PRES EClampsiq
Reading File
Finding Sources
Finding Sources
Searching PubMed
"posterior reversible encephalopathy syndrome" AND eclampsia
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
PRES posterior reversible encephalopathy syndrome MRI eclampsia
Finding Sources
Reading File
I now have all the key information needed for a comprehensive answer. Let me compile it.
PRES in Eclampsia (Posterior Reversible Encephalopathy Syndrome)
Definition & Overview
PRES (also known as reversible posterior leukoencephalopathy syndrome, RPLS) is a clinico-radiological syndrome of vasogenic cerebral edema that is a well-recognized complication of preeclampsia-eclampsia. It results from vascular endothelial dysfunction and breakdown of cerebral autoregulation.
"PRES is thought to be due to abnormal cerebral vascular autoregulation resulting in vasogenic edema." — Bradley and Daroff's Neurology in Clinical Practice
Pathophysiology
There are two interrelated mechanisms:
1. Loss of Cerebral Autoregulation (Hyperperfusion Theory)
- Severe, sudden hypertension overwhelms the brain's ability to autoregulate blood flow
- Forced vasodilation → hyperperfusion → fluid extravasation into the interstitium
- Results in vasogenic edema — predominantly in posterior (parieto-occipital) white matter
- The posterior circulation is more susceptible because it has less adrenergic innervation
2. Endothelial Dysfunction (Vasospasm Theory)
- In eclampsia, circulating anti-angiogenic factors (e.g., sFlt-1) and endothelial activation cause endothelial injury
- Damage to capillary endothelial tight junctions → fluid extravasation
- Vasodilatation and vasogenic edema occur
- This is analogous to the mechanism seen with calcineurin inhibitors (tacrolimus, cyclosporine)
Clinical Features (Classic Tetrad)
| Feature | Detail |
|---|---|
| Headache | Severe, diffuse — most common symptom |
| Visual disturbances | Blurring, visual field defects, cortical blindness (due to occipital involvement) |
| Seizures | Often generalized tonic-clonic; hallmark of eclampsia |
| Altered consciousness | Confusion → encephalopathy → coma in severe cases |
"Cortical visual deficits can occasionally be the presenting feature, others including headache and seizures." — Kanski's Clinical Ophthalmology
MRI Findings
PRES has a characteristic and diagnostic MRI appearance:
- Modality of choice: MRI with FLAIR sequence
- Signal: T2/FLAIR hyperintensities (vasogenic edema) — hypointense on T1
- Location: Predominantly parietal and occipital lobe white matter, bilateral and roughly symmetric
- Gray matter (cortex, basal ganglia) can also be involved
- Frontal and temporal lobes may be affected in atypical/severe cases
- DWI: Typically shows no diffusion restriction (distinguishing vasogenic from cytotoxic/ischemic edema) — though areas of true infarction may show restriction in severe cases
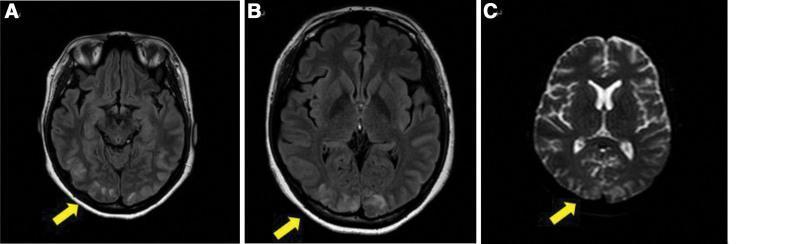
T2/FLAIR axial MRI: bilateral hyperintensities in parieto-occipital regions representing vasogenic edema in a patient with preeclampsia/eclampsia. Yellow arrows indicate the characteristic posterior distribution.
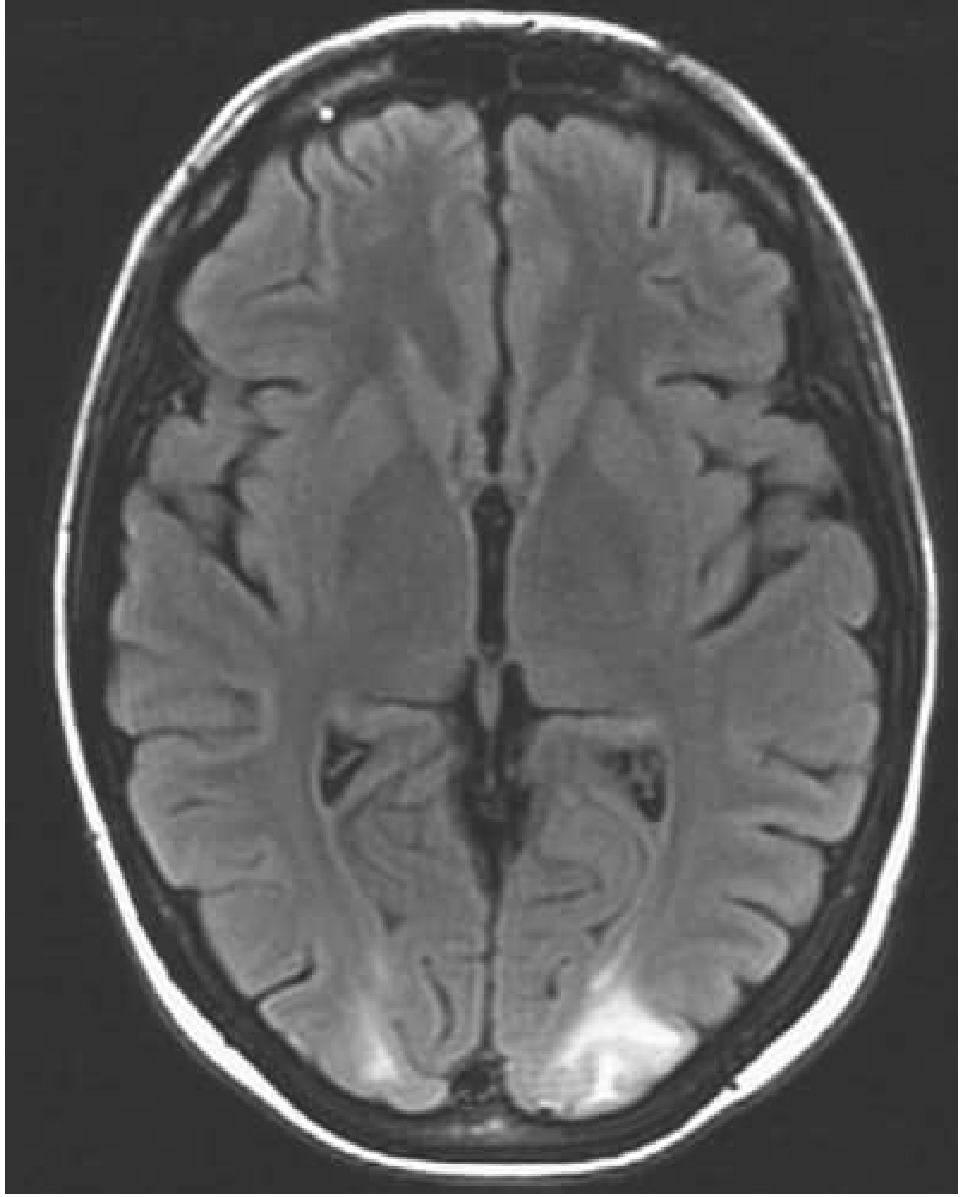
Axial FLAIR: hyperintense signal in bilateral occipital subcortical white matter (left > right) in a patient presenting with hypertension, visual changes, and seizure.
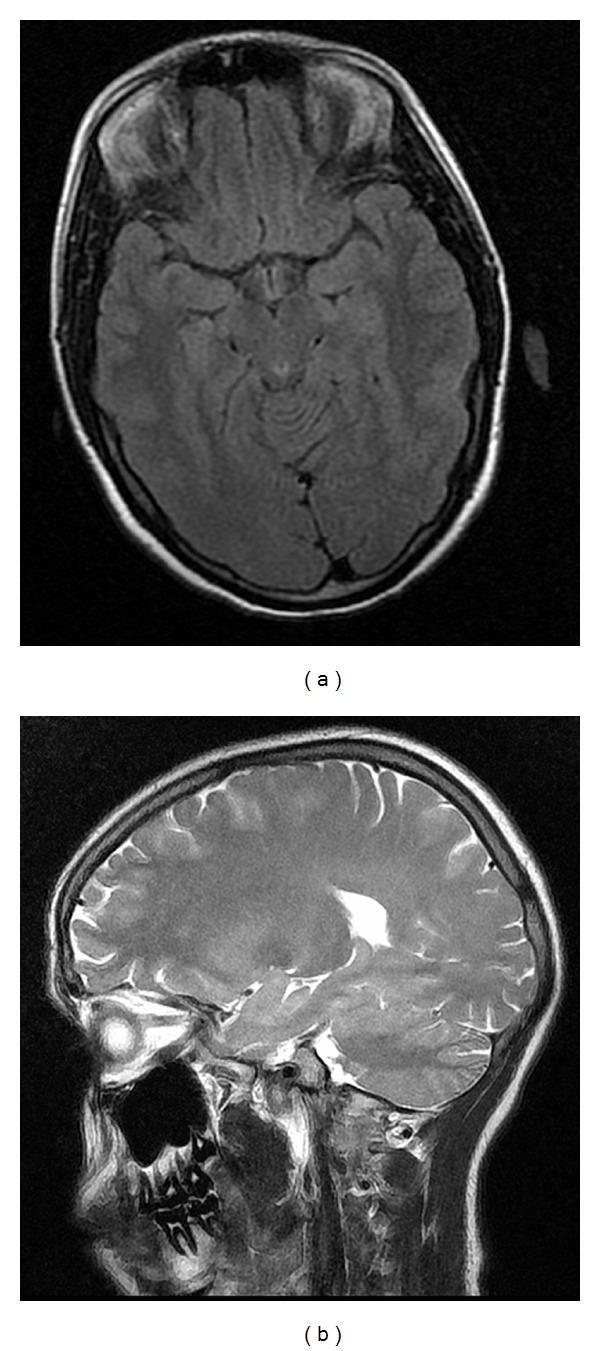
Follow-up MRI 1 month after treatment for PRES associated with eclampsia and HELLP syndrome — complete radiological resolution, demonstrating the "reversible" nature of the condition.
Diagnosis
- Clinical + MRI confirmation
- CT may show cerebral edema but is less sensitive than MRI
- Lumbar puncture: not routinely required; may show elevated opening pressure
- Blood work: assess for HELLP (CBC, LFTs, LDH), renal function, proteinuria
- Exclude stroke (DWI positive) and other encephalopathies
Association with Eclampsia
- PRES is found in a significant proportion of women with severe preeclampsia and eclampsia
- The pathophysiology overlaps: both involve endothelial dysfunction and disrupted cerebral autoregulation
- Postpartum eclampsia accounts for ~25% of eclamptic seizures and can occur up to 8 weeks postpartum, even without preceding hypertension — PRES must be considered in this window
- Long-term: women with preeclampsia have more white matter lesions and are more likely to report cognitive dysfunction compared to normotensive pregnancies
- Severe cases can progress to cytotoxic edema and infarction (irreversible injury)
Management
Definitive Treatment
Delivery of the fetus (and placenta) is the only cure for eclampsia-associated PRES.
Seizure Control
| Drug | Role |
|---|---|
| Magnesium sulfate | Drug of choice — more effective than phenytoin in preventing recurrence; reduces maternal death; benefits the neonate (fewer NICU admissions) |
| Benzodiazepines | Acute seizure termination if actively seizing |
| Phenytoin/levetiracetam | Second-line; used if Mg contraindicated |
"Magnesium is the therapy of choice to treat acute eclamptic seizures and prevent recurrence. It is more effective and has a better safety profile than phenytoin." — Rosen's Emergency Medicine
Blood Pressure Control
- Target: reduce BP by no more than 25% in the first hour, then gradually to ~160/105 mmHg
- Agents: labetalol (IV), hydralazine (IV), nifedipine (oral)
- Avoid nitroprusside in pregnancy (fetal cyanide toxicity)
General Supportive Care
- Airway management, O₂ supplementation
- Continuous fetal monitoring (>24 weeks)
- ICU-level monitoring in severe cases
Prognosis & Reversibility
- With prompt treatment, imaging and clinical findings typically resolve (the "R" in PRES)
- Irreversible infarction can occur if treatment is delayed or hypertension is extreme
- The name changed from "reversible posterior leukoencephalopathy" because gray matter involvement and frontal/temporal extension are recognized
Differential Diagnosis
| Condition | Key Distinction |
|---|---|
| Ischemic stroke | DWI positive (restricted diffusion), not bilateral/symmetric |
| Cerebral venous thrombosis | Venous phase CTA/MRV; often frontal/parasagittal; prothrombotic setting |
| Hypertensive encephalopathy (non-obstetric) | Similar imaging; no pregnancy context |
| Herpes encephalitis | Temporal lobe predominant; CSF PCR positive |
| ADEM | White matter lesions with different distribution; often post-infectious |
Sources:
- Creasy & Resnik's Maternal-Fetal Medicine, 8th ed. — Chapter 45
- Bradley and Daroff's Neurology in Clinical Practice — Chapter 40
- Rosen's Emergency Medicine — Chapter 88
- Kanski's Clinical Ophthalmology, 10th ed. — Chapter on neuro-ophthalmology
This is a shared conversation. Sign in to Orris to start your own chat.