Occular infection
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching the Web
ocular infections overview types pathogens treatment 2024
Finding Sources
Finding Sources
Reading Web Page
ocular infections overview types pathogens treatment
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a full overview of ocular infections, organized by the part of the eye affected - from superficial to deep.
Ocular Infections - Overview
Understanding which part of the eye is infected guides both diagnosis and treatment. The anatomy diagram below shows the key structures involved:
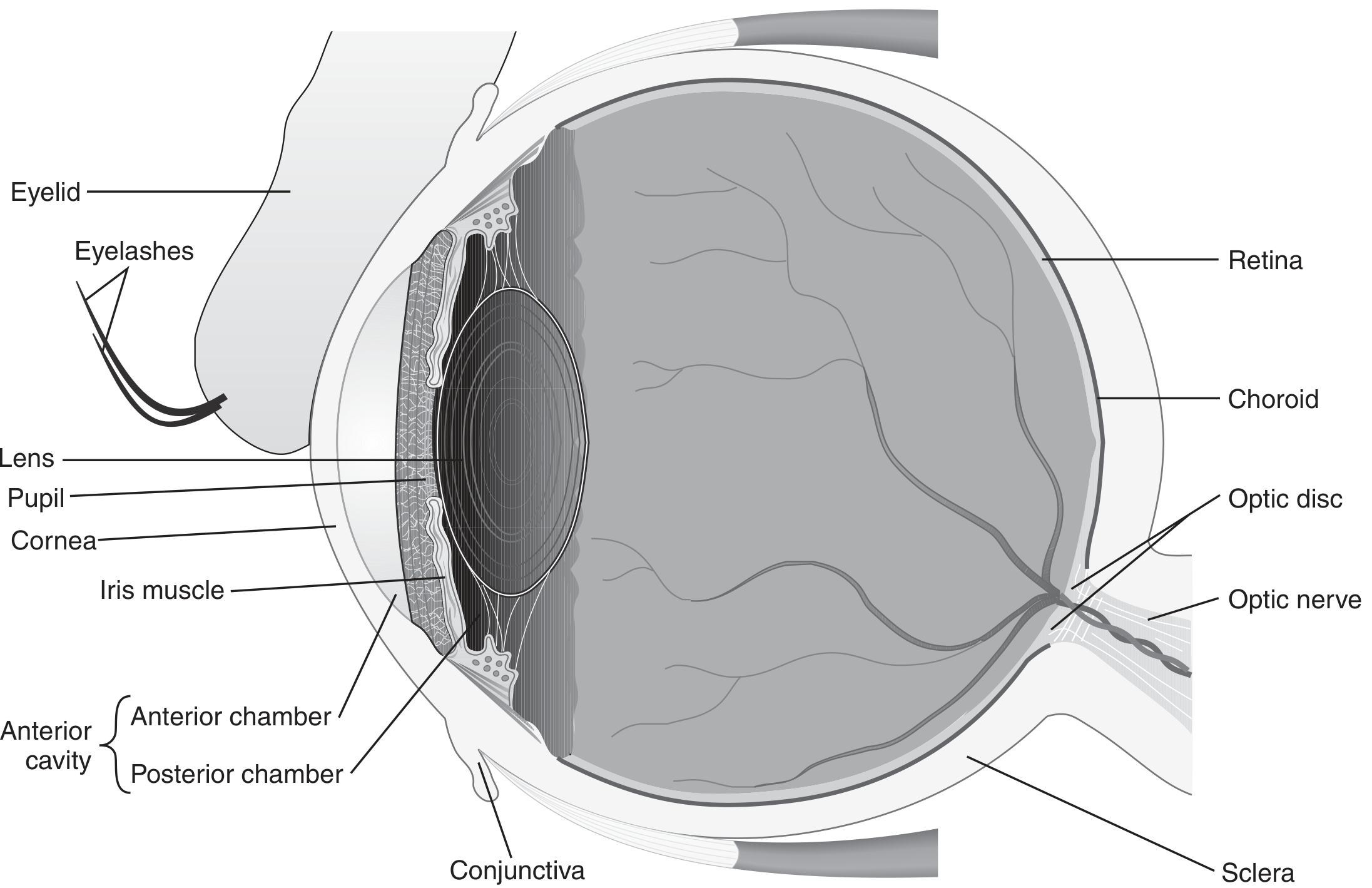
1. Conjunctivitis ("Pink Eye")
The most common ocular infection. The conjunctiva is the mucous membrane lining the inner eyelids and covering the white of the eye up to the corneal edge.
Viral Conjunctivitis
- Most common type in adults
- Classic features: watery discharge, conjunctival redness, often starts in one eye and spreads bilateral
- May come with fever, runny nose, sore throat
- Adenoviruses account for up to 90% of viral cases - highly contagious
- Some adenovirus serotypes cause epidemic keratoconjunctivitis (involving the cornea), with symptoms lasting weeks to months
- HSV and VZV can also cause conjunctivitis and may extend to deeper eye structures
- Other causes: influenza, EBV, measles, mumps, molluscum contagiosum
- Treatment: Usually self-resolves within 2 weeks; supportive care
Bacterial Conjunctivitis
- More common in children than adults
- Typical organisms: Staphylococcus aureus, Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis - in adults, S. aureus predominates
- Usually self-limited; benefit of topical antibiotics is debated but they are commonly prescribed
Hyperacute bacterial conjunctivitis (a more severe subtype):
- Neisseria gonorrhoeae (and less often N. meningitidis)
- Copious, thick yellow-green discharge
- Requires systemic antibiotics (IM ceftriaxone), not just topical
Chlamydial conjunctivitis:
- Chlamydia trachomatis - usually sexually acquired
- Trachoma (serotypes A, B, Ba, C) is the leading infectious cause of blindness worldwide - repeated infections cause eyelid scarring and corneal scarring
- Treatment: tetracycline eye ointment and/or oral azithromycin; oral doxycycline for genital chlamydia types
2. Keratitis (Corneal Infection)
An infection of the cornea - the clear front dome of the eye. Far more serious than conjunctivitis, as corneal scarring can permanently impair vision.
Bacterial Keratitis
- Occurs with eye trauma, contact lens overwear, or corneal disease
- Organisms: Staphylococcus (including MRSA), Streptococcus, occasionally Mycobacterium
- Presents as a corneal ulcer - requires slit lamp examination to diagnose
- Treatment: topical fluoroquinolones (e.g., ciprofloxacin) as first-line; ideally after cultures taken from the ulcer
- Ophthalmology referral urgently needed
Herpes Simplex Keratitis
- Common corneal viral pathogen
- Classic finding: dendritic (branching) pattern on fluorescein staining
- Often recurs with any corneal stress (UV exposure, trauma, immunosuppression)
- Treatment: topical or oral antivirals (e.g., acyclovir, ganciclovir ophthalmic gel)
Acanthamoeba Keratitis
- A parasitic infection increasingly linked to contact lens use and exposure to contaminated water
- Presents as a red eye where initial bacterial cultures are negative - often misdiagnosed early
- Pathophysiology not fully understood; can be devastating if treatment is delayed
- Requires specific anti-amoebic therapy (e.g., PHMB, chlorhexidine eye drops)
Fungal Keratitis
- Consider in chronic ulcers or immunocompromised patients
- Common in agricultural settings (trauma with plant material)
- Treatment: topical natamycin or voriconazole
3. Orbital Cellulitis
A bacterial infection of the soft tissues behind the orbital septum (the fat, muscles, nerves surrounding the eye). A serious, sight- and life-threatening infection.

- Most common source: Extension from sinusitis (especially ethmoid sinus)
- Also from: trauma, hematogenous spread
- Peak age: ~12 years old
- Pathogens: S. pneumoniae, S. aureus, S. pyogenes, M. catarrhalis, anaerobes (Bacteroides, Fusobacterium), nontypeable H. influenzae
Distinguishing features (vs. periorbital/preseptal cellulitis):
- Proptosis (bulging eye)
- Impaired or painful eye movements
- Decreased visual acuity
- Chemosis (swelling of the conjunctiva)
- Afferent pupillary defect
Diagnosis: CT scan of orbit + sinuses (also identifies abscess)
Complications: Subperiosteal abscess, orbital abscess, cavernous sinus thrombosis, endophthalmitis
Treatment: Inpatient with IV antibiotics
- First-line: cefuroxime (50 mg/kg IV q8h) or ampicillin-sulbactam (50 mg/kg IV q6h)
- Add clindamycin or metronidazole if anaerobes suspected
- Add vancomycin if MRSA suspected
- Total course: ~3 weeks (IV then oral)
- Ophthalmology + ENT co-management; surgery if abscess present
4. Endophthalmitis (Intraocular Infection)
Infection of the vitreous and/or aqueous humour - the interior of the eye. A medical emergency.
Exogenous Endophthalmitis
- More common; pathogens enter via the ocular surface
- Main risk factors: Cataract surgery, intravitreal injections (e.g., for macular degeneration)
- Eye trauma is the leading cause in some countries
- Pathogens: Coagulase-negative staphylococci (most common), Bacillus cereus after trauma (causes fulminant rapid vision loss)
- Treatment: Intravitreal antibiotic injections (primary); vitrectomy for severe or refractory cases; systemic antibiotics generally not added except in fungal cases
Endogenous Endophthalmitis
- Pathogens reach the eye via bloodstream (bacteremia or fungemia)
- Fungal: Candida spp. most common - candidemia carries ~9% risk of chorioretinitis and ~1.6% progression to endophthalmitis
- Risk factors: central venous catheters, IV drug use, severe immunocompromise
- Also caused by molds (Aspergillus, Fusarium)
- Treatment: systemic antifungal therapy with voriconazole or fluconazole for at least 4-6 weeks (IDSA guidelines) + intravitreal injections
5. Posterior Segment Infections (Retinitis)
CMV Retinitis
- Occurs in immunocompromised patients (HIV/AIDS, post-transplant)
- Features: retinal hemorrhages, perivascular exudates, granular retinitis with minimal vitritis
- Treatment: Induction with IV ganciclovir 5 mg/kg q12h OR oral valganciclovir 900 mg q12h for 2-3 weeks, then maintenance valganciclovir 900 mg daily
Acute Retinal Necrosis (ARN) / Progressive Outer Retinal Necrosis (PORN)
- Caused by VZV or HSV; extremely rare but an ophthalmologic emergency
- Mechanism: vaso-occlusive angiitis of retinal and choroidal vessels
- Rapid irreversible vision loss possible
- Symptoms: sudden vision decline, photophobia, floaters, eye pain/redness
- Requires urgent systemic antivirals
Summary Table
| Type | Location | Key Pathogens | Red Flags / Urgency |
|---|---|---|---|
| Conjunctivitis | Conjunctiva | Adenovirus, S. aureus, N. gonorrhoeae, Chlamydia | Hyperacute = urgent |
| Keratitis | Cornea | HSV, bacteria, Acanthamoeba, fungi | Any corneal ulcer = ophthalmology same-day |
| Orbital cellulitis | Orbital fat/muscle | S. aureus, S. pneumoniae, anaerobes | Inpatient IV antibiotics |
| Endophthalmitis | Vitreous/aqueous | CoNS, Bacillus, Candida | Emergency - risk of blindness |
| CMV retinitis | Retina | CMV | Urgent in immunocompromised |
| ARN / PORN | Retina | VZV, HSV | Ophthalmologic emergency |
Sources: Tietz Textbook of Laboratory Medicine 7e, Roberts & Hedges' Clinical Procedures in Emergency Medicine, Tintinalli's Emergency Medicine, State-of-the-Art Review: Ocular Infections (PMC, 2024)
This is a shared conversation. Sign in to Orris to start your own chat.