-4 mg once daily | Superior to adalimumab in MTX-inadequate responders in head-to-head trial |
| Upadacitinib | 15 mg once daily | Relatively JAK1-selective; effective as monotherapy or add-on |
| Filgotinib | 100-200 mg once daily | Effective in DMARD-inadequate responders |
Treatment Algorithm (EULAR 2019 Framework)
Step 1: Diagnosis confirmed → Start csDMARD immediately
↓ MTX (first choice) ± short-term bridging glucocorticoid
Step 2: Reassess at 3 months; if <50% improvement or target not met by 6 months
↓ Modify therapy (change or add csDMARD; consider triple therapy)
Step 3: csDMARD failure (poor prognosis factors* or refractory)
↓ Add bDMARD (TNF inhibitor preferred) or tsDMARD (JAK inhibitor)
Always combine with MTX where possible
Step 4: First bDMARD failure
↓ Switch to another bDMARD (different mechanism) or JAK inhibitor
After JAK inhibitor failure: switch to bDMARD
After IL-6 inhibitor failure: switch to non-IL-6 bDMARD
Step 5: Sustained remission (≥6 months)
↓ Consider DMARD tapering (reduce dose/frequency; rarely discontinue entirely)
DMARD Tapering
- Reduce frequency (dose spacing) rather than abrupt discontinuation
- Remain on at least one DMARD
- Seronegative RA patients and those on combination therapy are better tapering candidates
- Stopping is associated with high flare rates; most patients can recapture their good state upon restarting the same bDMARD/tsDMARD
Surgical Management
- Synovectomy (arthroscopic or open) - for persistent synovitis unresponsive to medical treatment
- Tenosynovectomy and tendon repair/realignment - especially in the hand and wrist
- Arthroplasty (joint replacement) - most commonly hip, knee, and MCP joints; for severe joint destruction
- Arthrodesis (joint fusion) - for painful, unstable joints when arthroplasty is not suitable
Non-Pharmacological Management
- Physical therapy - range-of-motion exercises, strengthening, aerobic conditioning
- Occupational therapy - joint protection techniques, assistive devices, splinting
- Warmth and activity - relieves morning stiffness
- Patient education - disease understanding, treatment adherence, self-management
Managing Comorbidities
| Comorbidity | Management |
|---|---|
| Cardiovascular disease (leading cause of excess mortality) | Methotrexate, TNF inhibitors reduce CV mortality; aggressively treat lipids, hypertension, diabetes |
| Osteoporosis | Calcium, vitamin D supplementation; bisphosphonates; DXA monitoring (especially with glucocorticoid use) |
| Infections | Pneumococcal vaccine, annual influenza vaccination, zoster vaccine; caution with biologic/JAK inhibitor therapy |
| Malignancy | Increased lymphoma risk; decreased colon cancer risk (chronic NSAID use); monitor |
| Felty syndrome (RA + splenomegaly + neutropenia) | Treat underlying RA; splenectomy only for severe neutropenia (<500 cells/μL) with recurrent infections |
Prognosis
- RF and/or anti-CCP positivity
- Shared epitope (HLA-DRB1) positivity
- Radiographic erosions (usually occur within first 1-2 years)
- High baseline disease activity
- Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set - Chapter 73 (Treatment Overview, Treat-to-Target)
- Goldman-Cecil Medicine International Edition, 2-Volume Set - Chapter 243 (Medical Therapy)
- Rheumatology, 2-Volume Set (Elsevier, 2022) - Methotrexate and combination therapy
Search for latest 2025-2026 clinical guidelines on RA remission targets
"rheumatoid arthritis"[MeSH Terms] AND "remission"[MeSH Terms] AND "guideline"
ACR EULAR 2025 2026 rheumatoid arthritis remission targets clinical guidelines
PMID: 41826212
https://rheumnow.com/news/2025-update-eular-recommendations-…
EULAR 2025 RA recommendations 9 recommendations full list JAK inhibitor safety remission tapering changes from 2022
"rheumatoid arthritis" AND "treat to target" AND "remission"
https://www.guidelinecentral.com/insights/apr-2026-eular-man…
PMID: 38796922
EULAR 2025 Update: Clinical Guidelines on RA Remission Targets
What Changed: 2022 vs. 2025 Update at a Glance
| Feature | 2022 Version | 2025 Update |
|---|---|---|
| Number of recommendations | 11 | 9 (merged/removed) |
| DMARD initiation | Start immediately at diagnosis | Unchanged |
| Remission target | Remission or LDA in all patients | Unchanged |
| First csDMARD failure (no poor prognosis) | Try another csDMARD | Unchanged |
| First csDMARD failure (poor prognosis) | Add bDMARD; JAKi may be considered with risk assessment | Simplified: Add bDMARD; JAKi may be considered with risk assessment (merged into single recommendation) |
| JAK inhibitor positioning | Second-line, after csDMARD failure | Cautious positioning retained - explicit risk checklist added (age >65, MACE, VTE, malignancy) |
| Sustained remission + tapering | After GC discontinuation, DMARD dose reduction may be considered | After GC discontinuation, DMARD continuation is recommended; dose reduction may still be considered - shift to preserve therapy over stopping |
5 Overarching Principles (Unchanged from 2022)
- Rheumatologists are the specialists who should primarily care for people with RA
- Best possible care requires shared decision-making based on disease activity, safety, comorbidities, and structural damage
- Multiple drugs with different modes of action are available; patients may require multiple successive therapies throughout their life
- Societal and individual cost of RA is high and must be factored into management decisions
- RA management requires ongoing collaboration between the patient and the healthcare team
The 9 Recommendations (2025 Update)
Recommendation 1 - Start DMARDs Immediately
Recommendation 2 - Treat-to-Target (Remission or LDA)
- Remission is the primary target, especially in early disease
- Low disease activity (LDA) is an acceptable alternative for patients with long-standing disease who have failed one or more DMARDs
- Any state other than LDA should be regarded as unacceptable
Recommendation 3 - Monitoring Frequency
- Active disease: monitor every 1-3 months
- If no improvement by 3 months after treatment start, or target not reached by 6 months, adjust therapy
- Once target is sustained, monitoring frequency can be reduced to every 3-6 months
Recommendation 4 - MTX First
- If MTX is contraindicated or poorly tolerated early: use leflunomide or sulfasalazine
- MTX ideally combined with short-term bridging glucocorticoids
Recommendation 5 - Glucocorticoids as Bridge
- Taper and discontinue as rapidly as clinically feasible
- Goal: GC-free disease control
Recommendation 6 - Escalation After csDMARD Failure
- Without poor prognostic factors: consider other csDMARDs (e.g., triple therapy: MTX + SSZ + HCQ)
- With poor prognostic factors*: add a bDMARD; a JAK inhibitor may also be considered, but pertinent risk factors must be taken into account
Recommendation 7 - bDMARD/tsDMARD Failure and Sequencing
- Switch to any other bDMARD (from the same or a different class)
- A JAKi may be considered, but with careful risk assessment (MACEs, malignancies, VTE)
- TNF inhibitors (adalimumab, certolizumab, etanercept, golimumab, infliximab + biosimilars), abatacept, rituximab, tocilizumab, sarilumab are all options
- JAKi: tofacitinib, baricitinib, filgotinib, upadacitinib
Recommendation 8 - JAK Inhibitor Risk Stratification (Major 2025 Change)
- Age >65 years
- Smoking history / current smoker
- Pre-existing cardiovascular disease or risk factors
- History of venous thromboembolism (VTE)
- Personal or family history of malignancy
Recommendation 9 - Tapering in Sustained Remission (Key Change)
- DMARD continuation is now recommended (upgraded from "may be considered" in 2022)
- Dose reduction may still be considered cautiously
- Complete stopping is strongly discouraged - most patients flare upon discontinuation, especially those on bDMARDs and JAKi
- If tapering is attempted: reduce dose/frequency gradually; restore promptly if disease resurfaces
"A cure for RA is still rare, and for most patients stopping treatment altogether leads to the disease flaring, especially for patients on biologic or JAK inhibitor therapies." - Christopher Edwards, EULAR Task Force Co-Convenor
Remission Definitions Still in Use (ACR/EULAR)
| Score | Remission Threshold |
|---|---|
| DAS28 | ≤2.6 |
| SDAI | ≤3.3 |
| CDAI | ≤2.8 |
| Boolean 2.0 | TJC28 ≤1, SJC28 ≤1, CRP ≤1 mg/dL, PtGA ≤2 (0-10) |
Supporting Evidence: Treat-to-Target Meta-Analysis
- T2T patients were 68% more likely to achieve remission vs. usual care (pooled RR 1.68, 95% CI 1.47-1.92; p<0.001)
- Significant improvement in DAS-28 response (pooled SMD 0.47; p<0.001)
- Better HAQ/physical function outcomes (pooled SMD 1.48; p=0.004)
- No increase in adverse events vs. usual care
- T2T strategies with a predefined treatment protocol performed better than those without
July 2026 Update: Elderly-Onset RA
Summary: What Clinicians Should Apply Now
- Start DMARDs at diagnosis - no watchful waiting
- Target remission for all patients; LDA acceptable if remission is unachievable
- Review at 3 months - if <50% improvement, escalate; target must be met by 6 months
- MTX is still the anchor drug - optimise dose (up to 25 mg/week SC) with folic acid
- Bridge with short-term glucocorticoids - never long-term
- Escalate to bDMARD (preferred) or JAKi after csDMARD failure in high-risk patients
- Risk-stratify before prescribing JAKi - ORAL Surveillance data demands this
- In remission: continue DMARDs - do not stop; dose reduction is cautious, not cessation
- Monitor less frequently once stable, but never abandon surveillance
Management of autoimmune hemolytic anemia
"autoimmune hemolytic anemia"[MeSH Terms] AND "therapy"[MeSH Terms]
"autoimmune hemolytic anemia" AND "rituximab OR splenectomy OR complement"
PMID: 41347987
PMID: 41348049
Management of Autoimmune Hemolytic Anemia (AIHA)
Overview and Classification
| Type | Frequency | Antibody | Optimal Temp | Site of Hemolysis | DAT Pattern |
|---|---|---|---|---|---|
| Warm AIHA (wAIHA) | 60-80% | IgG (mainly IgG1) | 37°C | Spleen (extravascular) | IgG+ and/or C3+ |
| Cold agglutinin disease (CAD) | 15-25% | IgM | <30°C (optimum 4°C) | Liver (extravascular) | IgG-, C3+ |
| Mixed AIHA | ~5% | IgG + IgM | 4-37°C (wide thermal amplitude) | Both | IgG+ and C3+ |
| Paroxysmal cold hemoglobinuria (PCH) | Rare (mostly children) | IgG (Donath-Landsteiner) | 2-10°C | Intravascular | C3+ only |
- Lymphoproliferative disorders (CLL, lymphoma, Hodgkin's)
- Systemic autoimmune diseases (SLE, rheumatoid arthritis)
- Infections (EBV, Mycoplasma pneumoniae - especially CAD)
- Drugs (fludarabine, checkpoint inhibitors - anti-PD1, anti-CTLA4, etc.)
- Hematopoietic stem cell transplantation
- Congenital immunodeficiencies
A workup for underlying disease must be performed at diagnosis in every patient. A primary wAIHA can precede non-Hodgkin lymphoma by many years - patients must be followed beyond remission.
Diagnostic Confirmation
| Test | Finding in AIHA |
|---|---|
| Hemoglobin / Hematocrit | Decreased |
| Reticulocyte count | Increased (compensatory RBC production) |
| Peripheral smear | Spherocytes (extravascular hemolysis); schistocytes (intravascular) |
| LDH | Elevated |
| Haptoglobin | Decreased (especially in intravascular hemolysis) |
| Indirect (unconjugated) bilirubin | Elevated |
| Direct Antiglobulin Test (DAT / Direct Coombs) | Positive - the critical confirmatory screen |
| Urinary hemoglobinuria | Present in intravascular hemolysis |
Supportive Care (All Types)
Folic Acid
Red Blood Cell Transfusion
- Indicated for disabling anemia symptoms and/or significant cardiovascular comorbidity (e.g., coronary artery disease, heart failure)
- Target Hb ≥8 g/dL in patients with major comorbidities; younger patients may tolerate Hb as low as 6 g/dL if stable
- No patient with symptomatic AIHA should be denied transfusion due to an "incompatible crossmatch" - the positive DAT almost always interferes with compatibility testing
- Blood bank should provide the "least incompatible" packed RBCs and must be informed of the patient's status
- Monitor closely; transfusions accelerate hemolysis in AIHA
Prophylactic Anticoagulation
Recombinant Erythropoietin
Treat the Underlying Cause
Management of Warm AIHA
First-Line: Corticosteroids
- Response expected in 1-3 weeks; about 80% of patients respond initially
- Once Hb stabilizes and rises, taper gradually over 3-6 months
- Flares and relapses are common after corticosteroid withdrawal or dose reduction - they are a major feature of wAIHA
- For severe or life-threatening cases: high-dose methylprednisolone IV (e.g., 250-1000 mg/day for 3-4 days) may be used
- Long-term steroid dependence is common and problematic; transition to steroid-sparing therapy is a key management goal
IVIG (Intravenous Immunoglobulin)
- 2 g/kg IV over 2-5 days (or 400 mg/kg/day × 5 days)
- Used as adjunct to steroids in severe acute AIHA - provides faster short-term response
- Effect is transient (2-4 weeks); not a definitive therapy
- Particularly useful as bridging therapy
Plasma Exchange
- Considered for severe, life-threatening wAIHA not responding rapidly to steroids + IVIG
- Removes circulating autoantibodies temporarily
- Short-term bridge only
Second-Line: Rituximab (Preferred)
- Standard dose: 375 mg/m² IV weekly × 4 doses
- Response rate: ~75-80% in wAIHA
- Duration of response: months to years; retreatment on relapse is effective
- Advantages over splenectomy: avoids surgical risk, preserves immune function, can be repeated
- Particularly effective in secondary AIHA associated with lymphoproliferative disorders
Third-Line / Later: Splenectomy
- Removes the primary site of RBC destruction and autoantibody production in wAIHA
- Response rate ~60-70%, but relapse rates are significant
- Pre-splenectomy workup mandatory:
- Rule out antiphospholipid syndrome (especially before surgery given thrombotic risk)
- Vaccinate against encapsulated organisms: Streptococcus pneumoniae, Haemophilus influenzae, Neisseria meningitidis at least 2 weeks before surgery
- Lifelong penicillin prophylaxis post-splenectomy is recommended by some guidelines
- Reserved for fit patients who have failed steroids + rituximab
Other Immunosuppressants (Refractory / Later Lines)
| Drug | Notes |
|---|---|
| Azathioprine | 1-2.5 mg/kg/day; classic steroid-sparing agent; slow onset (3-6 months) |
| Mycophenolate mofetil | 1-1.5 g twice daily; well-tolerated steroid-sparing option |
| Cyclophosphamide | For refractory cases, especially with underlying lymphoma |
| Cyclosporine | 2.5-5 mg/kg/day; effective in refractory cases, especially in children |
| Danazol | Androgenic steroid; useful as steroid-sparing agent |
Emerging / Novel Therapies for Refractory wAIHA (2025)
- BTK inhibitors: ibrutinib, zanubrutinib, rilzabrutinib
- PI3K-delta inhibitors: parsaclisib
- Anti-CD19/BAFF: obexelimab, ianalumab, povetacicept
- Bortezomib (proteasome inhibitor)
- Daratumumab (anti-CD38)
- Fostamatinib, sovleplenib - inhibit macrophage Fc receptor-mediated phagocytosis
- Nipocalimab - reduces IgG autoantibody levels by blocking IgG recycling
Management of Cold Agglutinin Disease (CAD)
Avoid Cold Exposure
- Warming measures are essential: warm clothing, room temperature fluids, warm IV fluids during procedures
- Cold avoidance can substantially reduce hemolysis in mild-moderate CAD
No Role for Steroids or Splenectomy
- Corticosteroids are largely ineffective in CAD (hemolysis is complement-mediated, not splenic phagocytosis of IgG-coated RBCs)
- Splenectomy is also generally not beneficial in CAD (hemolysis occurs primarily in the liver)
First-Line Treatment: Rituximab
- Rituximab 375 mg/m² × 4 doses - targets the pathogenic IgM-producing B-cell clone
- Response rate ~50-60%; median duration ~1 year
- Can be repeated
Rituximab + Bendamustine (More Effective Combination)
- For patients requiring deeper/longer responses
- Response rate ~70-75%; longer remissions
Complement Inhibition (Emerging Standard for Severe CAD)
- Sutimlimab (anti-C1s): First FDA-approved complement inhibitor specifically for CAD (2022). Inhibits the classical complement pathway at C1s. Rapid response; recommended in patients with active hemolysis requiring transfusion.
- Other C1/C3/C5 pathway inhibitors in trials
BTK Inhibitors in CAD
Management of Paroxysmal Cold Hemoglobinuria (PCH)
- Mostly self-limiting in children (post-infectious)
- Supportive care: transfusion if needed, warming, treat underlying infection
- Steroids: variable benefit; may be used in severe cases
- Most resolve within weeks
Management of Drug-Induced AIHA
- Discontinue the offending drug - this is the most important step
- Immune checkpoint inhibitor-induced AIHA (anti-PD1, anti-PDL1, anti-CTLA4):
- High-dose corticosteroids (prednisone 1-2 mg/kg/day)
- Discontinue or hold the checkpoint inhibitor
- IVIG or rituximab for steroid-refractory cases
Summary: Treatment Algorithm for Warm AIHA
Diagnosis confirmed (positive DAT + hemolytic anemia)
|
v
Supportive: Folic acid | Transfusion (if Hb symptomatic) | Treat underlying cause
|
v
FIRST LINE: Prednisone 1 mg/kg/day ± IVIG (severe cases)
|
Response?
/ \
Yes No / Relapse
| |
Taper steroids SECOND LINE: Rituximab 375 mg/m² × 4
over 3-6 months |
Response?
/ \
Yes No
| |
Monitor; re-treat THIRD LINE: Splenectomy
on relapse OR
Azathioprine / MMF / Cyclosporine
|
Refractory
|
Novel agents: BTK-i, SYK-i,
FcRn-i, plasma cell-directed Rx
(Consider clinical trial)
Key Points
- Classify before treating - warm vs. cold AIHA have different mechanisms and require different therapies
- Never withhold transfusion in life-threatening anemia due to crossmatch incompatibility
- Folic acid supplementation in all active AIHA
- Steroids are first-line for wAIHA (not effective in CAD)
- Rituximab is now preferred over splenectomy as second-line in wAIHA
- Splenectomy is reserved for later lines; vaccinate beforehand
- CAD: cold avoidance + rituximab ± bendamustine; sutimlimab for complement-mediated severe CAD
- Secondary AIHA - treat the underlying condition
- A rapidly growing pipeline of novel agents (BTK-i, SYK-i, FcRn-i, anti-plasma cell) is available for refractory disease in 2025-2026
- Monitor for thrombosis - anticoagulation prophylaxis in severe hemolysis
- Goldman-Cecil Medicine International Edition, 2-Volume Set - Chapter 146 (AIHA Classification & Treatment)
- Tintinalli's Emergency Medicine, Comprehensive Study Guide - Chapter 237
- Mulholland & Greenfield's Surgery - Chapter 14
- Barcellini W & Fattizzo B, ASH Hematology Education Program 2025, PMID 41347987 - Management of wAIHA (latest review)
- Berentsen S, ASH Hematology Education Program 2025, PMID 41348049 - Diagnosis and management of cold agglutinin disease
Jyp measurement as per dm level
JVP (Jugular Venous Pressure) Measurement - The Sternal Angle (Angle of Louis) Method
The Core Principle: Why the Sternal Angle?
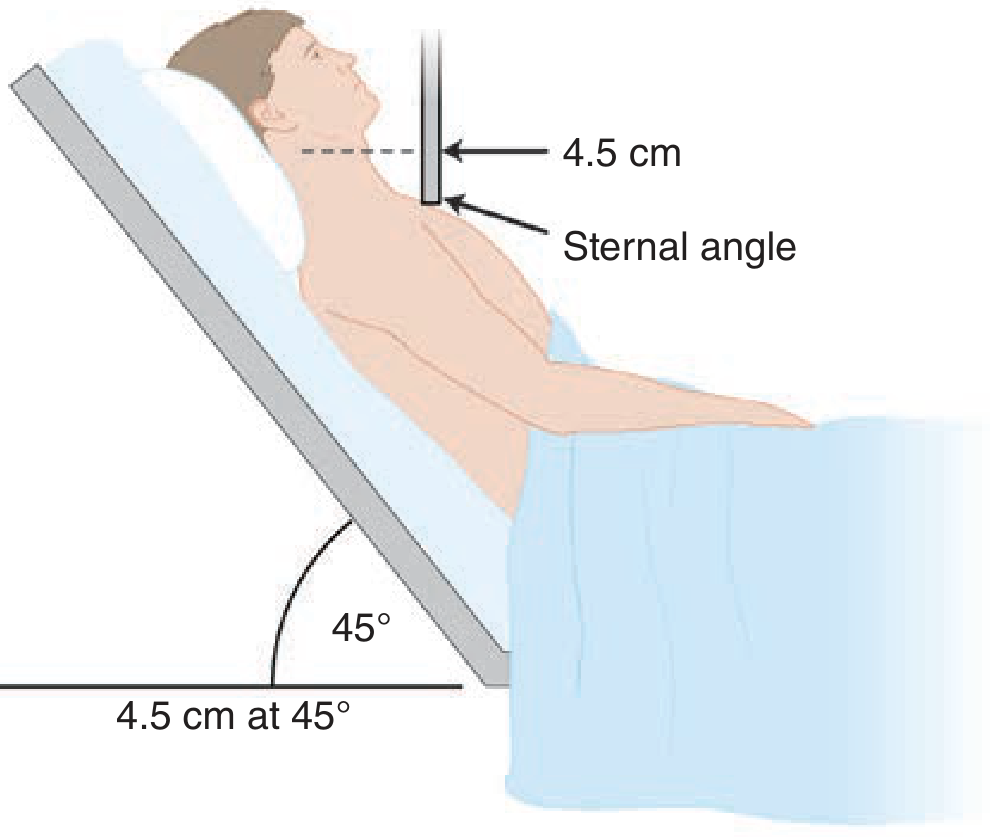
The sternal angle is approximately 5 cm above the center of the right atrium, regardless of the patient's position (whether lying flat, at 30°, 45°, or sitting upright).
The Measurement Technique
Step 1 - Position the Patient
- Position the patient semi-recumbent at 45° (standard position)
- Head turned slightly to the left to expose the right side of the neck
- The right internal jugular vein (IJV) is preferred (more direct path to the right atrium; no valves in the way)
- The external jugular vein is valved, so it is less reliable - but can still distinguish high from low CVP
Step 2 - Identify the Pulsation
- Shine a light tangentially across the neck to cast a shadow that makes the jugular pulsation visible
- The venous pulsation is biphasic (a and v waves); the carotid pulse is monophasic
- The venous pulsation is obliterated by light pressure at the base of the neck; the carotid is not
- Venous pulsation changes with posture and inspiration; carotid does not
Step 3 - Measure the Vertical Height
- Measure the vertical distance (in cm) between the top of the jugular venous column and the sternal angle
- Use a ruler held horizontally from the pulsation point, and a vertical reference from the sternal angle
Step 4 - Calculate CVP
CVP (cm H₂O) = Vertical height above sternal angle (cm) + 5 cm
The Diagram
Normal Values and Interpretation
| Vertical Height Above Sternal Angle | Estimated CVP | Interpretation |
|---|---|---|
| ≤4.5 cm | ≤9.5 cm H₂O | Normal |
| >4.5 cm | >9.5 cm H₂O | Elevated (abnormal) |
| Not visible at 45° | Very low | Suggests hypovolemia |
| Visible even when sitting upright | Very high | Severely elevated CVP |
- Normal CVP: 5-10 cm H₂O (equivalent to ~4-8 mmHg)
- To convert cm H₂O to mmHg: divide by 1.36 (i.e., 1.36 cmH₂O = 1 mmHg)
- A JVP >4.5 cm vertically above the sternal angle at 45° is considered abnormal
Adjusting Patient Position for Difficult Cases
| Suspected CVP | Best Patient Position |
|---|---|
| Very low (hypovolemia) | Flat (0°) - to make veins visible |
| Normal | 30°-45° |
| High (e.g., heart failure) | 60°-90° (sitting upright) |
| Very high and still elevated sitting | Legs dangling off the side of the bed |
Harrison's (2025): "The patient should always be placed in the sitting position, with the legs dangling below the bedside, when an elevated pressure is suspected in the semisupine position."
Important Caveats (Harrison's, 2025)
-
The sternal angle method systematically underestimates CVP - the actual distance from the sternal angle to the mid-right atrium varies with body size and patient angle. Use it to distinguish normal from elevated CVP, not for precise semiquantification.
-
The clavicle is an easier alternative reference point - any venous pulsation visible above the clavicle in the sitting position is clearly abnormal, since the clavicle-to-right-atrium distance is at least 10 cm.
-
Obese or uncooperative patients - IJV visualization may be impossible; use bedside ultrasound instead.
Ultrasound Method (Objective Alternative)
- Use a high-frequency linear transducer (7-9 MHz) on the right neck
- Find the point where the IJV tapers (resembles the neck of a wine bottle)
- Measure the vertical distance from this taper point to the sternal angle, then add 5 cm
- A distended IJV larger than the adjacent common carotid artery in the transverse plane = CVP >10 cm H₂O
- A near-collapsed IJV in the supine position = very low CVP
The JVP Waveform and Its Components
| Component | Timing | Mechanism | Clinical Significance |
|---|---|---|---|
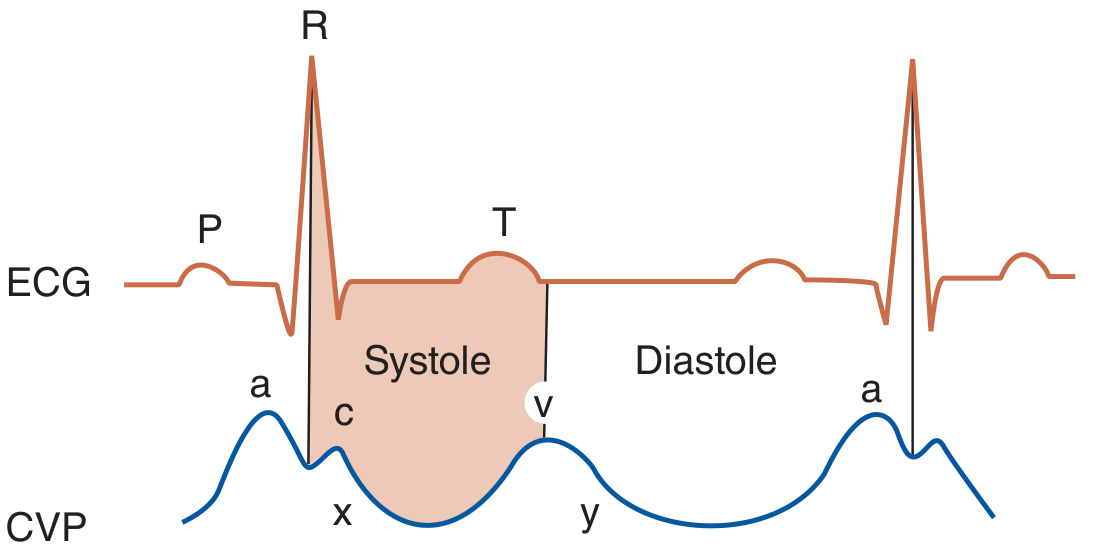
| a wave | Just after ECG P wave, before S1 | Right atrial contraction (presystolic) | Prominent in reduced RV compliance; absent in AF |
| c wave | After a wave | Tricuspid valve bulging into RA during early systole | Often not visible clinically |
| x descent | After a/c | Fall in RA pressure; RA relaxation + tricuspid valve pulling away | Exaggerated in cardiac tamponade |
| v wave | During ventricular systole (after ECG T wave) | Venous filling of RA while tricuspid valve is closed | Large v wave = tricuspid regurgitation |
| y descent | After v wave | Tricuspid valve opens; RA empties into RV | Steep y descent in constrictive pericarditis |
Clinical Significance of Elevated JVP
- Right heart failure / congestive heart failure
- Cardiac tamponade (elevated JVP + pulsus paradoxus + muffled heart sounds = Beck's triad)
- Constrictive pericarditis (Kussmaul's sign: JVP rises with inspiration, opposite of normal)
- Superior vena cava obstruction (non-pulsatile elevation)
- Pulmonary hypertension
- Tricuspid regurgitation (large v waves)
- Fluid overload / over-transfusion
- Harrison's Principles of Internal Medicine, 22nd Edition (2025) - Chapter 246: Cardiovascular Examination
- Goldman-Cecil Medicine International Edition - Chapter 39: Jugular Veins
- Tintinalli's Emergency Medicine, Comprehensive Study Guide - Chapter 32: Jugular Venous Pulsation
Which phase of respiration should it be measured inspiration or expiration
JVP Should Be Measured at End-Expiration
The Direct Answer
The Physiological Reason
"Venous pressure falls during inspiration as a result of the increased negative intrathoracic pressure, and rises again during expiration."
| Phase | Intrathoracic Pressure | Effect on Venous Return | JVP Level |
|---|---|---|---|
| Inspiration | Becomes more negative | Increases venous return into the chest; right heart fills → jugular column is "sucked in" | Falls (JVP drops) |
| Expiration | Returns toward zero / baseline | Venous return normalizes; venous column rises back up | Rises (JVP visible at peak) |
| End-expiration | At baseline | Most stable; venous column at its highest point | Measure here |
Practical Technique
- Ask the patient to breathe normally
- Watch the neck and observe the venous pulsation across several respiratory cycles
- Note that the top of the pulsation rises at end-expiration and falls during inspiration
- Take your measurement at end-expiration - when the column is at its highest
The Exception: Kussmaul's Sign
Kussmaul's Sign = Paradoxical rise in JVP (or failure to fall) with inspiration
- Constrictive pericarditis (classic)
- Cardiac tamponade (sometimes)
- Right ventricular infarction
- Severe right heart failure
- Restrictive cardiomyopathy
- Measure JVP at end-expiration (when the column is highest and most stable)
- During inspiration: JVP normally falls (negative intrathoracic pressure draws blood centrally)
- If JVP rises with inspiration → Kussmaul's sign → think constrictive pericarditis / RV infarction
Tb introduction, pathogenesis clinical features diagnosis management as per ntep and latest standard textbooks
NTEP National TB Elimination Programme India 2025 treatment guidelines regimen drug resistant
"tuberculosis"[MeSH Terms] AND "diagnosis" AND "treatment"
https://www.who.int/teams/global-programme-on-tuberculosis-a…
NTEP India TB treatment regimen 2024 2025 HRZE daily dose drug sensitive MDR XDR nikshay
https://phd.maharashtra.gov.in/en/scheme/national-tuberculos…
Tuberculosis (TB) - Comprehensive Review
1. Introduction
- Rod-shaped, obligate aerobe, slow-growing (doubling time ~20 hours)
- Defined by acid-fastness - retains carbol-fuchsin dye after acid-alcohol washing, due to a uniquely lipid-rich cell wall composed of mycolic acids with acyl chains up to 90 carbons
- High G+C content (65.6%); single circular chromosome of ~4.4 × 10⁶ nucleotides
- The MTBC complex includes: M. tuberculosis, M. africanum, M. bovis, M. canetti
- Humans are the only significant reservoir; virtually all transmission is human-to-human
2. Pathogenesis
2.1 Transmission and Initial Infection
- Spread by aerosolized droplet nuclei (1-5 μm) from an infectious case (smear-positive pulmonary TB)
- A single droplet nucleus may contain 1-3 bacilli; as few as 1-10 bacilli can establish infection
- Once inhaled, bacilli reach the alveoli and are ingested by alveolar macrophages
- Initial innate immunity: neutrophils are recruited first; however, excessive neutrophil activity creates a nutrient-rich environment that supports bacterial replication
2.2 Granuloma Formation (The Central Pathological Event)
- Blocking phagosome-lysosome fusion (prevents acidification and delivery of hydrolases) - key virulence mechanism
- ESX-1 secretion system secretes ESAT-6 and CFP-10 (important for virulence and immune evasion)
- ESX-3 secretes EsxH, which impedes MHC class II antigen presentation
- PE/PPE protein families contribute to immune evasion
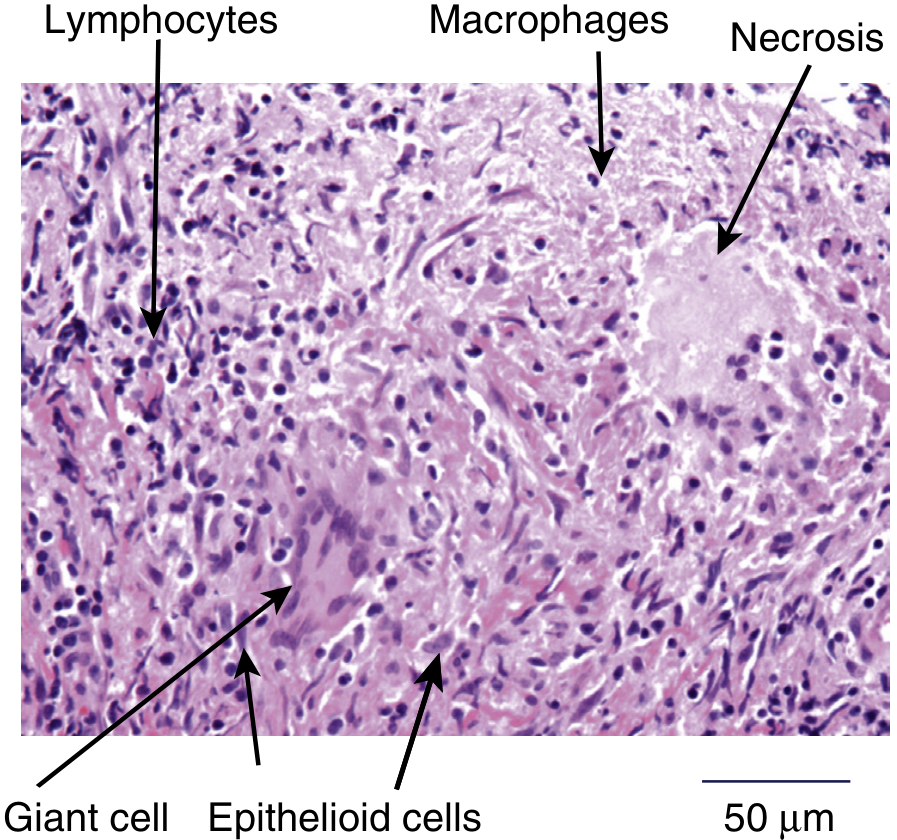
- Macrophages (some transform into epithelioid cells)
- Multinucleated Langhans giant cells (fused macrophages)
- CD4+ and CD8+ T lymphocytes in the periphery
- B cells, dendritic cells, neutrophils
Dual role of granuloma: Initially restricts dissemination; but M. tuberculosis exploits it for cell-to-cell spread, immune evasion, and drug tolerance.
2.3 Adaptive Immunity
- CD4+ T cells are essential - their depletion (as in HIV) dramatically increases risk of active TB
- Key cytokines: IFN-γ and TNF-α are critical for granuloma integrity and bacterial control
- IFN-γ unresponsiveness = Mendelian susceptibility to mycobacterial disease
- TNF-α blockade (anti-TNF biologics like infliximab, adalimumab) reactivates latent TB
- CD8+ T cells and γδ T cells also contribute
2.4 Outcomes After Infection
Exposure to M. tuberculosis
|
↓
~70% - NOT infected (innate immunity clears)
|
~30% - Infected (tuberculin test/IGRA converts positive)
|
┌────┴────┐
5-10% 90%
Primary Latent TB Infection (LTBI)
Active TB (Ghon focus calcifies; dormant bacilli persist)
|
↓
~10% lifetime risk reactivation
(↑ with HIV, DM, malnutrition, immunosuppression)
2.5 Reactivation TB (Post-Primary/Secondary TB)
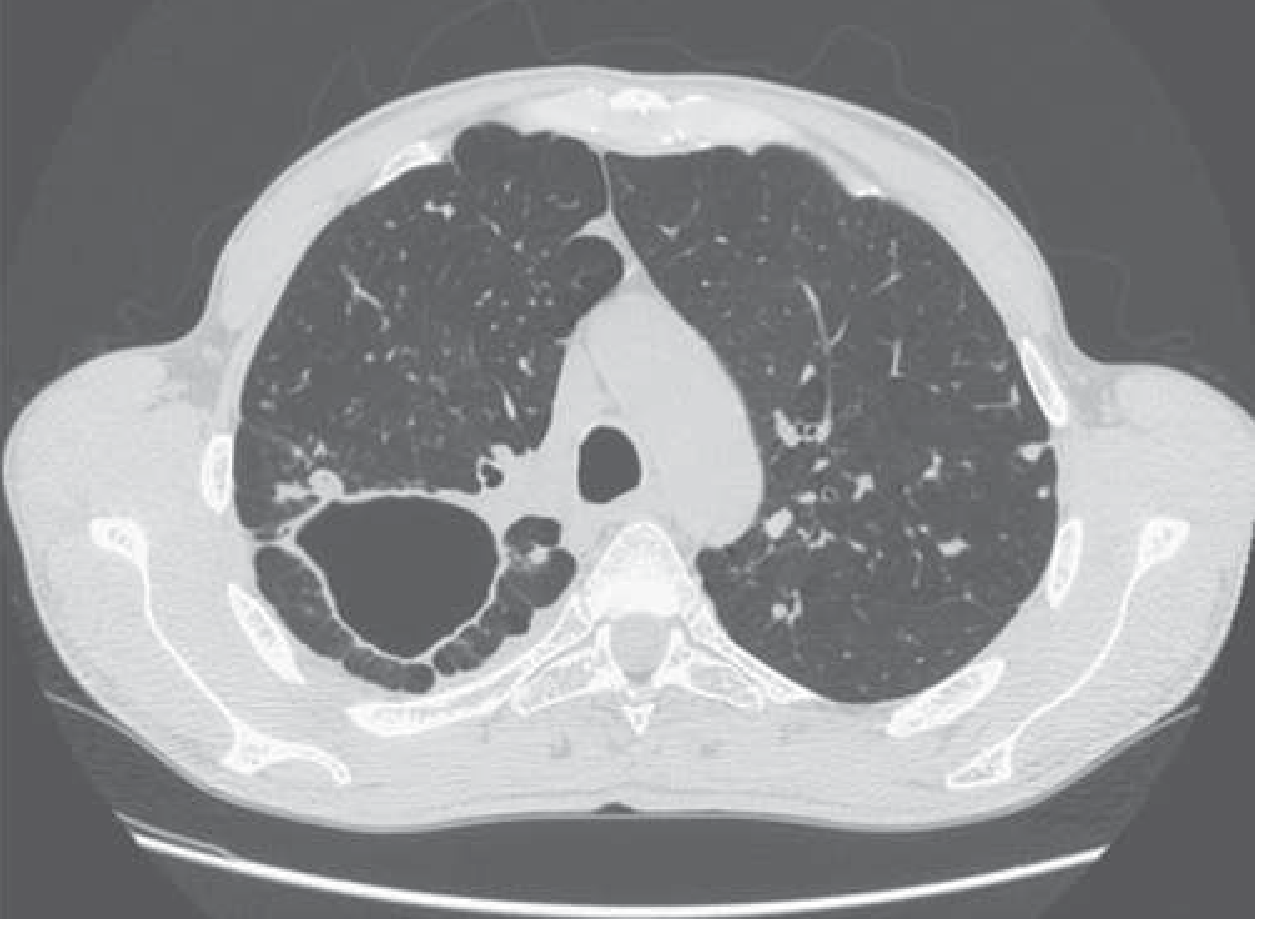
- Usually involves upper lobes (apex/posterior segments) - high oxygen tension favors M. tuberculosis growth
- Features: consolidation → cavitation → bronchogenic spread
- Cavitary disease allows high extracellular bacterial replication and is the source of infectious aerosols
3. Clinical Features
3.1 Pulmonary TB (80-85% of cases)
- Persistent cough >2 weeks (most common presenting symptom)
- Fever (often low-grade, afternoon peaks)
- Night sweats
- Weight loss / anorexia
- Fatigue and malaise
- Cough with mucopurulent sputum
- Hemoptysis - blood-streaked sputum; indicates cavitary disease with tissue destruction
- Breathlessness (with extensive disease)
- Pleuritic chest pain (TB pleuritis)
- Upper zone dullness, bronchial breath sounds over cavities
- Amphoric breath sounds over large cavities
- Crackles at lung apices
- Signs of pleural effusion if present
- Cachexia, pallor in advanced disease
3.2 Extrapulmonary TB
| Site | Features |
|---|---|
| Lymph nodes (most common EPTB) | Painless cervical/mediastinal lymphadenopathy; may cavitate and form "cold abscess" (no overlying inflammation); scrofula |
| Pleura (TB pleuritis) | Exudative effusion; lymphocytic, high protein, high ADA (>40 U/L); low glucose |
| CNS (TB meningitis) | Subacute meningitis; CSF: lymphocytic pleocytosis, high protein, low glucose, positive AFB smear in only 30-40%; disabling; mortality 18-40% |
| Skeletal (Pott's disease) | Vertebral TB (especially T10-L1); kyphosis (gibbus deformity); paravertebral "cold abscess"; compression myelopathy |
| Genitourinary | Sterile pyuria + microscopic hematuria; "putty kidney" calcification; salpingitis → infertility |
| Abdomen | Ileocecal most common; diarrhea, RIF pain; ascites; intestinal obstruction |
| Pericardium | Constrictive pericarditis; pericardial effusion |
| Miliary TB | Hematogenous dissemination; "millet seed" pattern on CXR; found in HIV, immunosuppressed |
| Adrenals | Addison's disease (bilateral adrenal destruction) |
4. Diagnosis
4.1 Presumptive Diagnosis (WHO / NTEP Definition)
4.2 Chest X-Ray
- Primary TB: Middle/lower lobe infiltrate, hilar lymphadenopathy, Ghon complex
- Post-primary/reactivation TB: Upper lobe infiltrates, cavitation, fibrosis, consolidation, pleural effusion
- Miliary TB: Diffuse 1-3 mm nodular ("millet seed") shadows throughout both lung fields
- Not diagnostic alone but critical screening tool; AI-enabled portable X-ray now deployed under NTEP 2025
4.3 Sputum Smear Microscopy (ZN Stain / Fluorescence)
- Ziehl-Neelsen (ZN) stain for acid-fast bacilli (AFB)
- Sensitivity: 40-60% (requires ≥5000-10,000 bacilli/mL)
- Requires 3 sputum samples (spot-morning-spot) under NTEP
- Fluorescence microscopy (auramine-rhodamine) is more sensitive - preferred by WHO
- Cannot distinguish M. tuberculosis from NTM; cannot detect drug resistance
4.4 Molecular Tests (NTEP First-Line - Universal DST)
- Detects M. tuberculosis DNA + rifampicin resistance simultaneously
- Sensitivity ~88% (smear-positive), ~67% (smear-negative)
- Result in 2 hours
- Gold standard for rapid TB diagnosis and initial rifampicin resistance screening in India
- NTEP: 171 CBNAAT sites + 624 Truenat sites across India (2025)
- FL-LPA (GenoType MTBDRplus): Detects RIF resistance (rpoB mutations) + INH resistance (katG, inhA mutations)
- SL-LPA (GenoType MTBDRsl): Second-line DST - detects fluoroquinolone (gyrA/gyrB) and injectable resistance
- Used for rapid MDR-TB confirmation
4.5 Culture (Gold Standard)
- Liquid culture (MGIT 960): Positive in 1-3 weeks; more sensitive
- Solid culture (LJ medium): Positive in 4-8 weeks; slow but inexpensive
- Definitive confirmation; allows full DST (phenotypic)
- Threshold: ≥10 bacilli/mL
4.6 Tuberculin Skin Test (TST / Mantoux Test)
- 5 TU PPD (Purified Protein Derivative) injected intradermally
- Read at 48-72 hours; measure induration (not erythema)
| Induration | Considered Positive In |
|---|---|
| ≥5 mm | HIV-infected, immunocompromised, close TB contact, CXR showing old healed TB, organ transplant |
| ≥10 mm | Healthcare workers, high-risk groups, children <5 years, persons from high-burden countries |
| ≥15 mm | Low-risk persons with no known exposures |
- Limitations: False positive with BCG vaccination; false negative in HIV, severe malnutrition, miliary TB, immunosuppression (anergy)
4.7 IGRA (Interferon-Gamma Release Assay)
- QuantiFERON-TB Gold and T-SPOT.TB
- In vitro whole-blood test; measures IFN-γ release by T cells to M. tuberculosis antigens (ESAT-6, CFP-10, TB7.7)
- Unaffected by BCG vaccination - more specific than TST in BCG-vaccinated populations
- Positive IGRA = LTBI (not active TB)
4.8 Other Tests
- ADA (Adenosine Deaminase): Pleural/CSF/pericardial fluid; ADA >40 U/L in pleural fluid suggests TB pleuritis; high sensitivity
- Biopsy + histopathology: Caseating granuloma with AFB = diagnostic; applicable to lymph node, pleura, pericardium, bone
- FNAC: Lymph node aspiration - AFB smear + culture
- BAL (bronchoalveolar lavage): For smear-negative/difficult cases
5. Management
5.1 NTEP Treatment Framework: Detect - Treat - Prevent - Build
- Detect - Universal screening, U-DST for all new patients
- Treat - Free daily FDC drugs, patient support
- Prevent - TB Preventive Therapy (TPT), infection control
- Build - Health system strengthening, Nikshay platform
5.2 Drug-Sensitive TB (DS-TB) Treatment Regimen
Standard Regimen: 2HRZE / 4HR
| Phase | Duration | Drugs | Abbreviation |
|---|---|---|---|
| Intensive phase | 2 months | Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) | 2HRZE |
| Continuation phase | 4 months | Isoniazid (H) + Rifampicin (R) | 4HR |
| Total duration | 6 months | All oral, daily |
| Weight Band | Intensive Phase (HRZE) | Continuation Phase (HR) |
|---|---|---|
| 25-39 kg | 2 tablets (75/150/400/275 mg) | 2 tablets (75/150 mg) |
| 40-54 kg | 3 tablets | 3 tablets |
| 55-69 kg | 4 tablets | 4 tablets |
| ≥70 kg | 5 tablets | 5 tablets |
- Isoniazid (H): 5 mg/kg (max 300 mg/day) - bactericidal; pyridoxine (B6) 25-50 mg/day given with INH to prevent peripheral neuropathy
- Rifampicin (R): 10 mg/kg (max 600 mg/day) - sterilizing agent; strong hepatic CYP450 inducer
- Pyrazinamide (Z): 25 mg/kg (max 2g/day) - kills intracellular bacilli in acidic environment; used only in intensive phase
- Ethambutol (E): 15-20 mg/kg/day - bacteriostatic; monitor for optic neuritis (color vision testing)
- Baseline LFTs, complete blood count, renal function, visual acuity + color vision
- Monthly sputum AFB smear at end of months 2, 5, 6
- If smear-positive at end of 2 months: extend intensive phase by 1 month (3HRZE + 4HR)
- Sputum culture conversion is key marker of response
Extended Regimens for Specific Sites:
| Site | Duration | Modification |
|---|---|---|
| TB meningitis | 9-12 months (2HRZE/7-10HR) | + Dexamethasone 0.4 mg/kg/day (adults) tapering over 6-8 weeks |
| Bone/Joint TB | 6-9 months | May extend continuation phase by 3 months |
| Pericardial TB | 6 months + corticosteroids | Prednisolone to reduce constrictive pericarditis risk |
| Extensive miliary/disseminated | 6-9 months |
5.3 Drug-Resistant TB (DR-TB) - NTEP Guidelines
Classification:
| Type | Definition |
|---|---|
| RR-TB | Rifampicin-resistant (detected by Xpert/Truenat) |
| MDR-TB | Resistant to both H + R |
| Pre-XDR-TB | MDR-TB + resistance to any fluoroquinolone |
| XDR-TB | MDR-TB + fluoroquinolone + bedaquiline or linezolid resistance |
| HR-TB (Isoniazid-resistant, RIF-susceptible) | Resistant to H only |
Hierarchy of Drug Selection for MDR-TB (Murray & Nadel / WHO):
| Priority | Group | Drugs |
|---|---|---|
| Step 1 (choose 1) | Later-generation fluoroquinolones | Levofloxacin, Moxifloxacin |
| Step 2 (choose both) | Core agents | Bedaquiline, Linezolid |
| Step 3 (choose both) | Add-on agents | Clofazimine, Cycloserine |
| Step 4 (if needed) | Injectables (last resort) | Amikacin, Streptomycin |
| Step 5 (if needed) | Additional oral | Delamanid, Pyrazinamide, Ethambutol |
| Step 6 (last resort) | Reserve | Ethionamide, Carbapenems, PAS, High-dose INH |
Modern Short Regimens (WHO 2024-2025, now adopted by NTEP):
- Bedaquiline + Pretomanid + Linezolid + Moxifloxacin
- First 6-month all-oral MDR-TB regimen approved (2022, based on ZeNix/TB-PRACTECAL trials)
- 97 countries using this by end of 2024
- Bedaquiline + Pretomanid + Linezolid
- For MDR/RR-TB without fluoroquinolone resistance; fluoroquinolone-susceptible
India: 34,256 patients started on 6-month regimens globally in 2024 (up from 5,653 in 2023); India's DR-TB treatment success rate has improved from 59% (2018) to 74% (2021 cohort) under NTEP.
Isoniazid-Resistant TB (Hr-TB):
- Regimen: 6R-E-Z-Lfx (Rifampicin + Ethambutol + Pyrazinamide + Levofloxacin for 6 months)
- Do not use standard 2HRZE/4HR as inadequate resistance coverage
5.4 Directly Observed Therapy (DOT)
- Standard practice under NTEP for all TB patients
- Benefits: improved treatment success, earlier sputum conversion, reduced relapse, early detection of adverse effects
- Evidence: Even minimal non-adherence significantly worsens outcomes (HR 2.4 at >90% but sub-perfect adherence; HR 5.9 at ≤90% adherence)
- DOT can be facility-based, community-based, or via video-observed therapy (VOT) - all accepted under NTEP
- NTEP case manager assigned to each patient for individualized support
5.5 TB Preventive Therapy (TPT)
- HIV-infected persons (regardless of TST/IGRA result)
- Household child contacts <5 years of active TB cases
- Household contacts ≥5 years who are TST/IGRA positive
- Persons on immunosuppressive therapy (anti-TNF, transplant recipients)
- Silicosis patients
| Regimen | Duration | Drugs |
|---|---|---|
| 6H | 6 months | Isoniazid daily |
| 3HP | 3 months | Isoniazid + Rifapentine weekly (12 doses) |
| 1HP | 1 month | Isoniazid + Rifapentine daily |
| 3HR | 3 months | Isoniazid + Rifampicin daily |
| 4R | 4 months | Rifampicin daily |
Always rule out active TB before starting TPT.
5.6 Special Situations
TB-HIV Coinfection:
- Start ART within 2-8 weeks of starting ATT (regardless of CD4 count) - improves survival
- Exception: TB meningitis - delay ART 4-8 weeks to reduce IRIS risk
- Rifampicin-based regimens reduce antiretroviral drug levels significantly (enzyme induction); use Efavirenz-based ART
- Immune Reconstitution Inflammatory Syndrome (IRIS): Paradoxical worsening after ART initiation; manage with corticosteroids
TB in Pregnancy:
- Standard 2HRZE/4HR regimen is safe
- Streptomycin is contraindicated (ototoxicity to fetus)
- Pyridoxine supplementation mandatory
- Breastfeeding is allowed on ATT (small drug levels in breast milk, not harmful)
TB with Diabetes Mellitus:
- DM doubles the risk of TB and worsens outcomes
- Monitor blood glucose; optimize glycemic control
- Ethambutol + isoniazid toxicity monitoring more careful
- May need extended treatment duration
Drug-Induced Hepatotoxicity (DILI from ATT):
- Most common cause of stopping ATT
- Stop all ATT if: ALT >3× ULN + symptoms, or ALT >5× ULN (asymptomatic)
- Sequential re-introduction after LFT normalization: R → H → Z → E
- If unable to reintroduce, use non-hepatotoxic regimen: Ethambutol + Quinolone + Aminoglycoside
6. Monitoring and Follow-Up (NTEP)
| Timepoint | Assessment |
|---|---|
| Baseline | AFB smear + culture, CXR, LFT, CBC, renal function, visual acuity, HIV testing, blood glucose |
| End of month 2 | Sputum AFB smear (key decision point); extend IP if positive |
| End of month 5 | Sputum AFB smear |
| End of treatment (month 6) | Sputum smear + culture for treatment outcome assessment |
| Outcome | Definition |
|---|---|
| Cured | Bacteriological confirmation of cure (smear/culture negative at end of treatment) |
| Treatment completed | Completed treatment without evidence of failure but no bacteriological confirmation |
| Treatment failed | Smear/culture positive at month 5 or later |
| Died | Died during treatment |
| Lost to follow-up | Treatment interrupted for ≥2 consecutive months |
| Not evaluated | No outcome assigned |
| Treatment success | Cured + Treatment completed |
7. Infection Control (NTEP)
- Respiratory isolation for smear-positive pulmonary TB: negative pressure room ideal; otherwise adequate ventilation
- N95 respirators for healthcare workers
- Administrative controls: Early identification, triage, fast-track evaluation of presumptive TB
- Environmental controls: UV light (UVGI), natural ventilation, HEPA filtration
- BCG vaccination at birth (national immunization program in India) - protects against severe childhood forms (miliary TB, TB meningitis) but variable efficacy against adult pulmonary TB
8. India NTEP 2025 - Key Highlights
- 100-Day TB Mukt Bharat Abhiyan (Dec 2024 - March 2025): Intensive elimination drive across 347 high-priority districts, scaling up nationwide
- 26.18 lakh TB patients diagnosed in 2024 (92% treatment coverage vs 53% in 2015)
- AI-enabled handheld X-ray devices deployed for field screening
- Universal DST: 92% of new notified cases in India tested for Rifampicin sensitivity (vs 83% globally)
- Ni-kshay Mitra initiative: Community volunteers/organizations adopt TB patients and provide social support
- Nikshay Poshan Yojana: ₹4,406 crore disbursed to 1.37 crore beneficiaries since 2018
- Target: TB-free India by 2025 (5 years ahead of SDG 2030 target)
- Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume Set - Chapters 52 (Pathogenesis) and 54 (Chemotherapy)
- Medical Microbiology, 9th Edition - Chapter 22 (Clinical features, Laboratory diagnosis)
- Goldman-Cecil Medicine International Edition - Chapter 296
- NTEP (National Tuberculosis Elimination Programme) - Government of India, 2025
- WHO Global Tuberculosis Report 2025 - WHO DR-TB Treatment
- PIB India press releases, Nov 2025 - NTEP national updates
More detailed on pathogenesis and clinical features with mechanism and diagnostic test with latest advances in detail for md medicine level
"Mycobacterium tuberculosis" AND "pathogenesis" AND "macrophage"
"tuberculosis" AND "diagnosis" AND "novel biomarker" OR "molecular test"
"tuberculosis" AND "diagnosis" AND "advances"
PMID: 37490968
PMID: 39774813
Tuberculosis - MD Medicine Level: Pathogenesis, Clinical Features & Diagnostics
PART I: PATHOGENESIS - Molecular and Cellular Mechanisms
1.1 The Organism and Its Virulence Architecture
| Factor | Gene/Locus | Mechanism |
|---|---|---|
| Mycolic acids | Cell wall | 90-carbon lipid chains create impermeable barrier; acid-fast staining property; resists lysosomal killing |
| Lipoarabinomannan (LAM) | Cell wall glycolipid | Inhibits intracellular Ca²⁺ increase → blocks Ca²⁺/calmodulin pathway → prevents phagosome-lysosome fusion |
| ESAT-6 / CFP-10 | RD1 locus (ESX-1) | Pore-forming proteins; perforate phagosomal membrane; essential for virulence; absent in BCG (key attenuating mutation) |
| PDIM (phthiocerol dimycocerosate) | Cell wall lipid | Works with ESX-1 to perforate phagosomal membrane; promotes type I IFN responses |
| EsxH | ESX-3 secretion | Inhibits ESCRT (endosomal sorting complex) which normally repairs phagosomal damage - thus ESX-1 damages, ESX-3 prevents repair |
| PE_PGRS47 | PE/PPE gene family | Suppresses autophagy; interferes with ATG gene expression |
| KatG (catalase-peroxidase) | katG gene | Protects against oxidative stress; also required for isoniazid activation → mutations = INH resistance |
| Rv3671c | Membrane protein | Maintains neutral bacterial pH even in acidic lysosomal environment |
| DosS/DosT, PhoP/PhoR | Two-component regulators | Detect O₂, NO, CO levels; trigger dormancy-related gene expression (DosR regulon) |
1.2 Step-by-Step Pathogenesis: From Inhalation to Disease
Stage 1: Inhalation and Early Alveolar Events
- Droplet nuclei (1-5 μm) carrying 1-3 bacilli are inhaled
- Larger particles trapped in mucus blanket and cleared by ciliary escalator
- Fraction reaches alveoli: myeloid dendritic cells are the first cells encountered
- Subsequently, alveolar macrophages (prototypic alternatively activated, M2-like) phagocytose the bacilli
- Complement receptors (CR3/CR4) - opsonized via C3b/C3bi after complement activation
- Mannose receptor - binds ManLAM on mycobacterial cell wall; importantly, also downregulates post-phagocytic inflammatory signaling
- FcγR (immunoglobulin G receptor)
- Type A scavenger receptors
- Surfactant protein D can prevent phagocytosis (protective)
2025 update (Nat Rev Immunol, Russell et al., PMID 39774813): There are two distinct macrophage lineages in the lung: (1) embryonically-derived tissue-resident alveolar macrophages (TR-AMs) and (2) recruited blood monocyte-derived interstitial macrophages (MoAMs). These respond divergently to M. tuberculosis within the granuloma. TR-AMs are more permissive to infection while MoAMs mount stronger bactericidal responses. This macrophage heterogeneity determines disease outcome and response to therapy.
Stage 2: Phagosome Arrest - The Core Evasion Mechanism
Phagosome formed
↓
Acidification (V-ATPase assembly)
↓
Acquisition of lysosomal hydrolases, cathepsins
↓
NADPH oxidase generates ROS
↓
LC3-associated phagocytosis (LAP)
↓
Phagolysosome = bacterial killing
- LAM inhibits Ca²⁺/calmodulin pathway → prevents phagosome-lysosome fusion signaling
- Blocks PI3P (phosphatidylinositol 3-phosphate) production on phagosome surface → PI3P normally marks phagosomes for membrane sorting and maturation
- Prevents V-ATPase assembly → phagosome does not acidify → lysosomal hydrolases remain inactive
- Early endosomal markers retained (Rab5, EEA1), late endosomal markers (Rab7, LAMP-1) absent → arrested maturation
- NADPH oxidase, LC3 absent from mycobacterial phagosome → no ROS-mediated killing, no LAP pathway activation
- ESX-1 secretion of ESAT-6/CFP-10 perforates phagosomal membrane → bacilli gain access to cytosol, deliver effectors, acquire nutrients
- EsxH (ESX-3) blocks ESCRT → host cannot repair the membrane damage caused by ESX-1
- Autophagy blocked by PE_PGRS47 and other effectors → autophagosome cannot engulf and destroy the bacillus
- Catalase/SOD/alkyl hydroperoxidase enzymes neutralizing ROS
- Membrane protein Rv3671c maintaining neutral internal bacterial pH in acidic environment
Stage 3: Metabolic Reprogramming of the Host Macrophage
- Warburg effect induction: Shifts macrophage metabolism from oxidative phosphorylation → aerobic glycolysis (normally a feature of cancer cells). This generates a hypoxic, lactate-rich intracellular environment favorable to bacterial persistence.
- Foamy macrophage formation: Induction of lipid droplet accumulation within macrophages. These "foamy" lipid-laden macrophages line the inner granuloma. Bacilli extract cholesterol esters and fatty acids from lipid droplets as their carbon/energy source.
- Iron sequestration subverted: ESX-3 (via EsxH) is essential for mycobacterial iron acquisition from the host cell.
- Potential host-directed therapies exploiting this: statins (reverse foamy macrophage formation, enhance autophagy) and metformin (modulates host metabolism, enhances intracellular killing).
Stage 4: Cytokine Responses and Innate Signaling
- TLR2: Recognizes lipoproteins, LAM → NF-κB → TNF-α, IL-12
- TLR4: LPS-like components
- TLR9: CpG mycobacterial DNA
- NOD2 (NLR): Detects muramyl dipeptide → NF-κB activation → pro-inflammatory cytokines
- cGAS-STING pathway: Detects cytosolic mycobacterial DNA → cyclic GMP-AMP (cGAMP) → STING → IRF3 → Type I IFN (IFN-α/β) production
- NLRP3 inflammasome: Activated by lysosomal damage and ESX-1 → caspase-1 activation → IL-1β and IL-18 maturation
| Cytokine | Source | Role in TB | Clinical relevance |
|---|---|---|---|
| TNF-α | Macrophages, T cells | Activates macrophage microbicidal activity; granuloma integrity; enhances infected cell death | Anti-TNF therapy (infliximab, adalimumab, etanercept) = 25× ↑ TB risk; reactivates LTBI; mandatory LTBI screening before use |
| IFN-γ | CD4+ T cells, NK cells | Master regulator of macrophage activation; enhances autophagy; MHC II upregulation; essential for granuloma maintenance | IFN-γ receptor mutations = Mendelian susceptibility to mycobacterial disease (MSMD); genetic unresponsiveness → disseminated TB |
| IL-12 / IL-23 | Macrophages, DCs | Drive Th1 differentiation; IL-12 induces IFN-γ production | IL-12 receptor deficiency = MSMD |
| IL-1β | Inflammasome | Pyroptotic cell death; promotes granuloma formation | Balanced with anti-inflammatory IL-10 |
| IL-10 | Regulatory macrophages | Anti-inflammatory; may allow bacterial persistence if overproduced | Elevated in active TB; contributes to immune evasion |
| Type I IFN (IFN-α/β) | Macrophages (cGAS-STING) | Paradoxically harmful in TB: suppresses IL-1β/IL-1α production; impairs macrophage bactericidal activity | Blood transcriptomic "IFN signature" correlates with active TB disease severity (Berry et al., 2010) |
Critical paradox: Type I IFN, which is protective in viral infections, is detrimental in TB. ESAT-6/PDIM-mediated phagosomal damage triggers cGAS-STING → Type I IFN → suppresses protective IL-1β production → worse outcomes. This explains why interferon therapy worsens TB and is a target for host-directed therapy.
Stage 5: Granuloma Formation and Dynamics
Initial macrophage infection
↓
Macrophage secretes chemokines (CCL2, CXCL10, IL-8)
↓
Recruitment of: monocytes → macrophages
neutrophils (early, transient)
NK cells
dendritic cells
↓
Macrophages aggregate; some undergo EPITHELIOID transformation
Some fuse → LANGHANS GIANT CELLS (multinucleated)
↓
Adaptive immune cells recruited:
CD4+ T cells (peripheral rim) → IFN-γ production
CD8+ T cells
B cells (at periphery / tertiary lymphoid structures)
↓
Center undergoes CASEATING NECROSIS:
• Enzymatic digestion of cells
• Lipid-rich cheese-like texture (caseum)
• Bacteria can replicate extracellularly in caseum
↓
Progressive disease: Liquefaction of caseum → CAVITATION
• Bacillary burden ↑↑ (up to 10⁸/mL)
• Erodes bronchus → coughing = aerosol generation → transmission
| Protective Function | Pathological Function |
|---|---|
| Restricts hematogenous dissemination | Enables cell-to-cell bacterial spread via macrophage aggregates |
| Contains bacilli in walled-off space | Blocks adaptive immune cell access to bacteria |
| Kills some bacilli via macrophage activation | Drives bacteria into non-replicating drug-tolerant state |
| Prevents systemic spread | Granuloma expansion = tissue destruction (immunopathology) |
2024-2025 advance (Spatial transcriptomics, Qiu et al., PMID 39431015; Pyle et al., PMID 40772762): Single-cell and spatial transcriptomics of granulomas reveal: (1) distinct immune microenvironments in different granuloma compartments; (2) osteopontin-producing macrophages as central mediators of granuloma formation; (3) heterogeneity of individual granulomas even within a single patient - some progressing, some regressing.
Stage 6: Dormancy and Latent TB (LTBI)
- DosR regulon (DevR): ~50 genes activated in response to hypoxia (↓O₂), nitric oxide (NO), CO within the hypoxic granuloma core. Encodes proteins for adaptation to anaerobic survival.
- DosS and DosT: Sensor kinases that detect O₂, NO, CO → phosphorylate DosR → transcription of dormancy genes
- Sigma factor B (SigB): Stress response
- WhiB3: Redox sensor; metabolic reprogramming
- Slow/non-replicating → resistant to most antibiotics (which target replicating cells)
- Maintain membrane integrity but minimal metabolic activity
- Located in calcified granuloma (Ghon focus), mediastinal lymph nodes
- Can persist for decades → reactivation when immunity wanes (HIV, malnutrition, diabetes, immunosuppression, aging)
Stage 7: Reactivation Disease (Post-Primary TB)
| Condition | Mechanism |
|---|---|
| HIV infection (especially CD4 <200) | Loss of CD4+ T cells → granuloma breakdown |
| Anti-TNF therapy | Disrupts granuloma integrity and macrophage activation |
| Diabetes mellitus | Impaired macrophage function, hyperglycemia favors bacterial growth |
| Malnutrition/low BMI | Deficient cell-mediated immunity |
| Silicosis | Silica particles destroy alveolar macrophages |
| Renal failure (dialysis) | Uremia impairs T-cell function |
| Glucocorticoid therapy | Broad immunosuppression |
| Hematologic malignancy (CLL, lymphoma) | Impaired cellular immunity |
| Post-solid organ transplant | Immunosuppressive drugs |
| Aging | Immunosenescence |
1.3 Why Upper Lobe Predominance?
- Apex of upper lobes has highest pO₂ (150-170 mmHg) and poorest lymphatic drainage
- Lower perfusion-ventilation ratio in apices reduces immune surveillance
- Bacteria reactivate and replicate preferentially here
- Results in: apical/posterior segment consolidation → cavitation → bronchogenic spread to lower lobes
PART II: CLINICAL FEATURES - Mechanistic Understanding
2.1 Primary TB (First infection - usually children)
- Bacilli reach alveoli → initial pneumonitis (usually mid/lower zone - better ventilated area in upright children)
- Ghon focus forms (subpleural parenchymal lesion, usually <1 cm)
- Bacilli travel via lymphatics to hilar/mediastinal lymph nodes → lymphadenopathy
- Ghon complex = Ghon focus + draining lymph nodes
- Most lesions heal with fibrosis + dystrophic calcification → Ranke complex on CXR (calcified primary focus + calcified hilar node = "dumbbell" pattern)
- Primary progressive TB: <5 years, HIV, malnourished → lesion enlarges, lymph nodes compress airways
- Low-grade fever, mild cough
- Enlarged lymph nodes may cause: bronchial compression → obstructive emphysema or atelectasis; or erode into bronchus → bronchial TB
- Erythema nodosum and phlyctenular conjunctivitis (hypersensitivity manifestations)
2.2 Post-Primary (Reactivation) TB - Pulmonary
| Symptom | Mechanism |
|---|---|
| Cough (most common) | Airway inflammation; bronchial irritation; cavities communicate with bronchi |
| Fever + night sweats | TNF-α, IL-1β, IL-6 → hypothalamic prostaglandin E₂ → thermoregulatory disruption; diurnal variation (peak afternoon/evening due to activity and cortisol nadir) |
| Weight loss / cachexia | TNF-α (originally called "cachectin") → anorexia, accelerated catabolism, lipolysis; impaired nutrient absorption |
| Hemoptysis | (1) Bronchial artery erosion in cavity wall; (2) Rasmussen's aneurysm - dilated artery in cavity wall ruptures; (3) Aspergilloma in old cavity (secondary cause) |
| Dyspnea | Extensive parenchymal involvement; associated pleural effusion; miliary disease |
| Amphoric breath sounds | Cavity with narrow neck resonates like bottle opening |
| Hyponatremia (SIADH) | Inflammatory cytokines stimulate ADH secretion; also direct hypothalamic involvement in miliary TB |
| Finger clubbing | Chronic hypoxemia in advanced/extensive disease (less common) |
- Mild normocytic anemia - chronic disease → increased hepcidin → iron sequestration + reduced erythropoiesis
- Leukocytosis, thrombocytosis - inflammatory response; IL-6 drives platelet production
- Raised ESR and CRP - acute phase proteins driven by IL-6
- Lymphopenia - anti-inflammatory mechanisms; also if HIV co-infected
2.3 Extrapulmonary TB - Mechanisms
Tuberculous Lymphadenitis (35% of EPTB)
- Initial lymph node seeding during primary bacteremia → bacilli contained
- Reactivation → caseous necrosis of node → cold abscess (no overlying erythema/heat because indolent inflammation without acute phase reactants)
- Lymph node softens → collar stud abscess (penetrates deep fascia, subcutaneous pointing abscess with underlying firm node = "collar stud" or "dumbbell" abscess)
- Most common: cervical (posterior triangle), axillary; in HIV: more often abdominal/disseminated
TB Meningitis (Most Dangerous Form)
- Hematogenous seeding → Rich focus (small subependymal or subpial granuloma) forms during primary bacteremia
- Rich focus ruptures into subarachnoid space → meningitis
- Thick gelatinous exudate at base of brain → basal meningitis
- Inflammation → vasculitis of perforating arteries → lacunar infarcts (especially BG, internal capsule)
- CSF outflow obstruction → hydrocephalus (communicating type initially)
- Cranial nerve involvement (CN II, III, IV, VI, VII in subarachnoid segments)
- Stage I: No altered consciousness, no neurological deficit
- Stage II: Altered consciousness (GCS 15-10) OR minor neurological deficit
- Stage III: GCS <10, severe neurological deficit, coma
| Parameter | Finding | Mechanism |
|---|---|---|
| Appearance | Pellicle formation on standing ("cobweb clot") | High fibrinogen content |
| WBC | 100-500 cells/μL (predominantly lymphocytes) | T cell-mediated inflammation |
| Protein | Very high (100-500 mg/dL) | Vascular permeability + barrier breakdown |
| Glucose | Low (<45 mg/dL; CSF:serum <0.5) | Glucose utilization by bacilli + impaired transport |
| Chloride | Decreased | Follows glucose (CSF chloride normally higher than serum) |
| AFB smear | Positive only 30-40% (requires large centrifuged volume) | Low bacterial concentration; technical issues |
| ADA | >10 U/L in CSF suggestive | Reflects T-lymphocyte activity |
Pott's Disease (Spinal TB)
- T10-L1 most commonly (highest mobility + mechanical stress + rich blood supply)
- Anterior vertebral body destruction → anterior collapse → angular kyphosis (gibbus deformity)
- Paravertebral cold abscess travels along fascial planes: psoas abscess (descends under inguinal ligament to femoral triangle); retropharyngeal abscess (upper cervical); mediastinal abscess
- Cord compression: anterior (rare in early) → myelopathy
Genitourinary TB
- "Sterile pyuria" = pyuria with negative standard urine culture → strongly suspect GU-TB
- Bacilli reach kidney during bacteremia → cortical granulomas → papillary necrosis → fibrosis → "putty kidney" calcification (dystrophic calcification in necrotic renal parenchyma)
- Ureteral stricture → hydronephrosis
- Bladder: contracted bladder, fish-hook ureter (elevation of ureteral orifice)
Miliary TB
- Primary infection (young children, immunosuppressed)
- Erosion of a pulmonary/lymph node lesion into a blood vessel
- Paradoxical reaction during treatment (rare)
- Choroidal tubercles on fundoscopy (pathognomonic of miliary TB; found in 15-20%)
- Adrenal gland: Bilateral destruction → Addison's disease (hypocortisolism)
- Bone marrow: Pancytopenia, leuco-erythroblastic picture
- Liver: Elevated ALP (alkaline phosphatase) out of proportion to transaminases
PART III: DIAGNOSTIC TESTS - Mechanisms, Interpretation and Latest Advances
3.1 Sputum Smear Microscopy
- Primary stain: Carbol fuchsin (fuchsin + phenol) - penetrates mycolic acid-rich cell wall when heated
- Decolorizer: Acid-alcohol (3% HCl in 95% ethanol) - removes dye from non-acid-fast organisms; mycobacteria retain dye due to mycolic acids
- Counterstain: Methylene blue - non-AFB appear blue; AFB appear bright red
- Requires ≥5,000-10,000 bacilli/mL → low sensitivity (40-60% in smear-positive pulmonary TB; 20-30% in smear-negative)
- LED fluorescence microscopy (Auramine-rhodamine): 10-15% more sensitive than ZN; faster scanning; preferred by WHO
- Cannot speciate; cannot detect drug resistance
- Still important because: cheap, fast, indicates infectiousness
| Grade | Bacilli seen | Report |
|---|---|---|
| Scanty | 1-9 per 100 fields | Report exact number |
| 1+ | 10-99 per 100 fields | 1+ |
| 2+ | 1-10 per field | 2+ |
| 3+ | >10 per field | 3+ |
3.2 Nucleic Acid Amplification Tests (NAATs) - Detailed
Xpert MTB/RIF (CBNAAT - Cartridge-Based NAAT)
- Sample-to-result cartridge containing all reagents
- Hemi-nested real-time PCR targeting 81-bp rifampicin resistance-determining region (rpoB gene) of M. tuberculosis complex
- 5 molecular beacon probes cover overlapping segments of rpoB; failure of any probe to bind indicates mutation at that position = rifampicin resistance
- Integrated sample processing (decontamination, DNA extraction, PCR, detection all in cartridge)
- Result in 2 hours; biosafety level 2 sufficient
- Sensitivity: 88% in smear-positive, 67% in smear-negative pulmonary TB
- Specificity: >99%
- For rifampicin resistance: sensitivity 95%, specificity 98%
- Also WHO-endorsed for CSF, lymph node, pleural fluid, gastric aspirate
- 2nd generation; 100× lower limit of detection than original Xpert
- Additional targets: IS6110 and IS1081 (higher copy number → improved sensitivity)
- Higher sensitivity in smear-negative and extrapulmonary TB, paucibacillary disease, HIV-infected
- Slightly lower specificity (1-2% false-positive rate due to dead bacilli in treated patients)
Truenat MTB / MTB Plus / MTB-RIF Dx
- Chip-based real-time micro-PCR; portable, battery-operated
- Validated for use in peripheral health facilities
- WHO-endorsed as alternative to Xpert; equivalent performance
- MTB-RIF Dx detects rifampicin resistance as a reflex test
LAMP (Loop-Mediated Isothermal Amplification)
- Isothermal amplification (no thermocycler needed; operates at 63-65°C constant temperature)
- Targets IS6110 sequence
- Sensitivity ~80%; less than Xpert; useful in resource-limited settings
- Head-to-head studies show comparable performance to Xpert in some settings (Harrison's 2025)
3.3 Line Probe Assay (LPA)
- Multiplex PCR + reverse hybridization on nitrocellulose strip
- PCR amplification of target gene → biotin-labeled PCR product → hybridizes to probes immobilized on strip → streptavidin-conjugated enzyme detection
- Detects: RIF resistance (rpoB mutations), INH resistance (katG codon 315 = high-level; inhA promoter = low-level/ethionamide cross-resistance)
- Directly on smear-positive sputum; also on culture
- Results in 5-6 hours
- Detects: Fluoroquinolone resistance (gyrA/gyrB mutations), resistance to injectable agents (rrs, eis mutations)
- Used to confirm pre-XDR/XDR-TB
3.4 Culture - The Diagnostic Gold Standard
- Fluorescence-based oxygen sensor; M. tuberculosis consumes oxygen → fluorescence released
- Positive result in 1-3 weeks (vs 4-8 weeks on LJ solid media)
- Sensitivity: detects as few as 10 bacilli/mL
- Enables complete phenotypic DST for all first and second-line drugs
- Contamination rate is higher than solid media - important quality concern
- Egg-based medium; inspissated at 85°C
- Colonies appear cream/rough ("cauliflower") in 4-8 weeks
- Slower but robust; less contamination
- Niacin test (positive for M. tuberculosis) and nitrate reduction test differentiate species
3.5 Tuberculin Skin Test (Mantoux) - Detailed
- Type IV delayed-type hypersensitivity (DTH) reaction
- PPD antigens (mixture of M. tuberculosis proteins) injected intradermally → presented to sensitized T lymphocytes (memory CD4+ T cells)
- T cells release IFN-γ, TNF → macrophage recruitment → induration (cellular infiltrate) forms at 48-72 hours
- Induration, not erythema is measured (erythema = immediate type I hypersensitivity is irrelevant)
- HIV infection, miliary TB (paradoxical - extensive disease overwhelms response)
- Severe malnutrition
- Recent measles, varicella, influenza vaccines (live vaccines suppress DTH transiently)
- Immunosuppressive therapy
- Infancy <6 months (immune immaturity)
- Very recent infection (before sensitization develops; takes 2-10 weeks)
- Improper storage/administration of PPD
- BCG vaccination (most common cause of false positive in India) - cross-reactive antigens
- NTM (non-tuberculous mycobacterial) infection
- Repeated TST (booster effect)
3.6 IGRA (Interferon-Gamma Release Assay) - Detailed
- In vitro whole blood test measuring T-cell IFN-γ secretion in response to highly specific M. tuberculosis antigens
- Key antigens: ESAT-6 (early secretory antigenic target 6) and CFP-10 (culture filtrate protein 10), both encoded by the RD1 locus
- These antigens are absent in BCG and most NTM → high specificity
- Exception: ESAT-6 present in M. kansasii, M. marinum, M. szulgai → may give false positive
| Feature | QuantiFERON-TB Gold Plus (QFT-Plus) | T-SPOT.TB |
|---|---|---|
| Format | ELISA on whole blood | ELISpot on separated PBMCs |
| Antigens | ESAT-6, CFP-10 (TB1 tube); + TB2 tube (CD8 epitopes) | ESAT-6, CFP-10 (on separate spots) |
| Readout | IFN-γ concentration (IU/mL) | Number of IFN-γ secreting T cells (spot-forming units) |
| Positive cutoff | ≥0.35 IU/mL above nil control | ≥8 spots (with ≥2× background) |
| Advantage | Single tube; automated | More sensitive in immunocompromised (counts cells, not cytokine quantity) |
- Cannot distinguish active TB from LTBI (same positive result in both) - major clinical limitation
- Does not predict who will progress from LTBI to active disease
- Reduced sensitivity in immunocompromised (HIV CD4 <200, immunosuppressive therapy) → indeterminate results
- Reproducibility issues near the quantitative threshold: spontaneous conversions/reversions on serial testing (clinically uncertain significance)
- Anti-IFN-γ autoantibodies → indeterminate result
- More expensive than TST; requires laboratory infrastructure
3.7 ADA (Adenosine Deaminase) - Mechanism
| Site | Threshold | Sensitivity | Specificity | Notes |
|---|---|---|---|---|
| Pleural fluid | >40 U/L | 92-95% | 90-95% | Most validated; helps avoid thoracoscopy |
| CSF | >10 U/L | 79% | 91% | Less reliable than pleural; useful as adjunct |
| Peritoneal fluid | >40 U/L | 100% | 95% | Ascites in peritoneal TB |
| Pericardial fluid | >40 U/L | 87% | 89% |
3.8 Latest Advances in TB Diagnostics (2024-2026)
1. Whole Genome Sequencing (WGS) / Next Generation Sequencing (NGS)
- Comprehensive DST: Detects resistance to all first and second-line drugs simultaneously from a single sequencing run - including rare mutations and novel resistance mechanisms not covered by LPA
- Transmission cluster analysis: Identifies epidemiological links between cases (strains <5 SNPs apart = likely direct transmission)
- Lineage typing: Classifies M. tuberculosis into 7 major lineages (L1-L7) with implications for virulence and drug resistance patterns
- Treatment failure prediction: Detects minority variants (heteroresistance) before they become dominant
2. Xpert MTB/XDR Assay (2021-2025 implementation)
- Detects resistance to: Isoniazid, fluoroquinolones, ethionamide, amikacin, kanamycin, capreomycin, bedaquiline, clofazimine
- Directly from sputum; result in ~80 minutes
- WHO-recommended for pre-XDR and XDR TB diagnosis
- Now being implemented in India's NTEP high-burden districts
3. Urine-Based Tests
- Detects lipoarabinomannan (LAM) antigen in urine - LAM shed into urine during active disseminated TB
- SILVAMP-LAM (newer generation): 3× more sensitive than AlereLAM; WHO-recommended for HIV-positive patients with CD4 <200 cells/μL
- Advantage: non-sputum-based; point-of-care; result in 25 minutes; no laboratory infrastructure needed
- Limitation: Low sensitivity in HIV-negative patients and non-disseminated pulmonary TB
4. Serum/Blood-Based Host Biomarkers
- Active TB patients have a highly upregulated type I IFN and neutrophil-driven transcriptional signature (RISK6 and other 3-6 gene signatures)
- Can be measured in blood by RT-PCR or gene expression profiling
- Potential for monitoring treatment response (signature normalizes with successful treatment)
- Research tool; not yet routine clinical use
5. Volatile Organic Compounds (VOC) / Breath-Based Tests
- M. tuberculosis produces specific VOCs (methyl nicotinate, naphthalene, others) detectable in exhaled breath
- Canine TB detection (trained dogs): sensitivity >90% in some studies
- Electronic nose/biosensor technologies: early-stage development
- Advantage: completely non-invasive; applicable in all ages
6. CRISPR-Cas Diagnostics
- SHERLOCK (Specific High-sensitivity Enzymatic Reporter unLOCKing) and DETECTR systems
- Combine isothermal amplification + Cas13/Cas12 nuclease activation + lateral flow readout
- Room temperature storage; single-use; 30-60 minute turnaround
- Demonstrated excellent sensitivity/specificity for M. tuberculosis and drug resistance in early studies
- Not yet WHO-endorsed; active pipeline
7. AI-Based Radiological Diagnosis
- CAD4TB, qXR, InferRead and other AI tools read chest X-rays for TB pattern recognition
- WHO-endorsed as screening tool (sensitivity 89-96%; specificity 75-89% in various studies)
- Deployed in India under NTEP 2025 on handheld X-ray devices for field-level screening
- Key limitation: Cannot confirm diagnosis; does not replace microbiological confirmation
3.9 Summary: Diagnostic Algorithm at MD Level
Presumptive TB (symptoms ≥2 weeks + risk factors)
↓
STEP 1 (Initial): CXR + Xpert MTB/RIF / Truenat (upfront NAAT)
↓
Xpert POSITIVE Xpert NEGATIVE + CXR suggestive
↓ ↓
Rifampicin Repeat Xpert on 2nd sample
sensitive? +/- Sputum culture (MGIT)
/ \ +/- Bronchoscopy + BAL
Yes No (RR-TB) ↓
↓ ↓ Clinical diagnosis if culture+
DS-TB FL-LPA (within or trial of ATT with close F/U
treatment 48 hrs)
(2HRZE/ ↓ confirms MDR?
4HR) Yes
↓
SL-LPA (gyrA/rrs)
↓
FQ-susceptible?
Yes → BPaLM 6 months
No (Pre-XDR/XDR) → BPaL 6-9 months
↓
WGS/NGS (comprehensive DST)
for complete resistance profile
Summary of Key MD-Level Points
- Phagosome arrest by LAM, ESAT-6/ESX-1, and PI3P suppression is the central early virulence mechanism of M. tuberculosis
- ESX-1 damages phagosomal membrane; ESX-3/EsxH blocks ESCRT repair - a two-hit system for cytosolic access
- Type I IFN is paradoxically harmful in TB (via cGAS-STING pathway) → immunopathology, suppresses IL-1β
- TNF-α is essential for granuloma integrity - anti-TNF therapy reactivates LTBI (25-fold risk)
- Foamy macrophage formation provides cholesterol/fatty acid nutrition to intracellular bacilli
- DosR/DevR regulon governs dormancy under hypoxic granuloma conditions - explains drug tolerance
- Rasmussen's aneurysm explains massive hemoptysis in cavitary disease
- Rich focus rupture explains TB meningitis pathogenesis; basal meningitis → vasculitis → lacunar infarcts
- IGRA superior to TST in BCG-vaccinated populations; both cannot distinguish active from latent TB
- Xpert Ultra > Xpert in smear-negative and extrapulmonary TB; slightly lower specificity
- WGS is the new gold standard for comprehensive DST; endorsed by WHO 2024
- Urine LAM (SILVAMP) for HIV+ with CD4 <200 - point-of-care, non-sputum diagnostic
- Macrophage heterogeneity (alveolar TR-AM vs monocyte-derived MoAM) is a 2025 frontier that may guide new immunotherapy strategies
- Harrison's Principles of Internal Medicine, 22nd Edition (2025) - Chapter 183 (TB Pathogenesis, Clinical Features, Diagnosis)
- Murray & Nadel's Textbook of Respiratory Medicine - Chapters 52 & 54 (Pathogenesis & Chemotherapy)
- Fishman's Pulmonary Diseases and Disorders - Chapter 130 (IGRA, TST)
- Russell DG et al., Nat Rev Immunol 2025, PMID 39774813 - Macrophage heterogeneity in TB
- Kontsevaya I et al., Clin Microbiol Infect 2024, PMID 37490968 - Update on TB diagnosis
- WHO Global TB Report 2025; NTEP India 2025 guidelines
Leptospirosis Intro Clinical features, diagnosis management md level
"leptospirosis"[MeSH Terms] AND "diagnosis" AND "treatment"
PMID: 41520794
PMID: 40457496
Leptospirosis - MD Medicine Level
PART I: INTRODUCTION
Definition
The Pathogen
- 0.1 μm wide, 6-20 μm long - coiled, highly motile spirochetes
- Two periplasmic flagella provide characteristic corkscrew motility
- Trailing end is hooked, giving the organism a question-mark shape - the basis for naming the species L. interrogans
- Visible by dark-field microscopy and silver impregnation staining; stain poorly with standard Gram stain
- Require special media (EMJH/Fletcher's medium) and weeks to months for culture growth
- 64 Leptospira species described: 17 pathogenic, 21 intermediate, 26 saprophytic (free-living)
- Serological classification (more clinically useful): >260 pathogenic serovars grouped into 26 serogroups
- Most important human pathogens: L. interrogans serogroup Icterohaemorrhagiae (rat-associated; most severe disease), Canicola (dogs), Pomona (cattle/swine), Grippotyphosa (rodents/cattle)
- Host immunity is serovar-specific (antibodies to LPS) → serovar crossing does not confer cross-protection
Epidemiology
- Predominantly tropical and subtropical, endemic in South/Southeast Asia, South America, Caribbean, Sub-Saharan Africa
- India, Brazil, Thailand, Philippines, Malaysia among highest burden countries
- In India: seasonal peaks during monsoon (July-October); major outbreak settings include floods, agricultural communities, urban slums
- Rodents (especially Rattus norvegicus - the brown rat): Primary urban reservoir; colonize renal tubules and shed Leptospira in urine chronically without becoming ill; >65% of Baltimore rats seropositive
- Other reservoirs: cattle, pigs, dogs, horses, wild animals - each serovar tends to have a preferred maintenance host
- Infected animals shed the organism for months to years without symptoms
- Indirect contact (most common): contact with water or soil contaminated with infected animal urine
- Direct contact with infected animal urine, blood, or tissues
- Entry route: abraded/macerated skin or mucous membranes (conjunctival, oral, nasal)
- Flooding dramatically increases risk - washout of animal burrows, soil contamination, high-density human-rodent contact
- Farmers, paddy field workers, sewage/sewer workers, miners, veterinarians, abattoir workers
- Military personnel operating in tropical environments
- Adventure travelers (triathlons, white-water rafting, eco-challenges - famous 2000 Eco-Challenge outbreak in Borneo, 42% attack rate)
- Urban slum dwellers during flooding
PART II: PATHOGENESIS - Molecular and Cellular Mechanisms
2.1 Entry and Dissemination (Leptospiremic Phase)
- Complement evasion: Leptospiral surface proteins bind complement regulators (Factor H, C4BP) → prevents complement-mediated killing → survival in serum
- TLR shielding: Leptospiral proteins bind LPS and peptidoglycan on their own surface → shields PAMPs from detection by TLR4/TLR2 → blunts early innate recognition
- Unusual LPS structure: Leptospira LPS has low endotoxic potency → weaker TLR4 stimulation → reduced early inflammatory response compared to gram-negative bacteria
- Motility-driven invasion: Corkscrew motility facilitates penetration through tissue barriers and endothelial cell junctions
- Liver (perisinusoidal infiltration, migration between hepatocytes)
- Kidney (tubular colonization)
- Lung (capillary injury → hemorrhage)
- Brain, meninges, CSF
- Heart
- Eyes (aqueous humor)
- Adrenal glands
2.2 Organ-Level Pathology - Mechanistic Breakdown
Liver:
- Leptospira infiltrate Disse's space (perisinusoidal) and migrate between hepatocytes
- Detachment of hepatocyte membranes from underlying structures → bile canaliculi plugging → intrahepatic cholestasis → jaundice
- Pathology: focal necrosis (NOT diffuse hepatocellular necrosis - unlike viral hepatitis); foci of inflammation; hepatocyte apoptosis
- Key point: Jaundice in Weil's disease is predominantly intrahepatic cholestatic (direct bilirubin elevated out of proportion to transaminases) - transaminases only mildly-moderately elevated (unlike viral hepatitis where transaminases can be >1000 U/L)
Kidney:
- Primary lesion: Acute tubulointerstitial nephritis (NOT glomerulonephritis)
- Leptospira colonize proximal tubular cells → tubular cell injury → decreased expression of tubular transporter proteins (Na-K-ATPase, NHE3, others)
- Proximal tubular dysfunction (Fanconi-like syndrome): impaired Na⁺ reabsorption, potassium wasting (K⁺ lost in urine despite AKI), bicarbonaturia, phosphaturia, glycosuria, magnesuria - HYPOKALEMIA despite AKI is characteristic
- Progressive → acute tubular necrosis → interstitial edema → interstitial nephritis with cellular infiltration
- Characteristically non-oliguric AKI (polyuria from tubular loss, not oliguria) in early stage - oliguria when late/severe
- Rhabdomyolysis contributes to AKI (myoglobinuria)
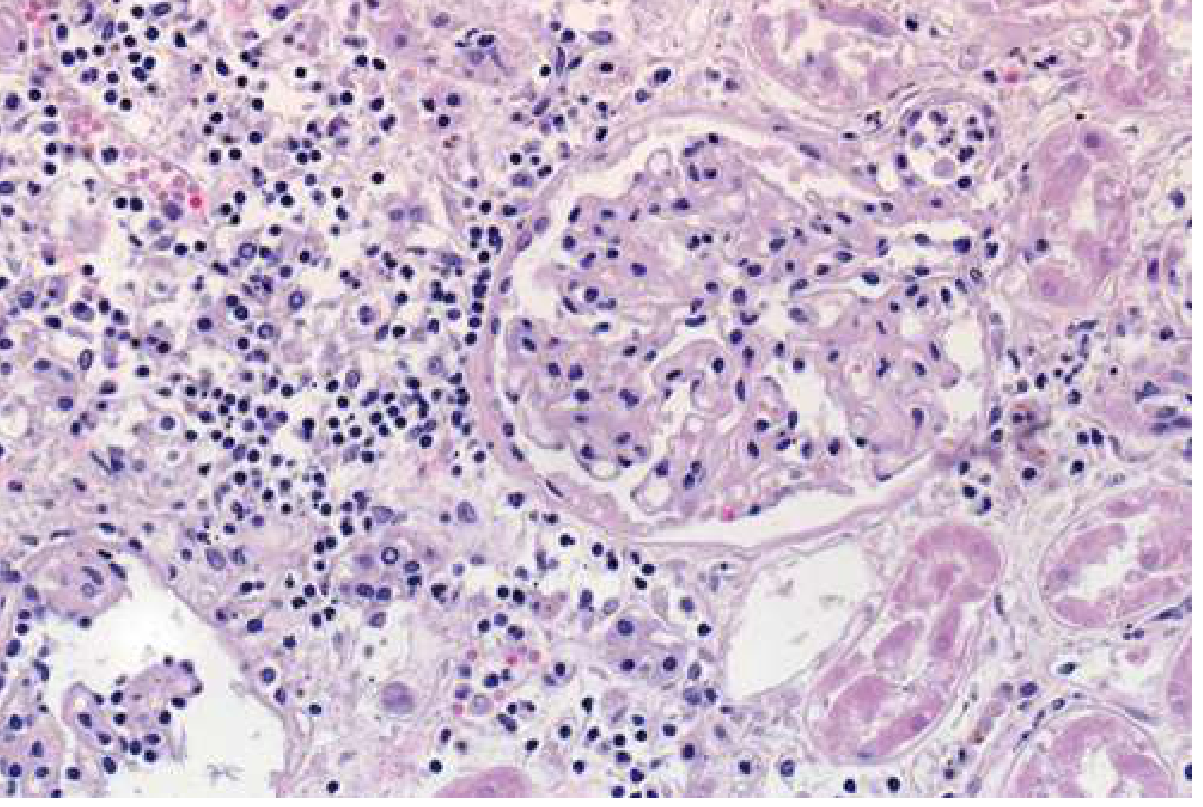
Lungs (Severe Pulmonary Hemorrhage - ARDS/HAPE-like):
- Diffuse alveolar hemorrhage is the most dangerous and increasingly recognized complication
- Mechanism: Leptospira directly damage pulmonary capillary endothelium → disruption of tight junctions → capillary leak → alveolar flooding with blood
- NOT due to coagulation failure alone - endothelial cell injury is primary
- Autoimmune mechanism: leptospiral antigens induce autoantibodies against human endothelial cells cross-reacting with Leptospira surface antigens
- CXR: bilateral alveolar opacities (hemorrhagic), sparing costophrenic angles
- CT: bilateral ground-glass opacities and airspace nodules (diffuse alveolar hemorrhage pattern)
- Mortality when ARDS/massive pulmonary hemorrhage develops: 30-70%

Hemorrhagic diathesis:
- Thrombocytopenia (immune-mediated platelet destruction + decreased production)
- Endothelial injury → disrupted hemostasis
- Coagulation disorders (elevated PT/INR, aPTT, D-dimers) - DIC-like picture but true DIC is uncommon
- Bleeding: petechiae, ecchymoses, conjunctival hemorrhages, hemoptysis, GI hemorrhage
Heart:
- Myocarditis (direct invasion + immune-mediated)
- Cardiac arrhythmias (AV block, atrial fibrillation) - portend poor prognosis
- Hypotension and cardiogenic shock in severe disease
Eyes:
- Late manifestation: uveitis (months to years after acute infection) - due to persistent Leptospira in aqueous humor; immune-mediated inflammation
2.3 The Biphasic Model of Disease
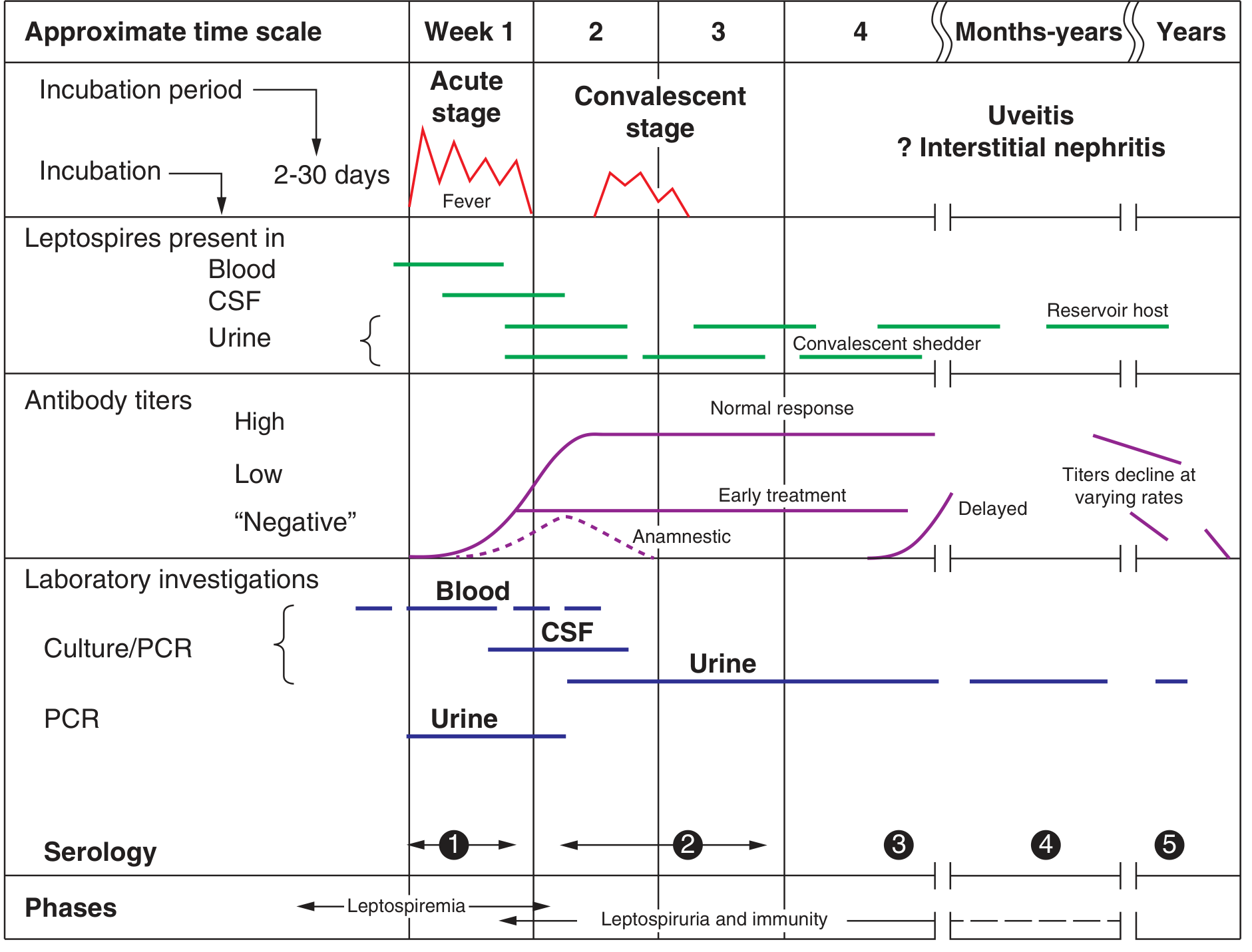
- Organisms detectable in: blood, CSF, urine (early)
- Optimal specimens for PCR and culture: blood and urine
- Serology negative (antibodies not yet formed)
- Clinical: acute febrile illness, myalgia, headache, conjunctival suffusion
- Antibodies appear → clear organisms from bloodstream
- Leptospires disappear from blood; persist in urine for weeks-months
- Serology becomes positive
- Clinical: may improve (mild disease) OR worsen with multi-organ failure (severe disease - Weil's syndrome); paradoxically the immune response itself contributes to organ injury
- Uveitis, interstitial nephritis
- Organisms still detectable in urine for months (convalescent shedding)
Key clinical implication: The threshold of early treatment - antibiotics are most effective during the leptospiremic phase (first 5-7 days). Delayed diagnosis after organ dysfunction has developed results in worse outcomes even with antibiotic initiation. - Limothai et al., J Infect 2026, PMID 41520794
PART III: CLINICAL FEATURES
3.1 Clinical Spectrum - Overview
| Severity | Presentation | Proportion | Mortality |
|---|---|---|---|
| Subclinical | Asymptomatic seroconversion | ~90% | 0% |
| Mild (anicteric) | Flu-like, self-limited | ~10% of symptomatic | <1% without treatment |
| Moderate/Weil's syndrome | Jaundice + AKI + bleeding | ~10% of symptomatic | 5-15% |
| Severe ARDS/Pulmonary Hemorrhage | ARDS, massive hemoptysis | 1-5% of symptomatic | 30-70% |
3.2 Mild (Anicteric) Leptospirosis
- High fever with chills (sudden onset)
- Intense headache: bitemporal, frontal, or retro-orbital; photophobia - closely mimics dengue fever
- Severe myalgia - characteristically calves, thighs, and lower back; muscle tenderness on palpation; may resemble rhabdomyolysis
- Nausea, vomiting, diarrhea, abdominal pain
- Non-productive cough (up to 50%)
- Conjunctival suffusion - bilateral conjunctival hyperemia/injection WITHOUT exudate or discharge. Not conjunctivitis. Due to vascular dilatation and increased permeability. One of the most reliable clinical clues.
- Pharyngeal injection
- Lymphadenopathy
- Hepatomegaly, splenomegaly
- Rash - transient, macular/maculopapular/erythematous, pretibial region particularly (resembles scrub typhus), may be petechial
- Aseptic meningitis (more common in children)
3.3 Severe Leptospirosis - Weil's Syndrome
- Jaundice (deep, direct hyperbilirubinemia; bilirubin can be markedly elevated >30 mg/dL; transaminases only mildly elevated - key distinguishing feature from viral hepatitis)
- Acute renal insufficiency (initially non-oliguric with hypokalemia; later oliguric AKI)
- Hemorrhagic manifestations (petechiae, ecchymoses, hemoptysis, GI bleeding)
- Myocarditis and arrhythmias (AV block, AF)
- Pulmonary involvement (cough, hemoptysis, ARDS)
- Hepatomegaly, splenomegaly
- Pancreatitis (serum amylase elevated)

Remember: Severe leptospirosis may be monophasic and fulminant - the neat biphasic pattern may not always be apparent.
3.4 Severe Pulmonary Hemorrhage Syndrome (SPHS)
- Sudden onset massive hemoptysis
- Bilateral diffuse alveolar hemorrhage on CXR/CT
- Rapid progression to respiratory failure
- Mechanism: direct endothelial injury + autoimmune endothelial damage
- Mortality: 30-70%
- Requires urgent ICU care and ventilatory support
3.5 Weil's Syndrome vs. Other Presentations - Differential Highlights
| Feature | Leptospirosis | Viral Hepatitis | Dengue | Malaria | Scrub Typhus |
|---|---|---|---|---|---|
| Conjunctival suffusion | +++ (hallmark) | - | - | - | - |
| Calf myalgia | +++ | + | ++ | + | + |
| Jaundice | Direct bili >> AST/ALT | AST/ALT >> bilirubin | - (rare) | + (indirect) | ± |
| Renal failure | Tubulo-interstitial (K⁺ loss) | Rare | Rare | ATN (falciparum) | ± |
| Pulmonary hemorrhage | ++ | - | - | - | - |
| Hypokalemia + AKI | Classic | - | - | - | - |
| Thrombocytopenia | ++ | + | +++ | ++ | ++ |
| Procalcitonin / CRP | Elevated | Low | Low | Elevated | Elevated |
3.6 Aseptic Meningitis in Leptospirosis
- Can occur in Phase 1 (organisms in CSF) or Phase 2 (immune-mediated)
- Clinically indistinguishable from viral meningitis
- CSF: lymphocytic pleocytosis, mildly elevated protein, normal glucose (unlike TBM/bacterial)
- Leptospira can be cultured from CSF in early disease
- Generally benign and self-resolving
3.7 Late Complications
- Uveitis: Most important late complication; occurs weeks to months post-infection; Leptospira persist in aqueous humor; immune-mediated
- Chronic interstitial nephritis: With or without chronic renal impairment
- Iridocyclitis, chorioretinitis
PART IV: DIAGNOSIS
4.1 Clinical Case Definitions (Goldman-Cecil, 2025)
- Acute febrile illness (≥38.5°C) and/or severe headache
- PLUS: myalgia, prostration, and/or conjunctival suffusion
- WITH history of exposure
- Suspect case + any 2 of: calf tenderness, cough ± hemoptysis, shortness of breath, skin rash, jaundice, hemorrhage, meningeal irritation, anuria/oliguria/proteinuria, cardiac arrhythmias
- Suspect case + positive rapid IgM + any 3 of: urinary findings (protein, WBC, blood), neutrophilia >80%, platelets <100,000/μL, elevated bilirubin >2 mg/dL
- Organism isolation from specimen, OR
- Positive PCR, OR
- Seroconversion/4-fold MAT titer rise, OR
- Single MAT titer ≥1:400 in context of clinical features
4.2 Laboratory Tests - Detailed
Routine Blood Tests
| Parameter | Finding in Leptospirosis | Mechanism |
|---|---|---|
| WBC | Leukocytosis (neutrophilic >80%) | Bacterial infection |
| Platelets | Thrombocytopenia (<100,000/μL) | Immune destruction + BM suppression |
| Bilirubin | Direct > indirect; markedly elevated (may be >30 mg/dL) | Intrahepatic cholestasis (bile duct plugging) |
| AST/ALT | Mildly elevated (rarely >200 U/L) | Focal necrosis (not diffuse) |
| ALP | May be disproportionately elevated | Cholestatic component |
| Creatinine/BUN | Elevated (AKI) | Tubulointerstitial injury |
| Serum K⁺ | Hypokalemia (despite AKI) | Tubular K⁺ wasting |
| Serum Na⁺ | May be low | Tubular Na⁺ loss + fluid shifts |
| CPK | Elevated (rhabdomyolysis) | Skeletal muscle lysis |
| PT/INR, D-dimer | Elevated | Coagulopathy |
| Procalcitonin / CRP | Elevated | Differentiates from dengue (where low) |
| Amylase/lipase | May be elevated | Pancreatitis |
- Proteinuria, hematuria, pyuria (without bacteriuria) - "active urinary sediment"
- Granular casts (tubular damage)
- Myoglobinuria if significant rhabdomyolysis
- Lymphocytic pleocytosis (10-500 cells/μL)
- Protein mildly elevated
- Glucose normal (vs TBM where low) - important differentiator
4.3 Specific Diagnostic Tests
1. PCR - Preferred Early Diagnostic Tool
| Feature | Details |
|---|---|
| Specimen | Blood (first 5-7 days); Urine (from day 7, persists weeks) |
| Sensitivity | Blood PCR: 73-95% in first week; Urine PCR: useful later |
| Specificity | >98% |
| Timing | Optimal in leptospiremic phase (before antibodies appear) |
| Advantages | Rapid; does not require viable organisms; works after antibiotics started |
| Limitation | May be negative in late disease; not universally available |
- Real-time PCR targeting 16S rRNA, lipL32, or secY genes
- PCR is the most sensitive test for early acute leptospirosis - endorsed as primary diagnostic by Goldman-Cecil 2025 and Limothai et al. 2026 (PMID 41520794)
2. Culture - Gold Standard (Rarely Used Clinically)
| Feature | Details |
|---|---|
| Media | EMJH (Ellinghausen-McCullough-Johnson-Harris) or Fletcher's semi-solid medium |
| Specimen | Blood (first 5-7 days), urine (from day 7 onward for weeks-months) |
| Time to positivity | 2 weeks to several months |
| Sensitivity | Low (~40% from blood); better from urine later |
| Use | Definitive confirmation; speciation/serogroup identification; research |
| Limitation | Too slow for clinical management; BSL-2; specialized lab required |
3. Serological Tests - Most Widely Used in Endemic Settings
- Live Leptospira serovar suspensions incubated with patient serum → microscopy to detect agglutination
- Panel includes multiple serovars from local geographic prevalence
- Positive: single titer ≥1:400 (endemic) or ≥1:800-1600 (non-endemic) OR 4-fold rise in paired sera
- Seroconversion: from negative to positive
- Limitations:
- Antibodies appear only from Day 5-7; negative in first week of illness
- Cross-reactivity between serovars (cross-agglutination)
- Early antibiotic treatment blunts antibody response → lower titers / delayed response
- Requires live organisms → BSL-3 containment; not available outside reference labs
- Cannot reliably identify infecting serovar (high cross-reactivity)
- Detects IgM antibodies (appear earlier than agglutinating antibodies)
- Lateral flow IgM assays (point-of-care) available
- Sensitivity: 50-70% in first week; 90%+ after week 2
- Specificity: 90-95%
- False positives: other spirochetal infections, malaria, dengue
- Useful as screening/triage tool in field settings
4. Dark-Field Microscopy
- Direct visualization of spirochetes in blood (first week) or urine
- NOT recommended for clinical diagnosis - very low sensitivity; high false-positive rate (platelets, fibrin threads misidentified as spirochetes); operator-dependent
- Only useful in reference/research laboratories
Summary: Diagnostic Test Choice by Disease Stage
| Disease Stage | Best Test | Specimen |
|---|---|---|
| Days 1-5 (leptospiremic) | PCR | Blood |
| Days 1-7 | Culture (if available) | Blood |
| Days 5-10 | Serology (IgM ELISA) begins to be useful | Serum |
| From Day 7 | PCR | Urine |
| Weeks 2-4+ | MAT (gold standard serology) | Serum (paired) |
| Weeks to months | Culture | Urine |
PART V: MANAGEMENT
5.1 General Principles
- Do not wait for laboratory confirmation before starting antibiotics - treat on clinical/epidemiologic suspicion
- Early treatment (during leptospiremic phase) prevents progression to multi-organ failure
- Antibiotics reduce duration of illness, leptospiruria, and urinary shedding
- Whether antibiotics reduce mortality in severe disease is debated but generally recommended
5.2 Antibiotic Treatment
| Severity | Drug of Choice | Alternative | Duration |
|---|---|---|---|
| Mild disease | Doxycycline 100 mg PO BD | Amoxicillin 500 mg PO TDS; Ampicillin 500 mg PO TDS; Azithromycin 500 mg OD | 7 days |
| Moderate/Severe (Weil's) | Penicillin G 1.5 MU IV every 6 hours | Ceftriaxone 1g IV OD; Cefotaxime 1g IV BD; Doxycycline 100 mg IV BD | 7 days |
| Pregnant women (severe) | Penicillin G IV; Ceftriaxone; Cefotaxime; Azithromycin | Avoid doxycycline | 7 days |
| Children (mild) | Amoxicillin PO | Azithromycin PO | 5-7 days |
Key point on ceftriaxone vs penicillin: Ceftriaxone 1g IV OD is as effective as penicillin for severe leptospirosis and is more convenient (once-daily dosing). Widely used in current practice.
Jarisch-Herxheimer reaction: May occur 2-6 hours after antibiotic initiation (fever spike, chills, transient hypotension) - due to mass leptospiral killing and endotoxin release. Not a sign of allergy. Manage supportively. Less severe than in relapsing fever.
5.3 Specific Organ Management
Renal Involvement:
- Early/non-oliguric AKI with hypokalemia:
- Aggressive IV fluid resuscitation - critical to prevent progression to oliguric failure
- Aggressive potassium replacement (oral and IV) - tubular K⁺ wasting can be dramatic
- Monitor urine output closely; fluid balance
- Oliguric AKI:
- Fluid restriction
- Renal replacement therapy (hemodialysis or peritoneal dialysis) - early initiation improves outcomes; most patients recover renal function with RRT support
- Indication: urea >30 mmol/L, refractory hyperkalemia, refractory acidosis, fluid overload
- Good prognostic sign: Most patients who survive the acute illness recover renal function fully
Pulmonary Hemorrhage/ARDS:
- Urgent ICU admission
- Mechanical ventilation (lung-protective strategy: low tidal volume 6 mL/kg)
- PEEP titration
- Corticosteroids - controversial; sometimes used for immune-mediated alveolar hemorrhage; not yet standardized
- Vasopressors if hemodynamic compromise
- Prone positioning if severe ARDS
- Avoid volume overload (worsens hemorrhage)
Cardiac Arrhythmias/Myocarditis:
- Continuous cardiac monitoring in all severe cases
- Manage AV block (temporary pacing if needed)
- Avoid drugs worsening arrhythmias
- Inotropes if cardiogenic shock
Bleeding/Coagulopathy:
- Platelet transfusion if <20,000/μL or active bleeding
- FFP for coagulopathy with active bleeding
- Vitamin K (if INR prolonged)
- Avoid NSAIDs (worsen platelet function + nephrotoxic)
Uveitis (late):
- Local and systemic corticosteroids (topical and oral prednisone)
- Cycloplegics
- Anti-leptospiral antibiotics (doxycycline) - may help clear aqueous humor leptospires
5.4 Predictors of Severe Disease / ICU Admission
- Dyspnoea and hypoxia
- Oliguria (vs non-oliguric AKI)
- Hypotension
- Icterus (jaundice)
- Thrombocytopenia <100,000
- AKI with rising creatinine
- Cardiac arrhythmias (AV block)
- Elevated bilirubin >30 mg/dL
- Leukocytosis >12,000
- Abnormal coagulation (PT, D-dimer)
- Emerging: microRNAs and vascular endothelium markers (research stage)
5.5 Prophylaxis
- Doxycycline 200 mg once weekly - WHO/IDSA-endorsed for occupational exposure or post-flood outbreak setting
- Shown to reduce clinical illness if given within 24-72 hours of high-risk exposure
- Cochrane review (Win et al., 2024, PMID 38483067): antibiotic prophylaxis reduces clinical leptospirosis but evidence quality is moderate; limited data on mortality reduction
- Rodent control programs
- Protective footwear, gloves for at-risk workers
- Avoid wading through floodwaters barefoot
- Vaccination:
- Human vaccines available and used in Cuba, China, France (occupational)
- Serovar-specific vaccines available in endemic countries
- No universally available broad-coverage human vaccine
- Monovalent and bivalent killed whole-cell vaccines used in India (inactivated L. interrogans serovar Icterohaemorrhagiae + Javanica)
- Recombinant outer-membrane protein-based vaccines in development
5.6 Monitoring in Severe Leptospirosis
- Urine output (target >0.5 mL/kg/hour)
- Serum electrolytes (especially K⁺, Na⁺) - twice daily in severe disease
- Serum creatinine, urea
- LFTs, bilirubin
- Platelet count, PT/INR
- Pulse oximetry / ABG
- ECG (arrhythmia surveillance)
- Daily weight (fluid balance)
Summary: High-Yield MD-Level Points
| Point | Detail |
|---|---|
| Most widespread zoonosis | ~1 million cases/year, ~60,000 deaths/year |
| Primary reservoir | Brown rat (Rattus norvegicus); serovar Icterohaemorrhagiae = most severe |
| Entry | Abraded skin or mucous membranes; NOT GI tract |
| Classic triad (Weil's) | Jaundice + AKI + Hemorrhage |
| Liver pattern | Deep jaundice (direct), mildly elevated transaminases = cholestatic (unlike viral hepatitis) |
| Renal pattern | Tubulointerstitial nephritis; HYPOKALEMIA despite AKI (tubular K⁺ wasting) |
| Pathognomonic sign | Conjunctival suffusion (injection without discharge) |
| Deadliest complication | Diffuse alveolar hemorrhage (ARDS) - 30-70% mortality |
| Early best test | PCR on blood (first 5-7 days) |
| Late best test | MAT serology (weeks 2+); paired sera |
| Serology in week 1 | Usually negative - do not rely on it for early diagnosis |
| Key biochemical clue | High bilirubin + mild AST/ALT + hypokalemia + thrombocytopenia |
| Mild treatment | Doxycycline 100 mg BD × 7 days |
| Severe treatment | Penicillin G or Ceftriaxone IV × 7 days |
| Critical management | Aggressive K⁺ replacement; early RRT for oliguria; protective ventilation for ARDS |
| Prophylaxis | Doxycycline 200 mg weekly for occupational/post-flood exposure |
- Harrison's Principles of Internal Medicine, 22nd Edition (2025) - Chapter 189: Leptospirosis (Goeijenbier, Wagenaar)
- Goldman-Cecil Medicine, 27th Edition (2025) - Chapter 298: Leptospirosis (Haake)
- Brenner & Rector's The Kidney, 2-Volume Set - Chapter on Tropical Nephrology
- Comprehensive Clinical Nephrology, 7th Edition
- Limothai U et al., J Infect 2026, PMID 41520794 - Early diagnosis and treatment; optimal therapeutic window
- Wickramasinghe M et al., Eur J Med Res 2025, PMID 40457496 - Predictors of severe leptospirosis
- Win TZ et al., Cochrane Database Syst Rev 2024, PMID 38483067 - Antibiotic prophylaxis for leptospirosis (Cochrane review)
Mitral stenosis Clinical features Pathogenesis Diagnostic Clinical and investigation As per md level for case discussion and theory
"mitral stenosis"[MeSH Terms] AND "management"
"mitral stenosis"[MeSH Terms] AND "percutaneous mitral commissurotomy"
"mitral stenosis"[MeSH Terms] AND "balloon valvuloplasty"