Adenoid tonsillectomy surgery
Reading File
Finding Sources
Finding Sources
Searching the Web
adenotonsillectomy surgical technique indications complications 2024
Reading File
Reading File
Searching PubMed
tonsillectomy adenoidectomy techniques outcomes
Reading File
Finding Sources
I now have comprehensive information from Cummings Otolaryngology and Scott-Brown's. Let me compile a thorough response.
Adenotonsillectomy (Adenoid Tonsillectomy)
Adenotonsillectomy (T&A) is the combined surgical removal of the palatine tonsils and pharyngeal tonsil (adenoids). It is one of the most frequently performed surgical procedures in children, with over half a million tonsillectomies performed annually in children under 15 in the United States alone.
Anatomy
- Palatine tonsils: Paired lymphoid masses in the oropharynx, between the anterior (palatoglossal) and posterior (palatopharyngeal) pillars
- Adenoids (pharyngeal tonsil): Single lymphoid mass on the posterior nasopharyngeal wall; forms part of Waldeyer's ring along with the lingual tonsil and tubal tonsils
- Both have peak size in childhood (ages 4-7) and undergo physiological involution after puberty
Indications
Tonsillectomy Indications
1. Recurrent tonsillitis (Paradise Criteria):
- ≥7 documented episodes in the preceding year, OR
- ≥5 episodes per year for 2 consecutive years, OR
- ≥3 episodes per year for 3 consecutive years
- Each episode should include one or more: fever (>38.3°C), cervical lymphadenopathy, tonsillar exudate, or positive Group A strep culture
2. Obstructive Sleep Disordered Breathing (SDB) / Obstructive Sleep Apnea (OSA): The first-line treatment for OSA in otherwise healthy children with tonsillar/adenoid enlargement
3. Peritonsillar abscess - especially recurrent
4. Suspected malignancy (asymmetric tonsillar enlargement)
5. Chronic tonsillitis unresponsive to medical management
Adenoidectomy Indications
- Adenoid hypertrophy causing nasal obstruction
- Recurrent/chronic otitis media with effusion (especially for OME-related hearing loss and grommets)
- Chronic rhinosinusitis
- Obstructive sleep-disordered breathing
- Recurrent acute otitis media
Contraindications
| Category | Examples |
|---|---|
| Absolute | Uncontrolled bleeding diathesis, active acute infection at time of surgery, velopharyngeal insufficiency (adenoidectomy) |
| Relative | Uncontrolled systemic disease (cardiac, pulmonary), submucous cleft palate (adenoidectomy), cleft palate repair history |
| Timing | Active throat infection - defer 2-4 weeks |
Surgical Techniques
Tonsillectomy Techniques
1. Cold Dissection (Traditional)
- Tonsil grasped, anterior pillar incised
- Capsule dissected off pharyngeal constrictors using blunt and sharp dissection
- Hemostasis by suture ligation or cautery
- Gold standard for minimizing thermal injury; higher intraoperative bleeding risk
2. Monopolar Electrocautery
- Most popular technique over the past 2-3 decades
- Affords greater hemostasis during dissection
- Associated with increased postoperative pain and longer healing times
3. Bipolar Cautery
- More precise coagulation, less surrounding tissue injury
- Can be performed with operating microscope using bipolar bayonet forceps or bipolar scissors
4. Coblation (Plasma Excision)
- Radiofrequency energy conducted through saline creates plasma field of active protons that break molecular bonds
- Removes tonsillar tissue en bloc while avoiding the capsule
- Lower temperatures (~60°C vs 400°C with electrocautery) - theoretically less thermal injury
- Data on pain reduction are mixed - some studies show benefit vs. cold/electrocautery, while a Cochrane review of 9 trials found no significant differences in pain and recovery speed
5. Harmonic Scalpel
- Uses ultrasonic vibration to transfer mechanical energy to break hydrogen bonds
- Conflicting results on pain outcomes vs. standard techniques
6. Powered Intracapsular Tonsillectomy and Adenoidectomy (PITA / Microdebrider)
- Removes bulk of tonsil while preserving the tonsillar capsule as a "biologic dressing" over the pharyngeal constrictors
- Decreased thermal injury, less postoperative pain, reduced hemorrhage risk
- Two large retrospective studies (4776 and 2943 patients) found significant reductions in delayed postoperative bleeding and readmission for dehydration
- Disadvantage: potential tonsil regrowth (~6% in one study) requiring completion tonsillectomy in rare cases
Adenoidectomy Techniques
1. Curette adenoidectomy - traditional technique, blind curettage of nasopharynx
2. Electrocautery adenoidectomy - direct cauterization under nasopharyngeal mirror or endoscopic visualization
3. Microdebrider adenoidectomy - powered shaver with suction, allows precise tissue removal under endoscopic guidance, excellent hemostasis
4. Coblation adenoidectomy - radiofrequency ablation
Anesthesia Considerations
- Airway: Endotracheal tube (ETT) vs. laryngeal mask airway (LMA). ETT is more secure and easier for the surgeon to place a Boyle Davis gag; LMA is quicker to insert. Safety of airway always takes precedence
- Positioning: Supine with neck extended (Rose position); Boyle Davis gag placed to retract tongue and provide exposure
- Antiemetics: Dexamethasone and/or ondansetron significantly reduce postoperative nausea and vomiting (PONV); combination is superior to either alone
- Analgesia: Regular NSAIDs (ibuprofen) + paracetamol; opioids are now limited given FDA warnings regarding codeine in children post-tonsillectomy (CYP2D6 ultra-metabolizers risk)
Outcomes: OSA
The CHAT trial randomized 464 children aged 5-9 to adenotonsillectomy vs. watchful waiting:
- At 7-month follow-up, 79% of surgery patients had AHI <2 vs. 46% watchful waiting (p<0.001)
- Meta-analysis by Friedman et al. (23 studies, 1079 patients) found overall "cure rate" of 66.3% (AHI <1-5 per protocol); drops to 59.8% when cure = AHI <1
- Risk factors for residual SDB: age >7 years, obesity, severe OSA, chronic asthma
Quality of life: Systematic review (37 studies) demonstrates significant short-term QoL improvement post-adenotonsillectomy; long-term results are mixed.
Postoperative Complications
Intraoperative
- Bleeding
- Laryngospasm
- Aspiration of tooth, gauze, or lymphoid tissue
- Trauma to anterior/posterior pillars
Early (< 24 hours)
- Primary hemorrhage (within 24 h) - most feared; requires return to OR if significant
- PONV
- Pulmonary edema (especially in OSA patients - relief of chronic obstruction)
- Pain, odynophagia, referred otalgia
- Respiratory complications in OSA children: 16-27% rate vs. 0-1.3% general pediatric population
Late (> 24 hours)
- Secondary hemorrhage (days 5-10, peak risk) - due to sloughing of tonsillar fossa eschar
- Dehydration from poor oral intake
- Velopharyngeal insufficiency / hypernasal speech (adenoidectomy - esp. if submucous cleft present)
- Grisel's syndrome (atlantoaxial subluxation from ligamentous laxity)
- Nasopharyngeal stenosis
- Taste impairment
- Rare: Eagle syndrome, Horner's syndrome, mediastinitis, necrotizing fasciitis
Post-op Respiratory Risk Factors (OSA children)
Age <8 years, pulmonary hypertension/cardiac abnormalities, craniofacial syndromes, failure to thrive - these patients require overnight monitoring post-operatively.
Post-Operative Care
- Analgesia: Regular NSAIDs ± paracetamol; soft diet; adequate oral hydration
- No aspirin (Reye's syndrome risk in children)
- Diet: Cool soft foods for 1-2 weeks; avoid hot, spicy, crunchy foods
- Activity restriction for 2 weeks
- Return precautions: Any bright red bleeding from mouth requires immediate ER evaluation
- Typical return to normal activity: 10-14 days
Special Considerations
- Obese children: Higher rates of residual OSA (33-76%) vs. non-obese (15-37%) - often require post-operative sleep study
- Submucous cleft palate: Adenoidectomy is contraindicated due to risk of velopharyngeal insufficiency
- Adults: Higher complication rates (especially bleeding) compared to children; indications are similar but the "watchful waiting" benefit is less well-established
Sources: Cummings Otolaryngology Head and Neck Surgery; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vols 1 & 2; ASOHNS Guidelines 2024
Adenoid tonsillectomy surgery for 15 years make child anaesthetic considerations
Reading File
Finding Sources
Finding Sources
Searching the Web
anesthetic considerations adenotonsillectomy pediatric adolescent OSA airway management 2024
Finding Sources
Reading Web Page
https://wikianesthesia.org/wiki/Tonsillectomy_and/or_adenoid…
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer. Let me compile it.
Anesthetic Considerations for Adenotonsillectomy in a 15-Year-Old
At 15 years, the patient is a late adolescent - physiologically close to an adult but managed with pediatric protocols. This age group carries specific anesthetic risks around the shared airway, OSA pathophysiology, opioid sensitivity, and post-operative respiratory complications.
Pathophysiology - Why It Matters for Anesthesia
Lymphoid hyperplasia causes chronic upper airway obstruction, leading to a dangerous physiological cascade if untreated:
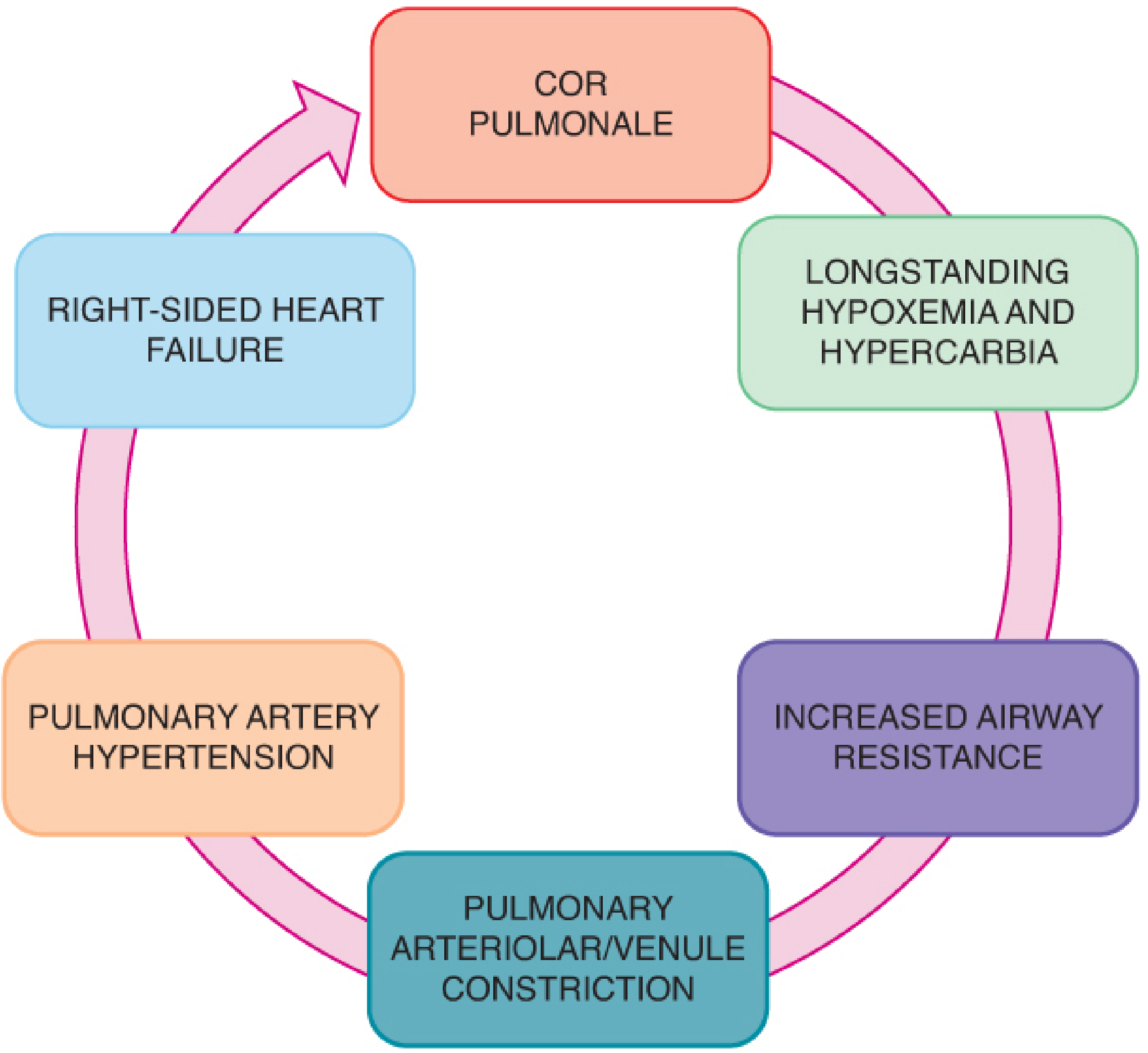
Barash, Clinical Anesthesia, 9e - Figure 48-1: Events leading to cor pulmonale
- Increased airway resistance → hypoxemia + hypercarbia → pulmonary arteriolar constriction → pulmonary hypertension → right ventricular hypertrophy → cor pulmonale
- During apneic episodes: intrapleural pressure can drop as low as -30 cm H₂O (vs. normal -2.5 to -10 cm H₂O), disrupting pulmonary capillary walls - this sets the stage for post-obstructive pulmonary edema once the airway is surgically relieved
- ECG changes (RVH) and cardiomegaly may be present in severe OSA - these are often reversible after adenotonsillectomy
1. PREOPERATIVE EVALUATION
History
- Sleep-disordered breathing: snoring, witnessed apneas, excessive daytime somnolence, mouth breathing, inattention, hyperactivity
- Use STOP-BANG (adult patients) or STBUR questionnaire (pediatric) - STBUR evaluates Snoring, Trouble Breathing, and Un-Refreshed sleep as a reliable predictor of perioperative respiratory events
- Ask about recent URIs - a fever or productive cough may be grounds for postponement
- Medication history: NSAIDs, aspirin-containing cold medications, or antihistamines - aspirin affects platelet function and must be stopped 7-10 days pre-op
Physical Examination
Look for:
- Audible respirations, obligate mouth breathing
- Elongated face, retrognathic mandible, high-arched palate - signs of chronic nasopharyngeal obstruction
- Tonsillar size assessment (Mallampati + tonsillar grading) - directly predicts ease of mask ventilation and intubation
- Chest: wheezing, rales, stridor, prolonged expiration - may indicate lower respiratory infection or partial obstruction
Tonsillar Size Classification
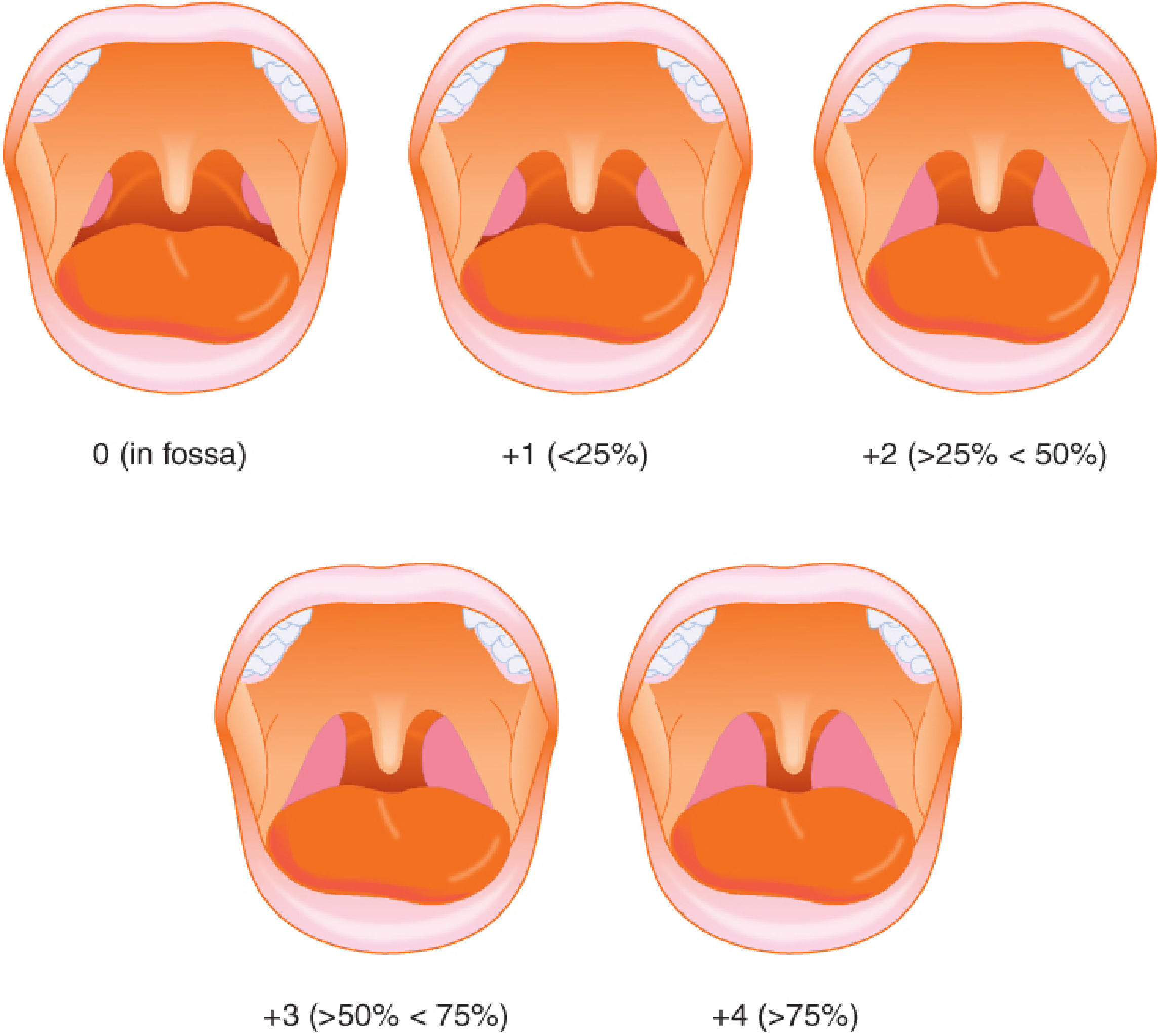
Barash, Clinical Anesthesia, 9e - Figure 48-2: Tonsillar size grading (percentage of oropharyngeal area occupied)
| Grade | Description |
|---|---|
| 0 | Tonsil within fossa |
| +1 | <25% oropharyngeal width |
| +2 | 25-50% |
| +3 | 50-75% |
| +4 | >75% - "kissing tonsils" |
Grades +3 and +4 signal potential difficult airway - anticipate challenging mask ventilation and laryngoscopy.
Investigations
- Hematocrit and coagulation profile (PT, APTT, platelet count) - routine given bleeding risk
- ECG if history suggests cor pulmonale or cardiac abnormality
- CXR only if recent pneumonia, bronchitis, or URI history
- Echocardiogram if cardiac abnormalities suspected
- Polysomnography (PSG) in complex cases: recommended by AAP when OSAS is not straightforward; assess AHI severity - guides intensity of post-op monitoring
Postpone Surgery If:
- Active acute infection / fever
- Productive cough (lower respiratory infection)
- Uncontrolled bleeding diathesis
- Incomplete workup for suspected cor pulmonale
2. PREMEDICATION
Avoid sedative premedication (benzodiazepines, opioids) in patients with OSA, very large tonsils, or intermittent obstruction - risk of respiratory depression and complete airway collapse.
- Antisialagogue (glycopyrrolate 4-6 mcg/kg IM/IV): reduces secretions in the operative field, decreases risk of laryngospasm - use this
- Anticholinergic agents may also reduce pharyngeal secretions
- If premedication is deemed essential: use minimal doses only in a monitored setting where rescue airway support is immediately available
3. AIRWAY MANAGEMENT
This is the most critical aspect - the airway is shared between surgeon and anesthesiologist.
Airway Device
- Endotracheal tube (ETT) - preferred over LMA for adenotonsillectomy
- More secure; easier for surgeon to position with Boyle-Davis mouth gag
- Protects against blood and secretion aspiration
- LMA: quicker to insert but less secure; may be acceptable for adenoidectomy alone in select cases - never compromise the airway for convenience
- Oral RAE tube or wire-reinforced (armored) tube - specifically recommended in both Miller's and Barash:
- Preformed oral RAE is taped in midline to the mandible
- Wire-reinforced tubes are less likely to kink after the mouth gag is placed
Tube Size (15-year-old)
- Near-adult sizing: typically 6.5-7.0 mm cuffed ETT (age/4 + 4 formula not applicable at 15 - use body habitus)
- Confirm correct placement and check for bilateral breath sounds after Boyle-Davis gag placement (gag can displace or kink the tube)
Difficult Airway Preparation
- Prepare video laryngoscope, multiple blade sizes, smaller tube sizes, suction
- If peritonsillar abscess is present: awake fiberoptic intubation is standard - avoid blind manipulation of friable, tense tonsillar tissue to prevent abscess rupture and purulent aspiration
- History of apnea: consider inhalational induction without paralysis until ability to ventilate is confirmed
4. INDUCTION
| Patient Profile | Recommended Approach |
|---|---|
| No IV access, cooperative | Inhalational induction (sevoflurane + O₂ ± N₂O) then IV placed |
| IV access present | IV induction with propofol (2-3 mg/kg) |
| Severe OSA / morbid obesity | IV induction + short-acting muscle relaxant + rapid airway control |
| Suspected difficult airway | Inhalational induction maintaining spontaneous respiration until intubation confirmed |
- Sevoflurane is standard volatile agent for inhalational induction - pleasant odor, rapid onset
- Glycopyrrolate given after IV placement to reduce secretions
- Muscle relaxant: short-acting non-depolarizing agent (rocuronium, mivacurium) or suxamethonium preferred - allows rapid return of neuromuscular function
- Many clinicians eliminate NMB in favor of deep inhalational anesthesia alone to maintain spontaneous ventilation during intubation
5. MAINTENANCE
- Volatile agent (sevoflurane or desflurane) in O₂
- Lower FiO₂ (avoid high-concentration O₂) - reduces risk of airway fire during surgical use of electrocautery (shared airway with ignition source)
- N₂O: used by some; avoid if significant bleeding anticipated
- TIVA (Propofol infusion): an alternative, especially in OSA - avoids volatile agent respiratory depression, faster clear-headed emergence
- Surgical position: Rose position - supine with neck extended, slight head-up tilt
Throat Pack
- Surgeon may place a moist throat pack to prevent blood from entering the trachea
- Critical: must be removed and accounted for before extubation - wrong-site retention is a sentinel event
Intraoperative Monitoring
- Standard: SpO₂, ETCO₂, ECG, NIBP, temperature
- Capnography - essential; confirms tube placement and monitors ventilation during shared-airway surgery
- Watch for sudden ETCO₂ changes - may indicate tube displacement or kinking from gag
6. ANALGESIA
Multimodal Approach (Avoid or Minimize Opioids)
| Drug | Dose / Notes |
|---|---|
| IV paracetamol (acetaminophen) | 15 mg/kg IV intraoperatively; regular post-op |
| Ketorolac or ibuprofen | Ketorolac 0.5 mg/kg IV intraop; regular oral ibuprofen post-op |
| Dexamethasone | 0.15-0.5 mg/kg IV (also antiemetic) - reduces post-op pain and swelling |
| Local infiltration | Surgeons may inject tonsillar fossae with bupivacaine ± adrenaline |
| Opioids | Use sparingly - fentanyl 1-2 mcg/kg for breakthrough; avoid codeine (FDA Black Box Warning in children - CYP2D6 ultra-metabolizers risk) |
- No aspirin post-operatively - platelet dysfunction increases secondary hemorrhage risk + Reye's syndrome risk
7. EMERGENCE
Goals: rapid, smooth, awake emergence with intact protective airway reflexes.
Steps Before Extubation
- Surgeon confirms complete hemostasis
- Remove throat pack (if placed) and document removal
- Turn patient lateral (tonsil position / recovery position) or head-down
- Gentle pharyngeal suctioning under direct vision - remove blood clots and secretions
- Gastric suctioning with orogastric tube - blood swallowed during surgery causes nausea/vomiting
Awake vs. Deep Extubation
- Awake extubation is generally preferred for adenotonsillectomy to protect against aspiration of blood
- Deep extubation reduces laryngospasm and avoids dislodging blood clots with coughing - but aspiration risk is higher
- Attenuate coughing/bucking with: IV lidocaine 1.5 mg/kg (given 90s before extubation) or light remifentanil infusion during emergence (Miller's recommendation)
- Extubate in lateral/semi-prone position - gravity keeps blood away from larynx
Laryngospasm Risk
- Adenotonsillectomy has an increased incidence of laryngospasm - blood and secretions in pharynx are the primary trigger
- Treatment: jaw thrust + CPAP, deepening anesthesia (propofol 0.5-1 mg/kg), suxamethonium 0.1-0.5 mg/kg IV (or 4 mg/kg IM if no IV access)
8. POST-OPERATIVE CONSIDERATIONS
Respiratory Monitoring
- 16-27% rate of post-op respiratory complications in OSA children vs. 0-1.3% in the general pediatric surgical population
- Risk factors for post-op respiratory complications:
- Age <8 years (less relevant here at 15)
- Severe OSA (AHI >10 or >5 with significant desaturations)
- Pulmonary hypertension or cardiac abnormalities
- Craniofacial syndromes
- Failure to thrive, obesity
Post-Obstructive Pulmonary Edema
- Occurs when chronic upper airway obstruction is suddenly relieved
- Mechanism: large negative intrapleural pressure (-30 cm H₂O) during obstructed breathing disrupts pulmonary capillary walls; on relief of obstruction, fluid floods into alveoli
- Treat with: supplemental O₂, CPAP/BiPAP, diuretics (furosemide), occasionally intubation
PONV Prophylaxis
- Post-op vomiting is common (blood swallowing, opioids, volatile agents)
- Dexamethasone 0.15 mg/kg IV + ondansetron 0.1 mg/kg IV - combination superior to either alone (systematic reviews confirm this)
- Avoid N₂O if PONV risk is high
Discharge and Admission Criteria
- At 15, day-case discharge is acceptable if:
- Mild or no OSA
- No intraoperative complications
- Tolerating oral fluids, pain controlled, no bleeding
- Overnight admission (or HDU) indicated if:
- Moderate-severe OSA
- Sleep apnea history
- Cardiac complications (cor pulmonale)
- Intraoperative difficulties
- Post-op desaturations in recovery
Pain Management Post-Op
- Regular oral ibuprofen + paracetamol as first line
- No oral opioids as take-home drugs (contact surgical team if breakthrough pain uncontrolled)
- Soft cool diet for 1-2 weeks
9. RE-OPERATION FOR POST-TONSILLECTOMY HEMORRHAGE
This is a life-threatening emergency requiring specific anesthetic planning:
- Resuscitate first - restore intravascular volume before induction (unless imminent airway obstruction)
- Assume full stomach - patient has swallowed significant blood
- Rapid sequence induction (RSI) with cricoid pressure - use suxamethonium or high-dose rocuronium
- Vigorous suctioning during laryngoscopy - copious oropharyngeal blood obscures view
- Reduce induction drug doses if hypovolemic - consider etomidate for hemodynamically unstable patients
- Have multiple laryngoscope sizes + video laryngoscope + smaller ETT sizes ready - previously easy intubation can become difficult with swelling and active bleeding
- A nasogastric tube to empty stomach before induction where time permits
Summary Table
| Phase | Key Action |
|---|---|
| Pre-op | OSA screening (STBUR), coagulation, avoid anxiolytics in severe OSA |
| Airway | Oral RAE/reinforced ETT; assess tonsillar grade |
| Induction | Inhalational (no IV) or IV induction; glycopyrrolate; short-acting NMB |
| Maintenance | Volatile or TIVA; lower FiO₂; confirm throat pack removed |
| Analgesia | Paracetamol + ketorolac + dexamethasone; minimize opioids; no codeine |
| Emergence | Awake extubation; lateral position; suction pharynx + stomach |
| Post-op | OSA monitoring; PONV prophylaxis; watch for hemorrhage; overnight if severe OSA |
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e; Miller's Anesthesia 10e; Barash, Cullen & Stoelting's Clinical Anesthesia 9e; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2
Ga drugs per kg bodyweight dosage
Finding Sources
Finding Sources
Searching the Web
general anesthesia drugs dosage per kg pediatric induction maintenance chart 2024
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I now have comprehensive, textbook-verified dosages. Let me compile the full drug dosage reference table specifically for a 15-year-old undergoing adenotonsillectomy.
General Anesthesia Drug Dosages (Per kg Body Weight)
Specific to a 15-year-old undergoing adenotonsillectomy - note that a 15-year-old is treated near-adult in dosing but note that teenagers may require higher propofol doses than adults (up to 5 mg/kg per Barash 9e).
INDUCTION AGENTS
| Drug | IV Dose (mg/kg) | Notes |
|---|---|---|
| Propofol | 2-3 mg/kg IV (teenagers up to 5 mg/kg) | Most widely used; causes transient apnea/hypotension; inject slowly to reduce pain on injection; higher dose needed in adolescents; cannabis users need even more |
| Ketamine | 1-2 mg/kg IV / 3-5 mg/kg IM | Useful if cardiovascular instability; maintains airway tone; causes dissociation + salivation (give with antisialagogue); avoid if large tonsils (may worsen obstruction on emergence) |
| Thiopental (Thiopentone) | 3-5 mg/kg IV | Now largely replaced by propofol; ultrashort barbiturate; good for RSI |
| Etomidate | 0.2-0.3 mg/kg IV | Use in haemodynamically unstable patients (post-tonsillectomy haemorrhage); single dose causes adrenal suppression up to 24h; painful on injection |
| Methohexital | 1-2 mg/kg IV | Rarely used; short-acting barbiturate; useful for brief procedures |
For a 15-year-old (~50 kg average):
- Propofol induction: 100-150 mg (up to 250 mg)
- Ketamine: 50-100 mg IV
- Etomidate: 10-15 mg IV
INHALATIONAL AGENTS (MAINTENANCE + INDUCTION)
| Agent | MAC (%) | Induction (inspired %) | Maintenance (%) | Notes |
|---|---|---|---|---|
| Sevoflurane | 2.0% (2.5% in children) | 6-8% | 1.5-3% | Drug of choice for inhalational induction in children - sweet odour, rapid onset; also used for maintenance |
| Desflurane | 6-7% | Not used for induction (pungent, causes coughing/laryngospasm) | 4-8% | Rapid emergence; good for longer cases; pungent odour limits mask induction |
| Isoflurane | 1.15% | Not ideal (pungent) | 1-2% | Older agent, still used for maintenance |
| Nitrous Oxide (N₂O) | 104% (adjunct only) | 50-70% | 50-70% (adjunct) | Used with volatile agent to reduce doses; avoid if high PONV risk; avoid high FiO₂ with diathermy (fire risk) |
Note on FiO₂: In adenotonsillectomy, keep FiO₂ as low as safely possible (typically 30-40%) - surgical electrocautery creates an airway fire risk in an O₂-enriched environment.
NEUROMUSCULAR BLOCKING AGENTS (NMBAs)
Depolarising
| Drug | Intubating Dose | Onset | Duration | Notes |
|---|---|---|---|---|
| Suxamethonium (Succinylcholine) | 1-1.5 mg/kg IV (2 mg/kg IM if no IV) | 60 sec | 10-15 min | Fastest onset - use for RSI and difficult airway; contraindicated in hyperkalaemia, burns, denervation, malignant hyperthermia susceptibility; causes fasciculations |
Non-Depolarising
| Drug | Intubating Dose | Maintenance | Onset | Duration |
|---|---|---|---|---|
| Rocuronium | 0.6 mg/kg IV (standard) / 1.2 mg/kg (RSI equivalent) | 0.1-0.2 mg/kg | 90-120 sec | 30-60 min |
| Vecuronium | 0.1 mg/kg IV | 0.01-0.015 mg/kg | 3-4 min | 25-40 min |
| Cisatracurium | 0.15-0.2 mg/kg IV | 0.03 mg/kg | 3-5 min | 40-60 min |
| Mivacurium | 0.2 mg/kg IV | - | 2-3 min | 15-20 min |
| Atracurium | 0.5 mg/kg IV | 0.1-0.2 mg/kg | 3-4 min | 30-45 min |
For adenotonsillectomy at 15 years (~50 kg):
- Rocuronium intubation: 30 mg (standard) or 60 mg (RSI)
- Suxamethonium: 75 mg IV
REVERSAL AGENTS
| Drug | Dose | Indication | Notes |
|---|---|---|---|
| Sugammadex | 2 mg/kg IV (moderate block) / 4 mg/kg IV (deep block) / 16 mg/kg IV (immediate reversal after 1.2 mg/kg rocuronium) | Reversal of rocuronium/vecuronium | Preferred over neostigmine; rapid, complete reversal; no muscarinic side effects |
| Neostigmine | 0.04-0.07 mg/kg IV (max 5 mg) | Reversal of non-depolarising NMB | Always give with glycopyrrolate (0.01 mg/kg) or atropine (0.02 mg/kg) to counteract muscarinic effects (bradycardia, secretions) |
| Atropine | 0.02 mg/kg IV (min 0.1 mg) | Bradycardia; with neostigmine | Avoid as sole premedication in modern practice |
| Glycopyrrolate | 0.004-0.01 mg/kg IV | With neostigmine; antisialagogue | Preferred over atropine - does not cross BBB; no CNS effects |
OPIOID ANALGESICS
| Drug | Intraoperative Dose | Post-op Dose | Notes |
|---|---|---|---|
| Fentanyl | 2-50 mcg/kg IV (anesthesia) | 0.5-1.5 mcg/kg IV (analgesia) | Short acting (30-60 min); most commonly used intraop opioid for T&A; use sparingly in OSA |
| Morphine | - | 0.05-0.15 mg/kg IV / 0.05-0.2 mg/kg IM | Longer acting (3-4 h); use cautiously post-op in OSA |
| Remifentanil | Loading: 1 mcg/kg IV / Infusion: 0.05-2 mcg/kg/min | Sedation: 0.05-0.3 mcg/kg/min | Ultra-short (offset 3-5 min); ideal for light emergence infusion; no post-op analgesia - bridge with other agents |
| Alfentanil | Loading: 8-100 mcg/kg / Infusion: 0.5-3 mcg/kg/min | - | Short acting; useful for brief procedures |
| Hydromorphone | - | 0.01-0.02 mg/kg IV / 0.02-0.04 mg/kg IM | More potent than morphine (5-7x) |
| FDA Black Box Warning - fatal respiratory depression in children who are CYP2D6 ultra-rapid metabolisers |
NON-OPIOID ANALGESICS
| Drug | Dose | Route | Notes |
|---|---|---|---|
| Paracetamol (Acetaminophen) | 15 mg/kg q6h (max 60 mg/kg/day, max 4 g/day) | IV / PO | Baseline analgesia; first line; do not exceed daily limit |
| Ibuprofen | 5-10 mg/kg q6-8h (max 40 mg/kg/day) | PO | Regular post-op; do not use if bleeding risk; most effective NSAID for tonsillectomy pain |
| Ketorolac | 0.5 mg/kg IV (max 15 mg) | IV | Single intraoperative dose; evidence for haemostasis - use with caution (risk of secondary haemorrhage - controversial) |
| Dexamethasone | 0.15-0.5 mg/kg IV (max 8-10 mg) | IV | Reduces post-op pain + swelling + PONV; give at induction; very important in T&A |
| Lidocaine | 1.5 mg/kg IV | IV (slow bolus) | Anti-cough agent before extubation (give 90 sec before); also reduces laryngospasm |
| Ketamine (sub-anaesthetic) | 0.1-0.5 mg/kg IV | IV | Low-dose as adjunct analgesic (NMDA antagonist); reduces opioid requirements |
ANTIEMETICS
| Drug | Dose | Notes |
|---|---|---|
| Ondansetron | 0.1 mg/kg IV (max 4-8 mg) | 5-HT₃ antagonist; give at end of surgery; gold standard PONV prophylaxis |
| Dexamethasone | 0.15 mg/kg IV (max 8-10 mg) | Also analgesic; give at induction; combine with ondansetron for best effect |
| Combination (ondansetron + dexamethasone) | As above | Dual prophylaxis - most strongly supported by evidence (Barash 9e); superior to either alone |
| Metoclopramide | 0.15 mg/kg IV | Dopamine antagonist; second line; extrapyramidal effects in children |
ANTICHOLINERGICS / ANTISIALAGOGUES
| Drug | Dose | Notes |
|---|---|---|
| Glycopyrrolate | 0.004-0.01 mg/kg IV (4-10 mcg/kg) | Reduces secretions in operative field; given after IV placement; does not cross BBB - preferred over atropine in children |
| Atropine | 0.01-0.02 mg/kg IV (min 0.1 mg) | Also treats bradycardia; crosses BBB - can cause central anticholinergic syndrome |
EMERGENCY / RESCUE DRUGS
| Drug | Dose | Indication |
|---|---|---|
| Suxamethonium | 1.5-2 mg/kg IV / 4 mg/kg IM | Complete laryngospasm / cannot intubate-ventilate |
| Propofol | 0.5-1 mg/kg IV | Partial laryngospasm / "deepening" |
| Epinephrine (Adrenaline) | 0.01 mg/kg IV (1:10,000) | Severe bronchospasm, anaphylaxis, cardiac arrest |
| Naloxone | 1-2 mcg/kg IV (titrate slowly) | Opioid reversal (respiratory depression post-op) - use low dose to avoid acute pain |
| Flumazenil | 0.01 mg/kg IV (max 0.2 mg/dose) | Benzodiazepine reversal |
| Labetalol | 0.25 mg/kg IV | Hypertension on laryngoscopy/emergence |
| Esmolol | 0.5 mg/kg IV bolus | Rapid heart rate control |
QUICK REFERENCE FOR A 50 kg (15-YEAR-OLD)
| Drug | Dose | Volume (standard conc.) |
|---|---|---|
| Propofol 1% | 2-3 mg/kg = 100-150 mg | 10-15 mL |
| Suxamethonium 50 mg/mL | 1.5 mg/kg = 75 mg | 1.5 mL |
| Rocuronium 10 mg/mL | 0.6 mg/kg = 30 mg | 3 mL |
| Fentanyl 50 mcg/mL | 1-2 mcg/kg = 50-100 mcg | 1-2 mL |
| Ondansetron 2 mg/mL | 0.1 mg/kg = 5 mg | 2.5 mL |
| Dexamethasone 4 mg/mL | 0.15 mg/kg = 7.5 mg | ~2 mL |
| Paracetamol IV 10 mg/mL | 15 mg/kg = 750 mg | 75 mL |
| Glycopyrrolate 0.2 mg/mL | 0.008 mg/kg = 0.4 mg | 2 mL |
| Sugammadex 200 mg/2mL | 2 mg/kg = 100 mg | 1 mL |
| Neostigmine 2.5 mg/mL | 0.05 mg/kg = 2.5 mg | 1 mL |
| Lidocaine 10 mg/mL (1%) | 1.5 mg/kg = 75 mg | 7.5 mL |
⚠️ Always verify doses against current local formulary and clinical context. Doses vary based on ASA status, comorbidities, concurrent medications, depth of block (for reversal agents), and clinical response. Obese patients: use ideal/lean body weight for most drugs. The above doses are from Morgan & Mikhail's Clinical Anesthesiology 7e, Miller's Anesthesia 10e, and Barash, Cullen & Stoelting's Clinical Anesthesia 9e.
This is a shared conversation. Sign in to Orris to start your own chat.