Labyrinthitis. Otogenic intracranial complications (meningitis. 11 meningoencephalitis, arachnoiditis, abscess of the brain and cerebellum. thrombophlebitis of the sigmoid sinus).
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the information needed to write a comprehensive response. Let me compile it:
Labyrinthitis & Otogenic Intracranial Complications
LABYRINTHITIS
Labyrinthitis is inflammation of the inner ear labyrinth (cochlea and vestibular apparatus) arising from spread of middle ear or mastoid infection. Two main forms are recognized:
Serous (Toxic) Labyrinthitis
The most common form, especially in children with acute otitis media (AOM).
Pathophysiology: Bacteria are not present within the labyrinth itself. Instead, bacterial toxins and inflammatory mediators enter through the oval window, round window, or a labyrinthine fistula. Round window membrane permeability increases during inflammation, allowing mediators to reach the labyrinth and alter ionic potentials — causing dysfunction without destroying neuroepithelium.
Clinical features:
- Unilateral dizziness (not always present)
- Mild to severe sensorineural hearing loss (SNHL)
- Symptoms are typically reversible once the inflammatory state subsides
Pathogens: Streptococcus pneumoniae, H. influenzae, M. catarrhalis
Treatment:
- Oral antibiotics directed at the infectious source
- Steroids (oral ± intratympanic) may improve hearing outcomes, though evidence is limited
- Myringotomy if middle ear infection is unresolved
- Tympanomastoidectomy if cholesteatoma is present
Suppurative (Purulent) Labyrinthitis
Uncommon in the antibiotic era. Involves direct bacterial invasion of the labyrinth.
Routes of bacterial entry:
- Subarachnoid space (via meningitis) — bacteria enter the scala tympani through the cochlear aqueduct or the internal auditory canal (IAC)
- Temporal bone osteomyelitis
- Middle ear — direct extension from AOM or COM, most often via a cholesteatomatous lateral semicircular canal fistula
In the modern era, the most common association is with cholesteatoma. Bacterial invasion is always promptly followed by total, irreversible loss of auditory and vestibular function. The oval window is a vulnerable entry point (e.g., in Mondini deformity, enlarged vestibular aqueduct, or post-stapes surgery).
Clinical features:
- Profound SNHL, frequently bilateral in meningitic labyrinthitis (2–20% of bacterial meningitis cases develop deafness; average ~10%)
- Severe vestibular dysfunction: initially brisk nystagmus toward the opposite ear, intense vertigo, pallor, diaphoresis, nausea, vomiting — subsiding over days as CNS compensates
- Fever, meningeal signs
- Evidence of OM or cholesteatoma
- Cranial neuropathies if infection spreads beyond the otic capsule
Pathogens: S. pneumoniae (most common, 20% deafness rate), H. influenzae (12%), N. meningitidis (5%); gram-negative rods and anaerobes in otogenic (cholesteatoma/COM) etiology
Diagnosis:
- Audiogram, vestibular testing
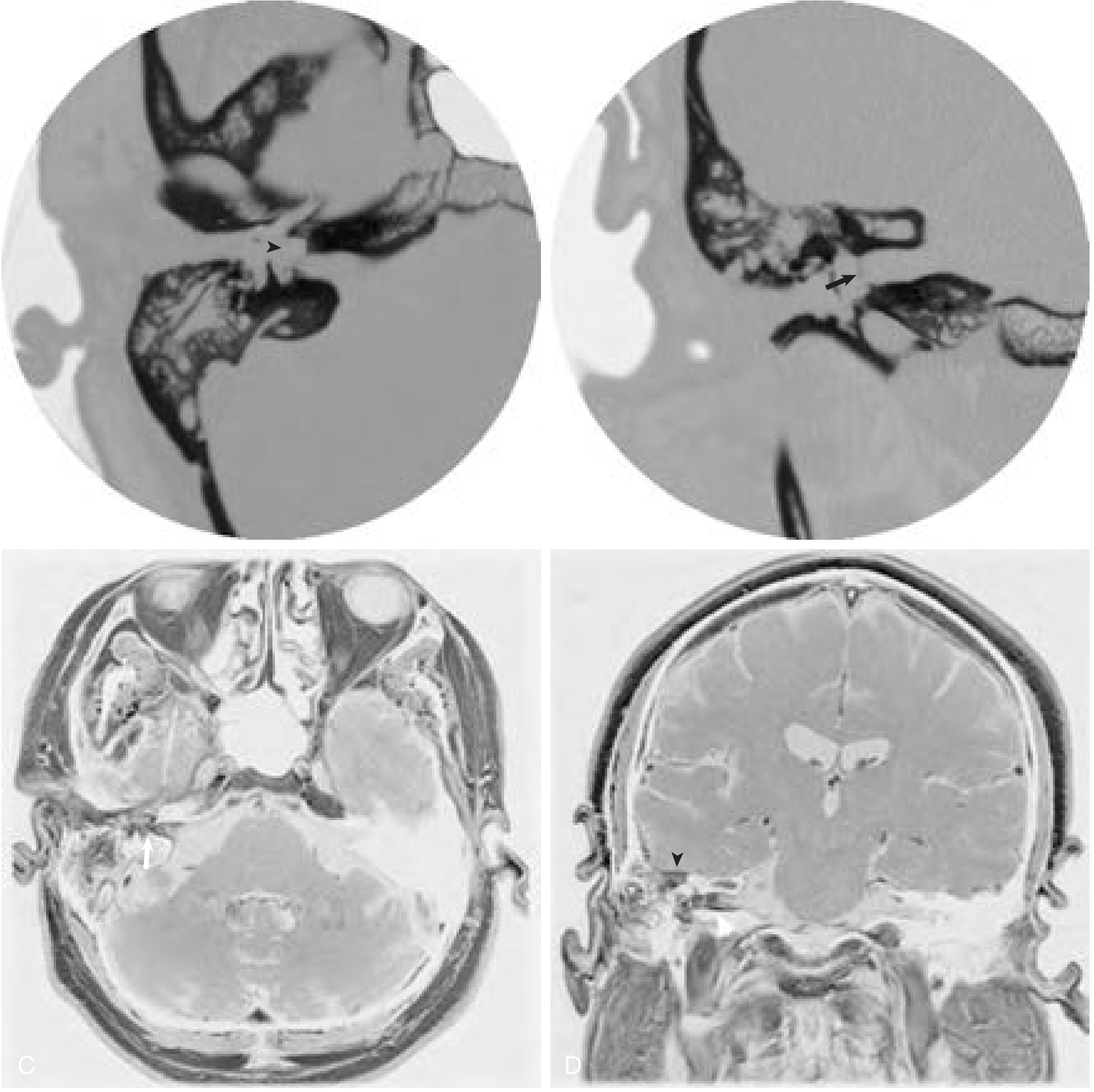
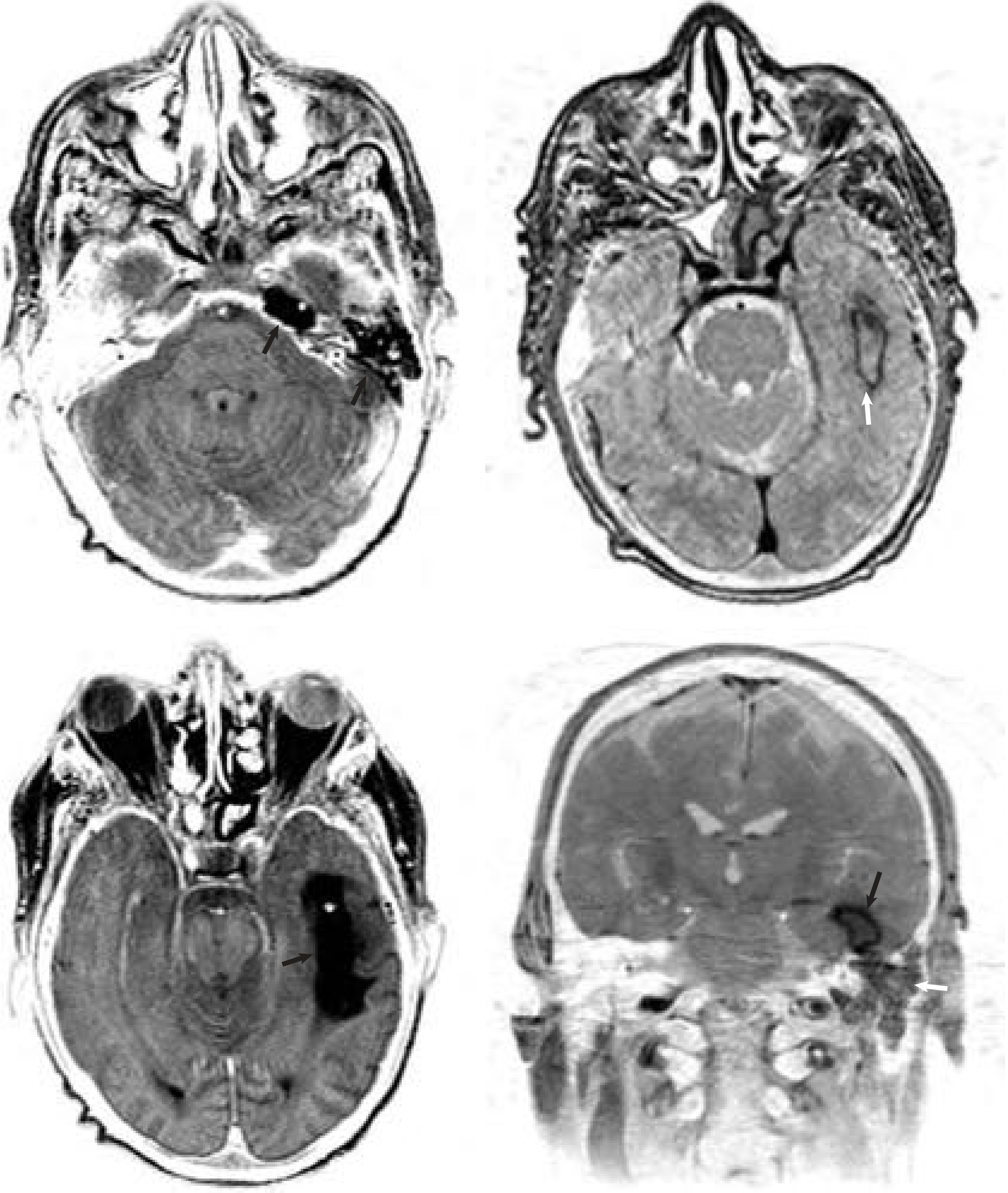
- HRCT temporal bones — evaluate for cholesteatoma, bony fistula, inner ear anomalies
- MRI — especially if intracranial complications suspected; essential for evaluating labyrinthitis ossificans (cochlear duct patency)
- Cultures via myringotomy or lumbar puncture
Treatment:
- Parenteral antibiotics with CSF penetration
- Steroids improve hearing outcomes in meningitic labyrinthitis (H. influenzae, S. pneumoniae)
- Myringotomy ± ventilation tube (non-cholesteatoma otogenic infection)
- Tympanomastoidectomy if cholesteatoma
- Serial CT/MRI for labyrinthitis ossificans — if bilateral SNHL: early cochlear implant (CI) before ossification progresses
OTOGENIC INTRACRANIAL COMPLICATIONS
These arise from spread of AOM or COM (with or without cholesteatoma) through eroded temporal bone, via bony channels (Hyrtl fissures), hematogenous spread, or retrograde thrombophlebitis.
1. Meningitis
The most common intracranial complication of otitis media.
Routes of spread:
- Hematogenous (most common)
- Direct extension via bony erosion
- Through congenital/anatomic channels (Hyrtl fissures, tegmen defects, inner ear anomalies)
- Iatrogenic (middle ear/mastoid surgery)
Clinical features:
- Generalized severe headache, photophobia, hyperesthesia
- Nausea/vomiting, fever, malaise, lethargy
- Nuchal rigidity, Kernig sign (pain on passive knee extension with thigh flexed to 90°), Brudzinski sign (passive neck flexion → involuntary thigh/knee flexion)
- Ominous signs: visual changes, seizures, ataxia, altered mental status
- 50% have additional intracranial complications on imaging
Pathogens: Same spectrum as AOM/COM; H. influenzae rare post-Hib vaccine; polymicrobial, anaerobic, gram-negative rods more common in COM
Diagnosis:
- HRCT temporal bones (evaluate mastoid/middle ear)
- CT brain (exclude abscess, mass effect, herniation before LP)
- Lumbar puncture with cultures
- Audiogram to detect SNHL
Treatment:
- Broad-spectrum IV antibiotics with CSF penetration
- Corticosteroids — shown to decrease auditory and neurologic sequelae
- If AOM: myringotomy + IV antibiotics
- If COM: mastoidectomy mandatory
- 7–10 days culture-directed IV antibiotics → 2–3 weeks oral therapy
- Monitor hearing; consider CI if bilateral SNHL with cochlear ossification
2. Meningoencephalitis / Cerebritis
An intermediate stage representing bacterial invasion of brain parenchyma before a frank abscess has formed. Characterized by focal cerebritis with edematous, inflamed brain tissue. At this stage, the condition can still be managed with IV antibiotics alone, before necrosis and capsule formation occur (see Brain Abscess below).
3. Arachnoiditis
Inflammation of the arachnoid layer, often occurring as part of the meningitic process or subdural involvement. Produces adhesions that can impair CSF flow and cause communicating hydrocephalus, cranial nerve entrapment, and local ischemia. Shares the clinical and management principles of bacterial meningitis.
4. Brain Abscess (Temporal Lobe & Cerebellar Abscess)
The second most common intracranial complication of OM after meningitis. Almost exclusively caused by COM. Two-thirds of patients have more than one concurrent intracranial complication.
Epidemiology: Predominantly males in the second decade of life; most current series come from Africa, Asia, and South America. ~75% associated with cholesteatoma. Mortality ~10%; up to 80% with intraventricular rupture.
Pathogenesis: Bacteria propagate along venous channels from mastoid into adjacent brain parenchyma → polymorphs migrate → endothelial swelling → focal cerebritis → edema, hemorrhage, necrosis → abscess with poorly-defined then firmer capsule. Abscesses are often multilocular.
Routes:
- Temporal lobe: tegmen erosion with direct extension
- Cerebellum: via thrombophlebitis; hematogenous
- Both locations nearly equally affected in otogenic cases
Three stages:
- Encephalitis — headache, fever, rigors, nausea/vomiting, mental status changes, seizures
- Quiescent (coalescent) — acute symptoms abate
- Rupture/expansion — return of acute symptoms + signs of raised ICP, meningeal signs
Focal deficits (in up to 70%):
- Cerebellar abscess: ataxia, dysmetria, dysdiadochokinesis, coarse horizontal nystagmus, action tremor
- Temporal lobe abscess: homonymous visual field defects, contralateral hemiparesis, aphasia
Diagnosis:
- Contrast-enhanced CT (evaluate mastoid bony anatomy)
- MRI brain with contrast (abscess with enhancing capsule + surrounding edema)
Pathogens: Staphylococcus aureus (most common); polymicrobial; gram-negative rods (Klebsiella, Proteus, E. coli, Pseudomonas); anaerobes (Bacteroides)
Treatment:
- Immediate broad-spectrum IV antibiotics with anaerobic coverage
- Urgent neurosurgical drainage/excision within 24 hours (when neurologically stable)
- IV steroids + anticonvulsants
- Simultaneous transtemporal aspiration + mastoidectomy increasingly described (especially for abscesses near mastoid)
- Mastoidectomy through a separate surgical field (conventional approach)
- AOM → myringotomy; COM → mastoidectomy (timing staged vs. simultaneous is debated)
5. Epidural (Extradural) Abscess
Often insidious in onset; prognosis is good when treated early. Frequently coexists with lateral sinus thrombophlebitis, meningitis, and cerebritis.
Pathogenesis: Bony erosion from cholesteatoma or coalescent mastoiditis → abscess between temporal bone and dura → intense inflammatory response → granulation tissue on dural surface → pachymeningitis (dural thickening). Can affect the middle fossa (tegmen), posterior fossa (cerebellar plate), or both.
Clinical features:
- Deep mastoid pain — the most common symptom
- No signs specific to epidural abscess; many cases discovered incidentally at surgery or on imaging
- Otherwise similar presentation to coalescent mastoiditis
Diagnosis:
- CT or MRI: fluid-filled cavity between temporal bone and enhanced dura
Treatment: Surgery is the only recommended treatment:
- Mastoidectomy with bone removal overlying the abscess
- Scrape granulation tissue from dural surface (dura is thickened; use blunt Freer elevator or large curette)
- Middle fossa abscess → limited subtemporal approach (do not remove tegmen unless eroded)
- Posterior fossa abscess → remove bony plate (no encephalocele risk)
- Consider tegmen repair if large surface exposed
- IV antibiotics postoperatively
6. Subdural Empyema
One of the most urgent neurosurgical emergencies. Mortality 5–30% even in the antibiotic era. Two-thirds occur in men in the second decade.
Pathogenesis: Purulent infection between dura and pia arachnoid — spreads rapidly through the subdural space. Causes thrombophlebitis of cortical veins → cortical swelling, necrosis, infarction. Even a thin layer of subdural pus can cause devastating raised ICP, focal deficits, and seizures.
Clinical features:
- Severe headache, malaise, chills, nuchal rigidity
- Altered mental status, focal neurological deficits
- Papilledema (raised ICP)
Diagnosis:
- CT with contrast: crescent-shaped low-density fluid collection (may be normal early)
- MRI with contrast: enhancing fluid collection in subdural space (more sensitive)
Treatment:
- Urgent neurosurgical drainage
- Broad-spectrum antibiotics until cultures obtained
7. Thrombophlebitis of the Sigmoid (Lateral) Sinus
Accounts for 17–20% of intracranial complications of OM. Forms from a perisinus abscess → intimal damage → mural thrombus → infected clot → sinus occlusion.
Pathogenesis: Bony erosion from COM/cholesteatoma (or osteothrombophlebitis in AOM) exposes the dural sinus wall. Perisinus abscess exerts pressure → necrosis of outer wall → extends to intima → fibrin, platelets, blood cells → infected mural thrombus. Propagates:
- Proximally → transverse sinus, torcular herophili, superior sagittal sinus, cavernous sinus (via inferior/superior petrosal sinus)
- Distally → internal jugular vein (IJV)
- Showers septic emboli → metastatic abscesses (lungs most common)
Clinical features (classic):
- "Picket fence" fever: diurnal temperature spikes >39.4°C (103°F) — less common in antibiotic era
- Headache, malaise, septicemia
- Griesinger sign: edema and tenderness over mastoid tip (from thrombosis of mastoid emissary vein)
- Anterior SCM tenderness
- Diplopia or other neurological signs (common modern presentation in partially treated patients)
- Complications: septic pulmonary emboli, intracranial abscess/empyema, otitic hydrocephalus (papilledema), lower cranial nerve deficits if spread to jugular foramen
Diagnosis:
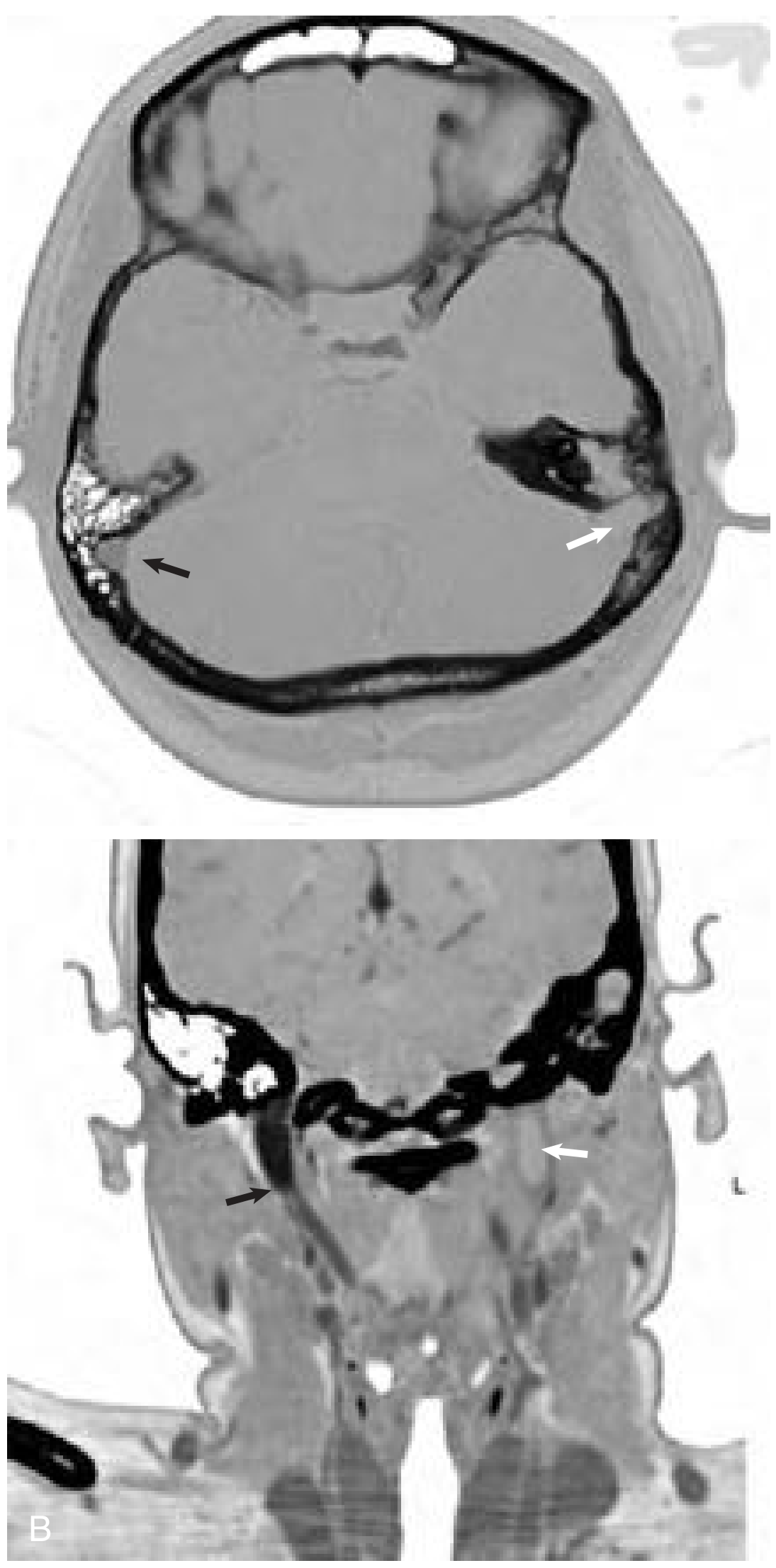
- CT brain with contrast: absent sinus enhancement + central hypodensity ("delta sign")
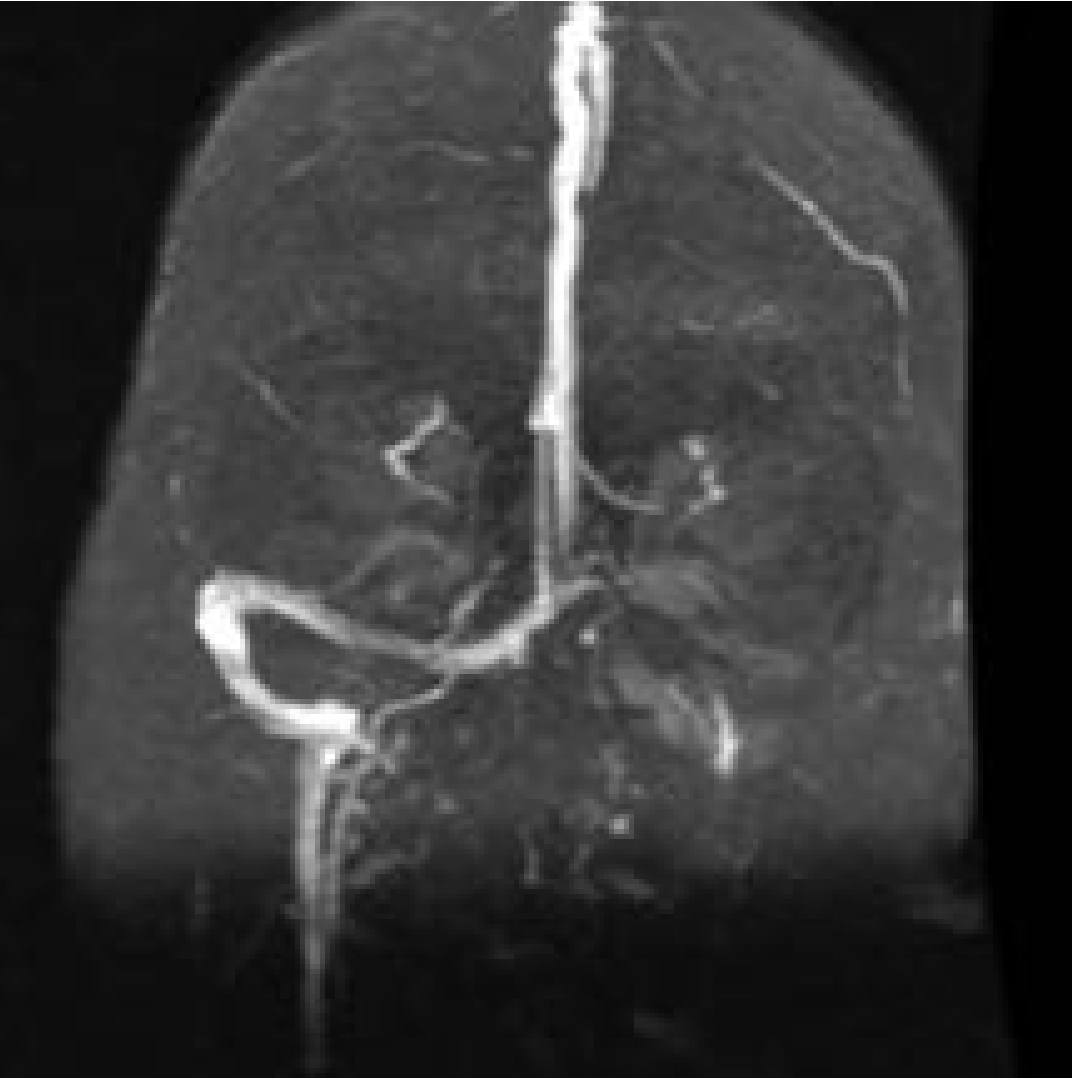
- Magnetic resonance venography (MRV): flow void in affected sinus
Treatment:
- Mastoidectomy to eradicate underlying COM/cholesteatoma (all patients)
- Broad-spectrum IV antibiotics
- Sinus management (debated):
- Needle aspiration: if blood returns → no intervention; if no blood/pus → open sinus with clot evacuation
- Recent literature: sinus likely to recanalize once surrounding infection removed
- IJV ligation only if septic emboli or clot extends into the neck
- 2-week IV antibiotics postoperatively + repeat MRI/MRV
- Anticoagulation controversial — necessary if clot extends to sagittal, transverse, or cavernous sinus
Otitic Hydrocephalus
A related complication: raised ICP with normal CSF on lumbar puncture.
Pathogenesis: Lateral sinus thrombosis → extends to confluence of sinuses → involves superior sagittal sinus → impairs CSF absorption at arachnoid villi → raised ICP.
Features: Headaches, nausea/vomiting, visual changes, lethargy, papilledema, photo/phonophobia.
Treatment: Mastoidectomy (if COM); acute ICP reduction with mannitol, acetazolamide, fluid restriction, corticosteroids; consider anticoagulation for sagittal sinus involvement; serial ophthalmological monitoring.
Summary Table
| Complication | Key Feature | Primary Investigation | Key Treatment |
|---|---|---|---|
| Serous labyrinthitis | Reversible SNHL, no bacteria in labyrinth | Audiogram, culture ME effusion | Oral ABx, steroids |
| Suppurative labyrinthitis | Total irreversible hearing/vestibular loss | HRCT + MRI temporal bones | IV ABx, mastoidectomy |
| Meningitis | Most common IC complication | LP + cultures, CT/HRCT | IV ABx + steroids, mastoidectomy (COM) |
| Epidural abscess | Deep mastoid pain, often found incidentally | CT/MRI: fluid between bone and dura | Mastoidectomy (surgery only) |
| Subdural empyema | Most urgent emergency, cortical vein thrombosis | MRI (crescent collection) | Urgent neurosurgical drainage + ABx |
| Brain abscess | 3 stages; temporal lobe or cerebellum | MRI with contrast (ring enhancement) | IV ABx + neurosurgical drainage + mastoidectomy |
| Sigmoid sinus thrombophlebitis | Picket-fence fever, Griesinger sign, septicemia | CT ("delta sign"), MRV | Mastoidectomy + IV ABx ± sinus opening |
| Otitic hydrocephalus | Raised ICP, normal CSF | MRI/MRV | ICP control, mastoidectomy |
Sources: K.J. Lee's Essential Otolaryngology, 11e; Cummings Otolaryngology Head and Neck Surgery, 7e
This is a shared conversation. Sign in to Orris to start your own chat.