Explain me 10 common heart disease with the ecg changes and ecg images of those diseases
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
ECG electrocardiogram ST elevation myocardial infarction STEMI
Searching Images
ECG atrial fibrillation irregularly irregular rhythm absent P waves
Searching Images
ECG complete heart block third degree AV block
Searching Images
ECG left ventricular hypertrophy high voltage QRS
Searching Images
ECG pulmonary embolism S1Q3T3 right heart strain
Searching Images
ECG Wolff-Parkinson-White delta wave pre-excitation
Searching Images
ECG ventricular tachycardia wide complex tachycardia
Searching Images
ECG pericarditis saddle-shaped ST elevation diffuse
Searching Images
ECG hyperkalemia peaked T waves wide QRS sine wave
Searching Images
ECG Brugada syndrome coved ST elevation right bundle branch block V1 V2
Here is a comprehensive guide to 10 common heart diseases with their ECG changes and images:
10 Common Heart Diseases — ECG Changes & Images
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
ECG Changes
- Hyperacute T waves — very early sign (tall, peaked, broad-based T waves)
- ST-segment elevation ≥1 mm in ≥2 contiguous limb leads or ≥2 mm in ≥2 contiguous precordial leads
- Reciprocal ST depression in mirror-image leads
- Pathological Q waves (>40 ms wide, >25% of R-wave height) — develop within hours, signify necrosis
- T-wave inversion in the evolving/chronic phase
Localization by leads:
| Territory | Affected Leads | Culprit Artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Inferior | II, III, aVF | RCA |
| Lateral | I, aVL, V5–V6 | LCx |
| Posterior | Tall R in V1, ST depression V1–V3 | RCA/LCx |
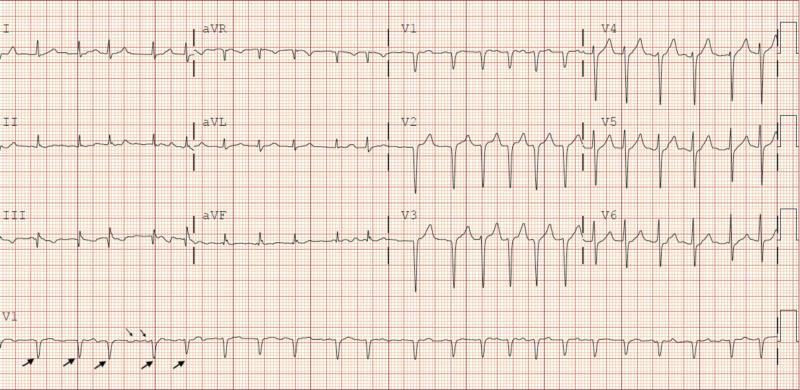
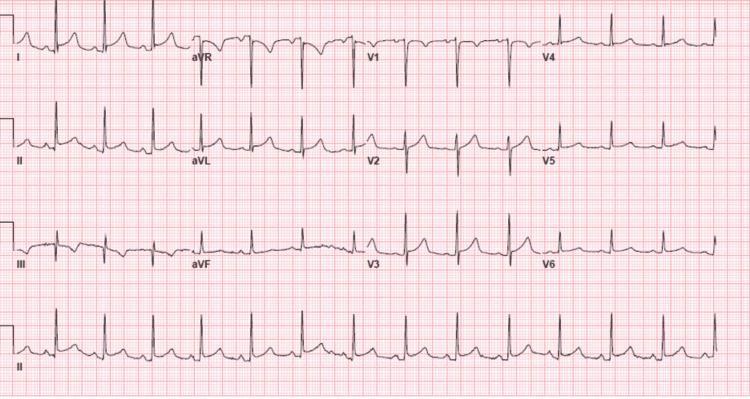
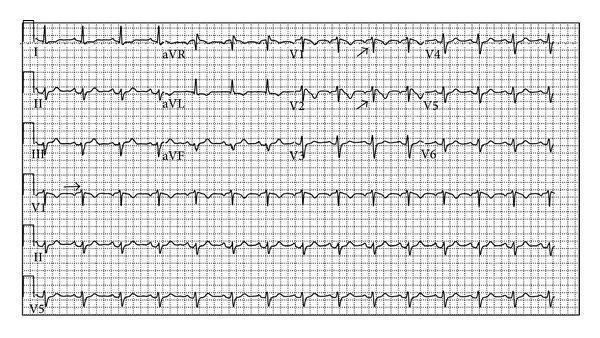
2. 💓 Atrial Fibrillation (AF)
ECG Changes
- Absent P waves — replaced by chaotic fibrillatory baseline (f waves, best seen in V1 and lead II)
- Irregularly irregular R-R intervals — hallmark finding
- Narrow QRS (unless aberrant conduction or bundle branch block present)
- Rapid ventricular response when rate is uncontrolled (>100 bpm = AF with RVR)
- Variable f-wave amplitude: coarse AF (amplitude >1 mm) vs fine AF
3. 🚫 Complete (Third-Degree) Heart Block
ECG Changes
- Complete AV dissociation — P waves and QRS complexes are totally independent
- Regular P-P intervals at atrial rate (~60–100 bpm)
- Regular, slower escape R-R intervals at ventricular rate
- Junctional escape: narrow QRS, rate ~40–60 bpm
- Ventricular escape: wide QRS (>120 ms), rate ~20–40 bpm — indicates infra-Hisian block
- No fixed PR interval — P waves "march through" QRS and T waves
- Associated with syncope (Stokes-Adams attacks)

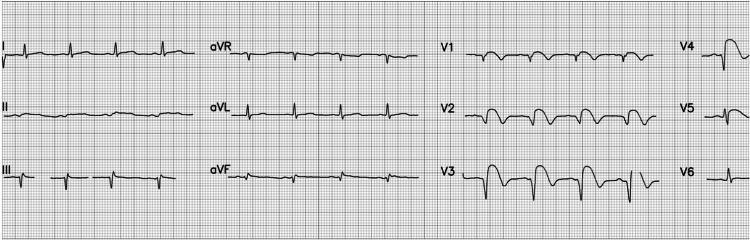
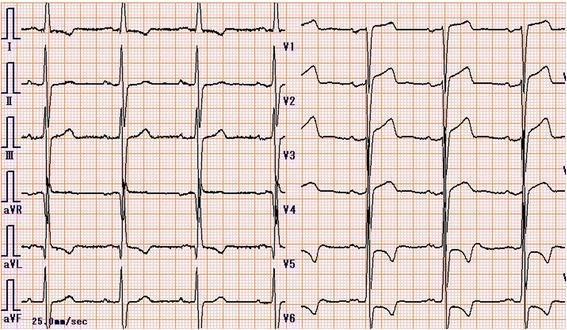
4. 📈 Left Ventricular Hypertrophy (LVH)
ECG Changes
- Voltage criteria (Sokolow-Lyon): S in V1 + R in V5 or V6 ≥35 mm
- Cornell criteria: R in aVL + S in V3 >28 mm (men) or >20 mm (women)
- Left axis deviation (axis −30° to −90°)
- ST depression and T-wave inversion in lateral leads (I, aVL, V5–V6) = "strain pattern"
- Prolonged QRS (sometimes >100 ms but not full BBB)
- Left atrial enlargement (broad, bifid P wave in II, deep negative P in V1)
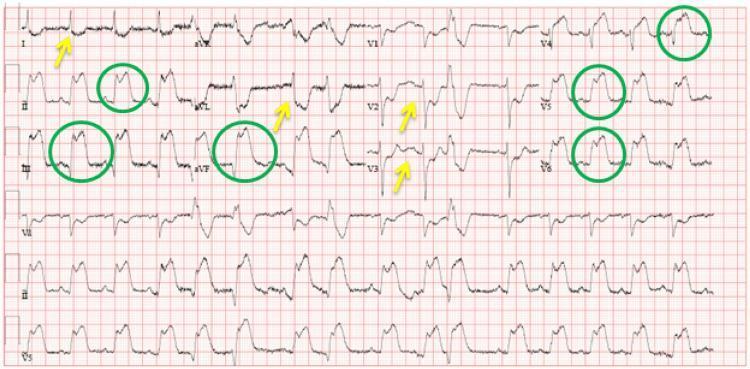
5. 🩺 Acute Pericarditis
ECG Changes (4 classic stages)
| Stage | Finding |
|---|---|
| Stage I | Diffuse concave ("saddle-shaped") ST elevation + PR depression in most leads; ST elevation + PR elevation in aVR |
| Stage II | ST returns to baseline; PR still depressed |
| Stage III | T-wave inversion (diffuse) |
| Stage IV | Normalization |
- No reciprocal ST changes (unlike STEMI — except aVR)
- Spodick's sign: downsloping TP segment
- No Q waves
- Large effusion → electrical alternans (alternating QRS amplitude)
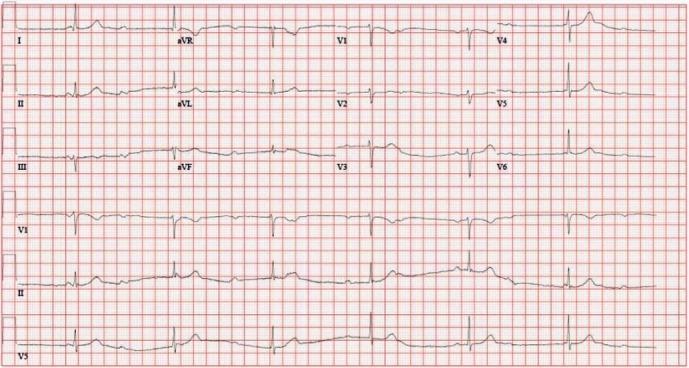
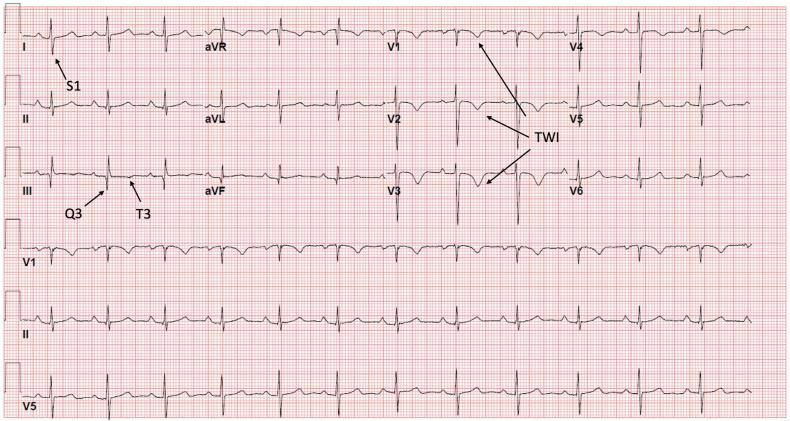
6. 🫁 Pulmonary Embolism (PE)
ECG Changes
- Sinus tachycardia — most common finding
- S₁Q₃T₃ pattern — S wave in lead I, Q wave in lead III, inverted T wave in lead III
- Right axis deviation (axis >+90°)
- Incomplete or complete RBBB (RSR' in V1)
- T-wave inversions in V1–V4 (right ventricular strain pattern)
- P pulmonale (tall, peaked P wave >2.5 mm in lead II)
- Atrial fibrillation (can be triggered)

7. ⚡ Ventricular Tachycardia (VT)
ECG Changes
- Wide QRS tachycardia (QRS ≥120 ms) at rate >100 bpm
- AV dissociation (P waves fire independently of QRS) — most specific finding
- Fusion beats — hybrid complex when normal sinus beat partially fuses with ectopic VT beat
- Capture beats — narrow complex amid wide tachycardia = pathognomonic
- Concordance across precordial leads:
- Positive concordance (all positive V1–V6) → VT
- Negative concordance (all negative) → VT
- RBBB morphology with left axis deviation or LBBB morphology with right axis deviation — favors VT over SVT with aberrancy
- Brugada algorithm (any of 4 criteria positive → VT)

8. 🔑 Wolff-Parkinson-White (WPW) Syndrome
ECG Changes (during sinus rhythm)
- Short PR interval (<120 ms) — due to bypass of AV node
- Delta wave — slurred upstroke at start of QRS (pre-excitation via accessory pathway)
- Wide QRS complex (>120 ms) — delta wave + normal QRS fused
- Secondary ST-T changes — discordant to delta wave
- Pseudo-infarct Q waves — negative delta waves in inferior leads mimicking inferior MI
- During orthodromic AVRT: narrow complex tachycardia (delta waves disappear)
- During antidromic AVRT or AF with WPW: very wide, irregular, fast (can be lethal)

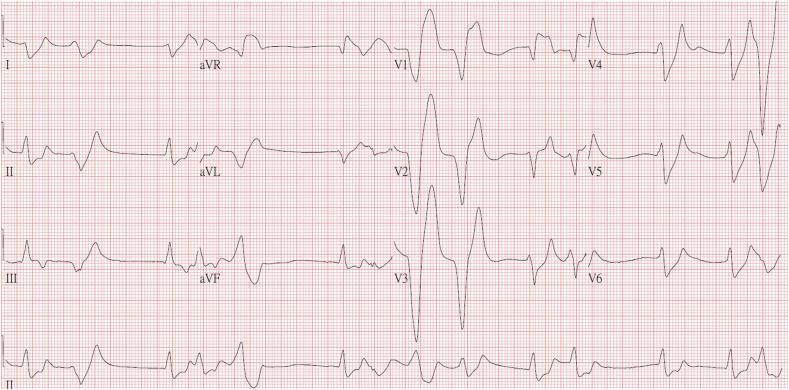
9. 🧪 Hyperkalemia
ECG Changes (progressive with rising K⁺)
| Serum K⁺ | ECG Finding |
|---|---|
| 5.5–6.5 mEq/L | Tall, peaked, narrow-based ("tented") T waves |
| 6.5–7.5 mEq/L | PR prolongation, P-wave flattening, QRS widening |
| 7.5–8.5 mEq/L | P waves disappear (sinoventricular rhythm), further QRS widening |
| >8.5 mEq/L | Sine-wave pattern (QRS and T merge) → VF or asystole |
- Peaked T waves most prominent in V2–V5
- No specific lead distribution (global effect)

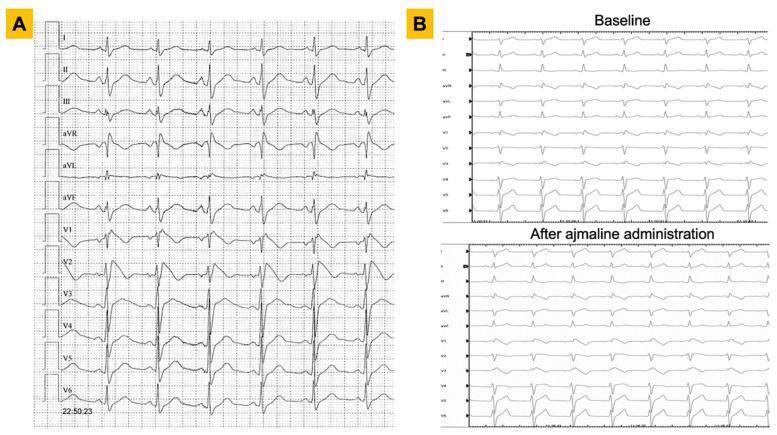
10. 🧬 Brugada Syndrome
ECG Changes
- Type 1 (diagnostic) — "coved" ST elevation ≥2 mm in V1–V2 (placed in 2nd, 3rd, or 4th intercostal space) descending into inverted T wave, without return to baseline
- Type 2 — "saddle-back" ST elevation with positive/biphasic T wave (not diagnostic alone)
- Incomplete RBBB morphology often present
- Fever, sodium channel blockers (ajmaline, flecainide) can unmask the pattern
- Normal baseline ECG possible — provocation testing may be required
- Associated with ventricular fibrillation and sudden cardiac death in young males, often during sleep
Quick Reference Summary Table
| # | Disease | Key ECG Finding |
|---|---|---|
| 1 | STEMI | ST elevation + reciprocal changes + Q waves |
| 2 | Atrial Fibrillation | No P waves, irregularly irregular rhythm |
| 3 | Complete Heart Block | AV dissociation, slow escape rhythm |
| 4 | LVH | High voltage, left axis, lateral strain pattern |
| 5 | Pericarditis | Diffuse saddle ST elevation, PR depression |
| 6 | Pulmonary Embolism | S₁Q₃T₃, sinus tachycardia, RBBB, RV strain |
| 7 | Ventricular Tachycardia | Wide QRS tachycardia, AV dissociation |
| 8 | WPW Syndrome | Short PR, delta wave, wide QRS |
| 9 | Hyperkalemia | Peaked T waves → sine wave pattern |
| 10 | Brugada Syndrome | Coved ST elevation V1–V2, RBBB morphology |
Sources: Harrison's Principles of Internal Medicine 22E; Guyton and Hall Medical Physiology; Tintinalli's Emergency Medicine; Fuster and Hurst's The Heart 15th Edition; Ganong's Review of Medical Physiology.
This is a shared conversation. Sign in to Orris to start your own chat.