Teach me basal ganglia
Reading File
Finding Sources
Searching the Web
basal ganglia anatomy circuits neuroscience
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
I now have everything I need for a thorough, well-illustrated response. Let me compose the full teaching answer.
The Basal Ganglia - A Complete Guide
(Sources: Ganong's Review of Medical Physiology 26e, Neuroanatomy through Clinical Cases 3e, Costanzo Physiology 7e, Kandel's Principles of Neural Science 6e)
1. What Are the Basal Ganglia?
The basal ganglia (more accurately called "basal nuclei") are a group of subcortical gray matter structures embedded deep in the white matter of the cerebral hemispheres. They sit at the base of the forebrain and top of the midbrain and have strong two-way connections with the cerebral cortex and thalamus.
Key concept: The basal ganglia do NOT project directly to the spinal cord or muscles. They influence motor behavior exclusively by modulating the cortex via the thalamus. Their role is best understood as a "gating" or "selection" system - they decide which movements get executed and suppress competing ones.
2. Components and Anatomy
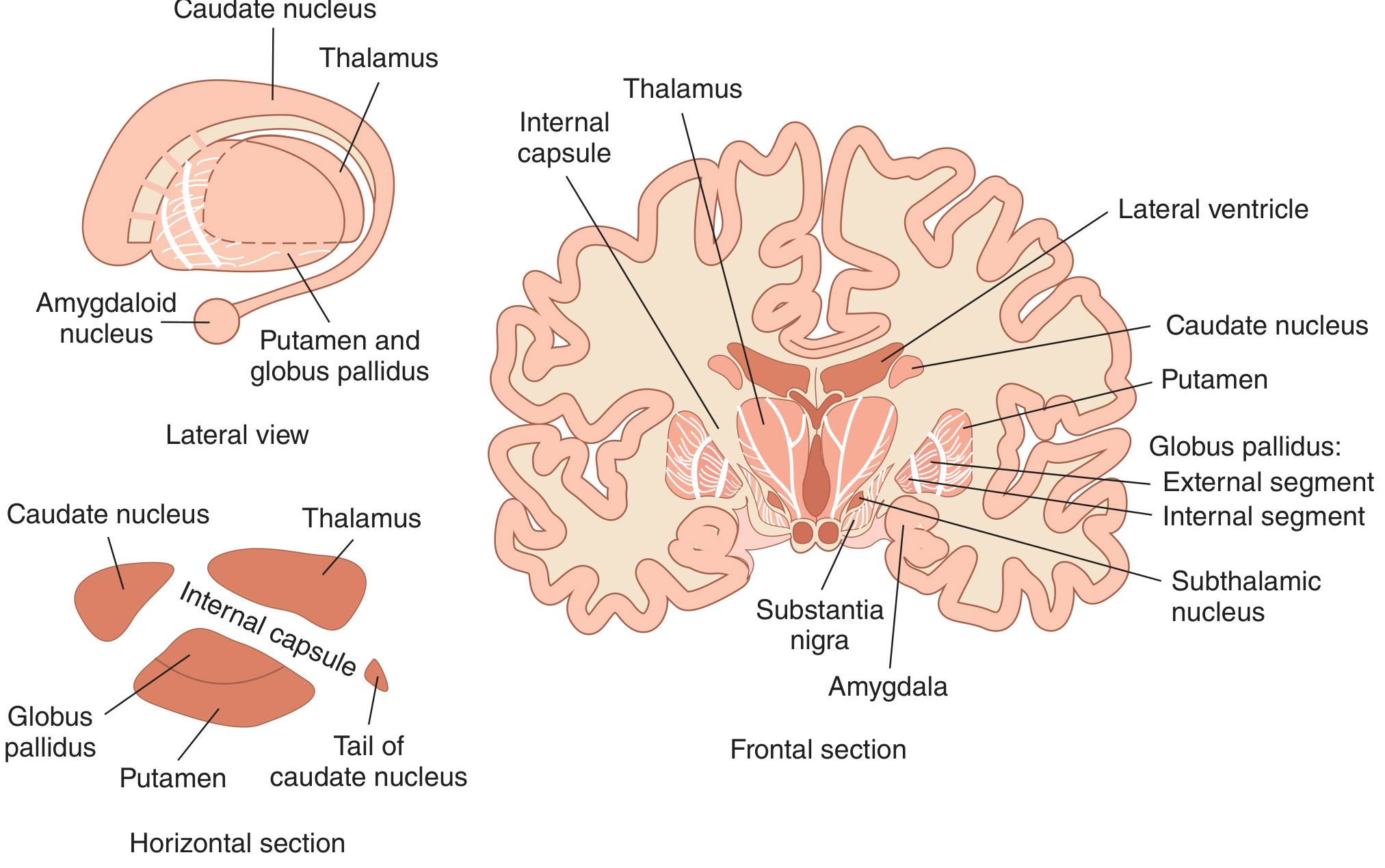
Here is the spatial layout of the basal ganglia:
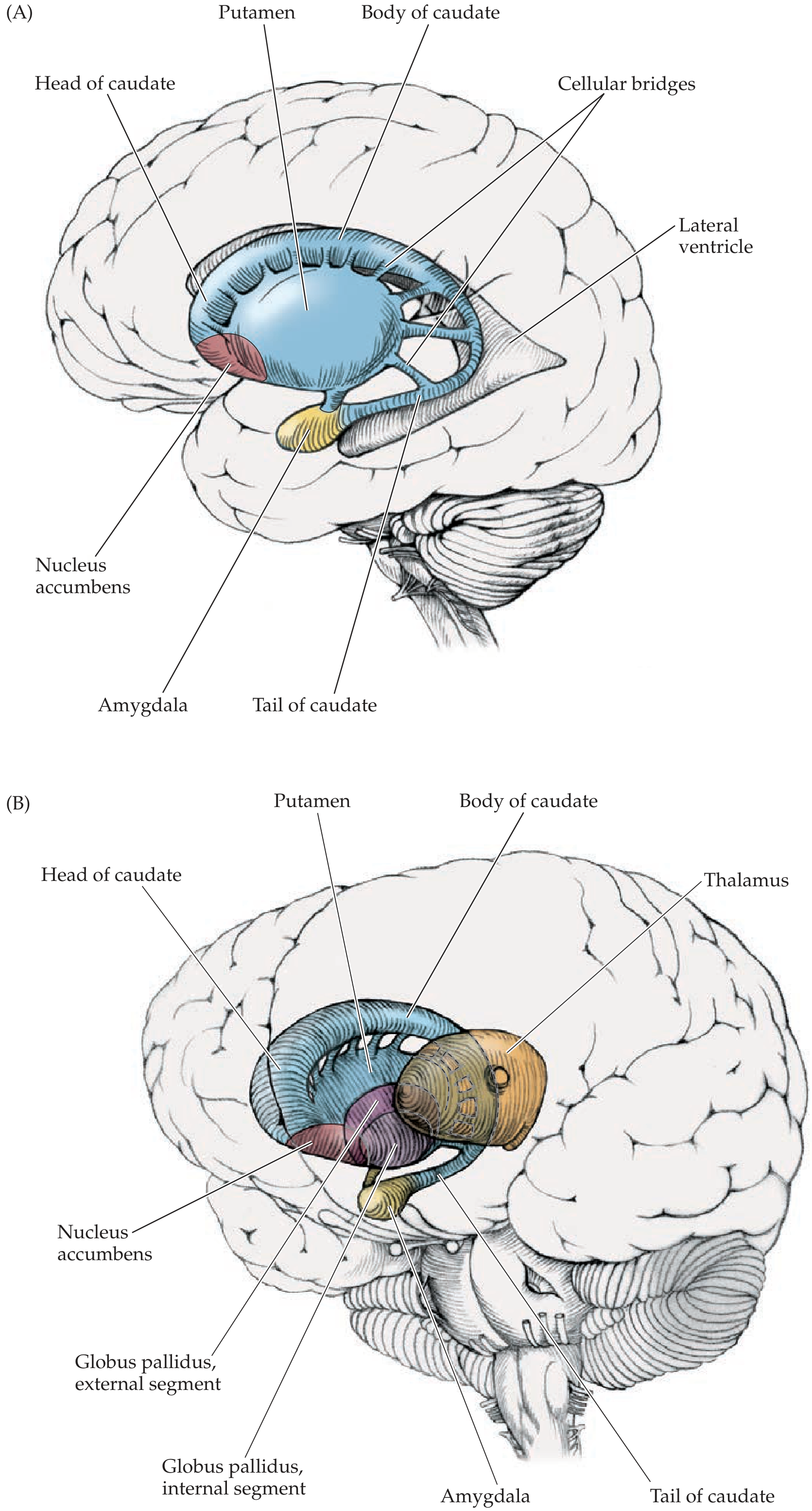
Here is the 3D spatial relationship showing caudate (blue), globus pallidus, nucleus accumbens, and amygdala:
The five nuclei and their groupings:
| Grouping | Nuclei |
|---|---|
| Striatum (main input zone) | Caudate nucleus + Putamen |
| Lenticular/Lentiform nucleus | Putamen + Globus pallidus |
| Output nuclei | GPi (internal globus pallidus) + SNpr (substantia nigra pars reticulata) |
| Intrinsic nucleus | GPe (external globus pallidus) |
| Relay nucleus | Subthalamic nucleus (STN) |
| Modulatory | Substantia nigra pars compacta (SNpc) |
Key structural points:
-
Caudate nucleus - C-shaped, follows the lateral ventricle; has a head, body, and tail. The tail ends near the amygdala in the temporal lobe. The caudate is particularly connected to the prefrontal cortex and is important for cognitive and eye-movement functions.
-
Putamen - The largest basal ganglia structure, forming the most lateral part. The putamen fuses anteriorly with the caudate head. The junction zone is the ventral striatum, which contains the nucleus accumbens (key in reward and limbic circuits).
-
Globus pallidus - "Pale globe," named for its many myelinated fibers. Divided into:
- GPe (external segment) - intrinsic relay
- GPi (internal segment) - main output to thalamus
-
The caudate and putamen look continuous in histological sections because cellular bridges connect them through the internal capsule fibers, creating the "striped" (striated) appearance - hence the name "striatum."
-
Substantia nigra - Located in the midbrain. Divided into:
- SNpc (pars compacta) - dopaminergic neurons, dark due to neuromelanin
- SNpr (pars reticulata) - GABAergic neurons, functionally similar to GPi
-
Subthalamic nucleus (STN) - Small nucleus in the diencephalon; the only excitatory (glutamatergic) nucleus within the basal ganglia circuit.
3. Neurotransmitters at a Glance
| Structure | Neurotransmitter | Effect |
|---|---|---|
| Striatum (medium spiny neurons, 95%) | GABA | Inhibitory |
| Striatum interneurons | Acetylcholine | Modulatory |
| GPe, GPi | GABA | Inhibitory |
| SNpr | GABA | Inhibitory |
| SNpc | Dopamine | D1 = excitatory; D2 = inhibitory |
| Subthalamic nucleus | Glutamate | Excitatory |
| Cortex → Striatum | Glutamate | Excitatory |
4. The Two Main Pathways (Circuit Physiology)
The basal ganglia receive massive excitatory (glutamatergic) input from the entire cerebral cortex and thalamus, both arriving at the striatum. The circuit then splits into two competing pathways:
Here is the complete connections diagram:
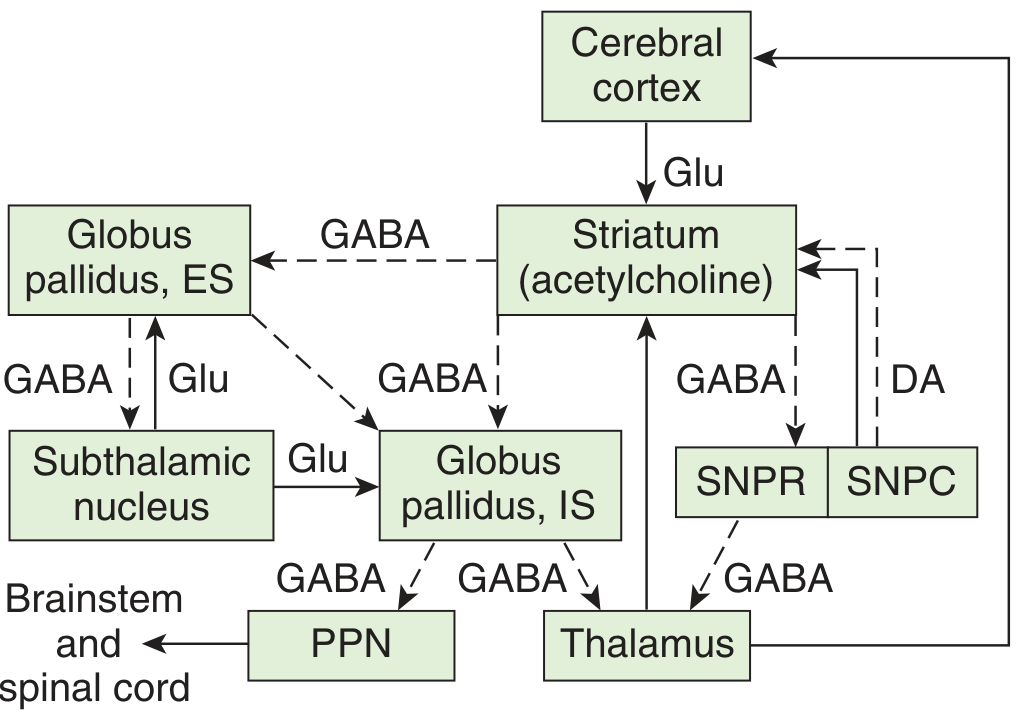
Direct Pathway - "Go" Signal (net excitatory to cortex)
Cortex --[Glu +]--> Striatum --[GABA -]--> GPi/SNpr --[GABA -]--> Thalamus --[Glu +]--> Cortex
Step by step:
- Cortex excites striatum (glutamate)
- Striatum inhibits GPi (GABA) -- D1 receptors on these neurons are excited by dopamine
- GPi is thus suppressed - it STOPS tonically inhibiting the thalamus
- Thalamus is now free to excite the cortex (glutamate)
- Net result: INCREASED cortical motor activity (movement facilitated)
The key insight: GPi/SNpr are tonically active at rest, constantly inhibiting the thalamus. The direct pathway DISINHIBITS the thalamus.
Indirect Pathway - "Stop" Signal (net inhibitory to cortex)
Cortex --[Glu +]--> Striatum --[GABA -]--> GPe --[GABA -]--> STN --[Glu +]--> GPi --[GABA -]--> Thalamus --[Glu +]--> Cortex
Step by step:
- Cortex excites striatum (glutamate)
- Striatum inhibits GPe (GABA) -- D2 receptors on these neurons are inhibited by dopamine
- GPe STOPS inhibiting the STN
- STN becomes active and excites GPi (glutamate)
- GPi strongly inhibits the thalamus (GABA)
- Thalamus cannot excite cortex
- Net result: DECREASED cortical motor activity (movement suppressed)
The Balance
The direct and indirect pathways are in constant opposition:
- Direct pathway = "press the gas" → facilitates movement
- Indirect pathway = "press the brake" → suppresses movement
Normal motor control = a precise balance between these two pathways, allowing smooth, purposeful movements while suppressing unwanted ones.
5. Role of Dopamine (The Master Modulator)
The SNpc sends dopaminergic fibers to the striatum (the nigrostriatal pathway). Dopamine acts differently depending on the receptor type:
| Receptor | Location | Effect of dopamine | Pathway affected |
|---|---|---|---|
| D1 | Direct pathway neurons | Excites striatum | Facilitates direct pathway (more "go") |
| D2 | Indirect pathway neurons | Inhibits striatum | Suppresses indirect pathway (less "stop") |
Net effect of dopamine: it biases the system toward movement. When dopamine is present:
- Direct pathway is enhanced (D1 activation)
- Indirect pathway is suppressed (D2 inhibition)
- Result: thalamus is more active, cortex gets more motor drive
When dopamine is lost (as in Parkinson's), the balance tips toward excessive inhibition.
6. Functional Territories - It's Not Just Motor
The basal ganglia have several parallel circuits for different functions:
| Circuit | Input cortex | Striatum area | Function |
|---|---|---|---|
| Sensorimotor | Motor/somatosensory cortex | Putamen | Voluntary motor control |
| Cognitive/Prefrontal | Prefrontal cortex | Head of caudate | Working memory, planning, object reversal tasks |
| Oculomotor | Frontal eye fields | Caudate (body) | Voluntary eye movements (saccades) |
| Limbic | Cingulate, orbitofrontal | Nucleus accumbens | Reward, motivation, emotion |
This is why basal ganglia diseases affect far more than just movement - they affect mood, cognition, impulse control, and reward processing.
7. Clinical Diseases of the Basal Ganglia
Three biochemical systems normally operate in balance in the basal ganglia:
- Dopaminergic nigrostriatal system
- Intrastriatal cholinergic system
- GABAergic system (striatum → GPi/SNpr)
Disruption of any one causes characteristic movement disorders, either hypokinetic (reduced movement) or hyperkinetic (excessive movement).
Parkinson's Disease (Hypokinetic)
Pathology: Degeneration of dopaminergic neurons in the SNpc, especially fibers to the putamen. Loss of dopamine causes:
- D1 understimulation → direct pathway weakened
- D2 underinhibition → indirect pathway overactive
- Combined result: GPi/SNpr become hyperactive → thalamus is excessively inhibited → cortex receives less drive
Clinical features (classic tetrad):
- Resting tremor ("pill-rolling")
- Bradykinesia (slowness)
- Cogwheel rigidity
- Postural instability, shuffling gait
Treatment:
- Levodopa (L-DOPA) - precursor to dopamine, crosses blood-brain barrier
- Dopamine agonists (bromocriptine, ropinirole)
- MAO-B inhibitors (selegiline)
- Deep brain stimulation (DBS) of STN or GPi
Huntington's Disease (Hyperkinetic)
Pathology: Autosomal dominant. CAG trinucleotide repeat expansion in the HTT gene on chromosome 4. Causes progressive destruction of striatal (caudate and putamen) inhibitory GABAergic neurons and cholinergic neurons. The indirect pathway neurons are preferentially lost first.
Circuit effect: Loss of indirect pathway → GPe is not inhibited → STN is inhibited → GPi becomes underactive → thalamus is disinhibited → excessive cortical activation → involuntary movements.
Clinical features:
- Chorea (rapid, involuntary "dancing" movements)
- Athetosis (slow, writhing)
- Progressive cognitive decline and dementia
- Psychiatric symptoms (depression, personality changes)
No cure. Symptoms managed with tetrabenazine (depletes dopamine), antipsychotics.
Hemiballismus
Pathology: Unilateral lesion (usually lacunar infarct) of the subthalamic nucleus.
Circuit effect: Loss of STN excitation to GPi → GPi underactive → thalamus disinhibited → uncontrolled contralateral movements.
Clinical feature: Violent, large-amplitude flinging movements of the contralateral arm/leg.
Wilson's Disease
Pathology: Autosomal recessive. Defective ATP7B copper transporter → copper accumulates in liver, basal ganglia (putamen), and cornea.
Clinical features:
- Movement disorders (tremor, dysarthria, dysphagia)
- Psychiatric symptoms
- Kayser-Fleischer rings in cornea
- Liver disease
8. Action Selection - The Deeper Role
From Kandel's Principles of Neural Science: The basal ganglia's fundamental function is action selection - choosing one behavior from competing options. Every vertebrate faces this challenge constantly. The neural architecture of the basal ganglia is configured to make winner-take-all selections:
- The focused inhibition pattern through GPi allows one motor program to be "selected" while others are suppressed
- This applies equally to motivational, affective, cognitive, and sensorimotor processing
- Reinforcement learning is built into this system: phasic dopamine signals from SNpc encode reward prediction errors, biasing future selections toward rewarding outcomes
This is why basal ganglia circuits are central to addiction (nucleus accumbens dopamine), obsessive-compulsive disorder (caudate hyperactivity), and habit formation.
9. Summary Table
| Structure | Input | Output | Neurotransmitter | Role |
|---|---|---|---|---|
| Striatum | Cortex, thalamus, SNpc | GPe, GPi, SNpr | GABA (projection), ACh (interneurons) | Main input station |
| GPe | Striatum | STN, GPi | GABA | Indirect pathway relay |
| STN | GPe, cortex | GPi, SNpr | Glutamate | Drive output nuclei |
| GPi | Striatum (direct), STN (indirect) | Thalamus, brainstem | GABA | Main output - tonic inhibitor |
| SNpr | Striatum | Thalamus, superior colliculus | GABA | Output (esp. eye movements) |
| SNpc | Various | Striatum (nigrostriatal) | Dopamine | D1 excites, D2 inhibits |
10. Quick Memory Aid
"CUPS + N" = the 5 components:
- Caudate
- U - (Putamen)
- Pallidum (Globus pallidus)
- Subthalamic nucleus
- Nigra (Substantia nigra)
Direct = "D1-D-Go" (D1 receptor, Dopamine, Go signal)
Indirect = "D2-D-No" (D2 receptor, Dopamine inhibits = No brakes = Stop signal)
Parkinson = Too much brake (dopamine lost → indirect pathway wins)
Huntington = Lost the brake (striatal GABA neurons lost → indirect pathway fails)
Sources: Ganong's Review of Medical Physiology 26e, p. 251; Neuroanatomy through Clinical Cases 3e, pp. 767-775; Costanzo Physiology 7e, p. 116; Kandel's Principles of Neural Science 6e, p. 980
This is a shared conversation. Sign in to Orris to start your own chat.