Peripartum CARDIOMYOPATHY in detail post graduate level exam oriented from standard textbooks
Reading File
Finding Sources
Finding Sources
Searching PubMed
"peripartum cardiomyopathy"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, multi-textbook content with excellent visuals. Let me compile the complete postgraduate-level answer.
PERIPARTUM CARDIOMYOPATHY (PPCM)
Postgraduate Level - Comprehensive Review
DEFINITION
Peripartum cardiomyopathy (PPCM) is an idiopathic cardiomyopathy presenting with heart failure (HF) due to left ventricular systolic dysfunction, occurring toward the end of pregnancy or in the first months following delivery, where no other cause of HF is found.
Diagnostic Criteria (Criteria of Demakis et al., modified):
- Development of cardiac failure in the last month of pregnancy or within 5 months of delivery
- LVEF <45% (or M-mode fractional shortening <30%, or LVEDD >2.7 cm/m² BSA)
- Absence of another identifiable cause of HF (diagnosis of exclusion)
- Absence of pre-existing heart disease before the last month of pregnancy
PPCM is a diagnosis of exclusion - all other causes of cardiac dysfunction must be ruled out.
- Braunwald's Heart Disease, 11th Ed.; Goldman-Cecil Medicine; Fuster and Hurst's The Heart, 15th Ed.
INCIDENCE & EPIDEMIOLOGY
| Region | Incidence |
|---|---|
| USA | 1:1000 to 1:4000 live births |
| Haiti | 1:300 live births |
| Africa | 1:100 live births |
| Japan | 1:20,000 live births |
| Worldwide average | ~1:1000 pregnancies |
Racial disparity - a key exam point:
- Non-Hispanic Black women have a 5-15 fold increased risk compared to other ethnic groups (Goldman-Cecil)
- Black women show more severe disease, slower recovery, lower recovery rates
- One-year mortality in predominantly Black cohorts: 11% vs 4% in mixed cohorts
Increasing incidence in the USA is attributed to: older maternal age, multifetal pregnancies from assisted reproduction, obesity epidemic, improved echocardiographic detection.
- Harrison's Principles of Internal Medicine, 22E (2025); Fuster and Hurst's The Heart, 15th Ed.; Goldman-Cecil Medicine
RISK FACTORS
| Category | Specific Risk Factors |
|---|---|
| Demographic | Age >30 years, African-American/Black ethnicity |
| Obstetric | Multiparity, multifetal (twin) pregnancy, assisted reproduction |
| Hypertensive | Preeclampsia (~25% of PPCM vs 5% in general population), gestational hypertension |
| Medical | Malnutrition, low selenium |
| Iatrogenic | Tocolytic therapy (especially β-mimetics like terbutaline) |
| Genetic | Family history of DCM, TTN mutations |
Preeclampsia is present in up to 25% of PPCM patients (vs. ~5% in general obstetric population), suggesting a shared predisposition or overlapping pathogenic mechanisms.
- Creasy & Resnik's Maternal-Fetal Medicine; Harrison's 22E; Fuster and Hurst's
PATHOPHYSIOLOGY
This is the most examined topic in PPCM at PG level. Three major hypotheses converge into the current "vasculo-hormonal model":
1. Prolactin/Vasoinhibin Hypothesis (Most Supported)
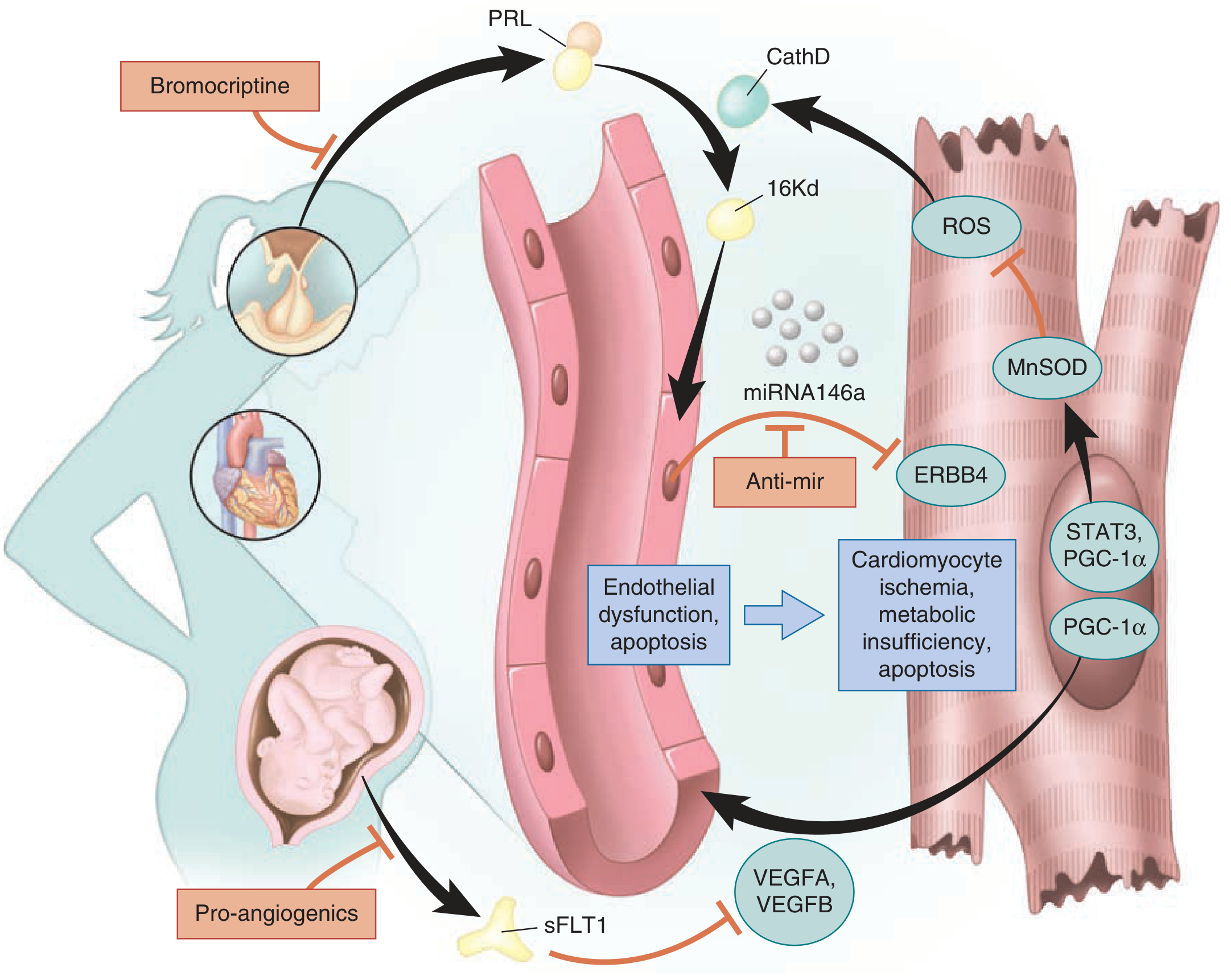
Fuster and Hurst's The Heart, 15th Ed. - Pathophysiology of PPCM
- STAT3 (Signal Transducer and Activator of Transcription 3) is downregulated in susceptible cardiomyocytes
- Reduced STAT3 → decreased MnSOD (manganese superoxide dismutase) expression
- Mitochondrial reactive oxygen species (ROS) accumulate unchecked
- Elevated ROS activates Cathepsin D (lysosomal protease)
- Cathepsin D cleaves full-length prolactin (23 kDa) into a 16 kDa antiangiogenic, proapoptotic fragment ("vasoinhibin")
- 16 kDa prolactin fragment causes:
- Endothelial cell apoptosis
- Impaired cardiomyocyte metabolism
- Inhibition of cardiomyocyte contraction
- Packaged into exosomes that also contain miRNA-146a → suppresses ERBB4 signaling in cardiomyocytes
Therapeutic implication: Bromocriptine (dopamine agonist) inhibits prolactin secretion, blocking this cascade.
2. Antiangiogenic Hypothesis (sFLT-1)
- The placenta secretes soluble fms-like tyrosine kinase-1 (sFLT-1) in late pregnancy
- sFLT-1 is a VEGF inhibitor - it binds and sequesters VEGF-A and VEGF-B
- This creates an angiogenic imbalance - the myocardial microvasculature cannot adapt adequately
- High sFLT-1 levels predict worse outcome in PPCM
- Shared with the pathophysiology of preeclampsia (explains the association)
- Pro-angiogenic agents are under experimental investigation
3. Genetic Predisposition
- ~15% of PPCM cases harbor rare truncating variants in TTN (titin gene) - the same gene implicated in DCM
- Other implicated genes: TTNC1, STAT3, MYH7, SCN5A, LMNA, DSP
- Among 90 DCM families, 6% had at least one member with PPCM
- Genetic testing reveals undiagnosed DCM in relatives of PPCM non-recoverers
- TTN truncating variants predict lower EF at 1-year follow-up and reduced recovery
- "PPCM may represent DCM occurring during pregnancy" - pregnancy is an environmental trigger for a genetically susceptible heart
4. Other Proposed Mechanisms
-
Autoimmune/inflammatory: Lymphocytic myocarditis found in 30-50% of endomyocardial biopsies; cross-reactivity between uterine and cardiac myocyte proteins
-
Nutritional: Low selenium levels (especially in Africa)
-
Viral myocarditis: Enhanced susceptibility during immunological changes of pregnancy
-
Hemodynamic stress: Volume overload + increased cardiac output of pregnancy precipitates failure
-
Fuster and Hurst's The Heart, 15th Ed.; Goldman-Cecil Medicine; Harrison's 22E; Braunwald's Heart Disease
TEMPORAL CLASSIFICATION
| Category | Timing |
|---|---|
| Traditional PPCM | Last month of pregnancy to 5 months postpartum |
| Early PACM (Pregnancy-Associated Cardiomyopathy) | 2nd-3rd trimester (earlier in pregnancy) |
| Most common presentation | First 2 weeks after delivery (when fluid mobilization unmasks failure) |
| Prepartum diagnoses | Most commonly in last month of pregnancy |
Why postpartum peak? The excess blood volume (40-50% expansion during pregnancy) mobilizes after delivery, dramatically increasing cardiac preload. If the ventricle is dysfunctional, this precipitates acute decompensation with pulmonary edema.
CLINICAL PRESENTATION
Symptoms
- Dyspnea on exertion (most common)
- Orthopnea, paroxysmal nocturnal dyspnea
- Fatigue, reduced exercise tolerance
- Chest pain (occasionally)
- Palpitations
- Peripheral leg edema
Signs
- Tachycardia (compensatory)
- S3 gallop (volume overload)
- Elevated JVP
- Crackles at lung bases (pulmonary edema)
- Displaced apex (cardiomegaly)
- Mitral/tricuspid regurgitation murmurs
- Peripheral edema
Diagnostic challenge: Dyspnea, fatigue, and edema are all normal in late pregnancy, leading to delayed diagnosis. Key differentiators are:
- Elevated BNP/NT-proBNP
- Elevated troponin
- Clinical features inconsistent with normal pregnancy (orthopnea, PND, S3)
- Elevated CVP
- Onset of hypertension (preeclampsia overlap)
Complications
- Atrial and ventricular arrhythmias (life-threatening)
- LV thrombus (particularly with LVEF <30-35%) → systemic emboli
- Cardiogenic shock
- Cardiopulmonary arrest
- Death
- Predictors of complications: LVEF <30%, Black ethnicity, delayed diagnosis
DIFFERENTIAL DIAGNOSIS (Exam Critical)
| Condition | Key distinguishing feature |
|---|---|
| Preeclampsia-related pulmonary edema | Resolves with BP control, no LV dysfunction |
| Pulmonary embolism | Normal LVEF, right heart strain pattern |
| Amniotic fluid embolism | Acute intrapartum collapse, DIC |
| Myocarditis | Histological distinction (30-50% overlap with PPCM) |
| Dilated cardiomyopathy (pre-existing) | History pre-dates last trimester |
| SCAD (Spontaneous Coronary Artery Dissection) | Regional wall motion abnormality, coronary imaging required |
| Tocolytic (β-mimetic)-induced HF | Drug history, resolves on drug cessation |
| Hypertensive cardiomyopathy | Long-standing HTN history |
| Takotsubo cardiomyopathy | Apical ballooning, stress trigger, postmenopausal more common |
INVESTIGATIONS
Echocardiography (Investigation of Choice)
- Global LV systolic dysfunction - LVEF <45%
- Variable LV dilatation (LVEDD >2.7 cm/m² BSA)
- M-mode fractional shortening <30%
- Right ventricular and biatrial dilatation
- Functional MR and TR
- Elevated pulmonary pressures
- LV apical thrombus - seen with severely depressed LV function
ECG
- Non-specific ST-T changes
- Sinus tachycardia
- LV hypertrophy pattern
- Left bundle branch block
- Arrhythmias (AF, VT)
Chest X-Ray
- Cardiomegaly
- Pulmonary venous congestion / pulmonary edema
- Pleural effusions
Biomarkers
- BNP/NT-proBNP: Markedly elevated; high levels predict worse outcome and less recovery
- Troponin: Elevated in myocardial damage; elevated levels = worse prognosis
- sFLT-1: Elevated; correlates with disease severity and poor recovery
Cardiac MRI
- Accurate assessment of chamber volumes and EF
- Detection of mural thrombi
- Late gadolinium enhancement (LGE) - predicts fibrosis and non-recovery
- Gadolinium is CONTRAINDICATED during pregnancy (fetal risk)
- Preferred in complex cases where echocardiography is inconclusive
Endomyocardial Biopsy
- Not routine
- Lymphocytic myocarditis found in 30-50% of specimens
- Reserved for atypical presentations or suspected giant cell myocarditis
Genetic Testing
- Recommended given ~15% yield for TTN truncating variants
- Impacts patient prognosis (TTN+ = lower recovery rates)
- Important for family screening - reveals undiagnosed DCM in relatives
MANAGEMENT
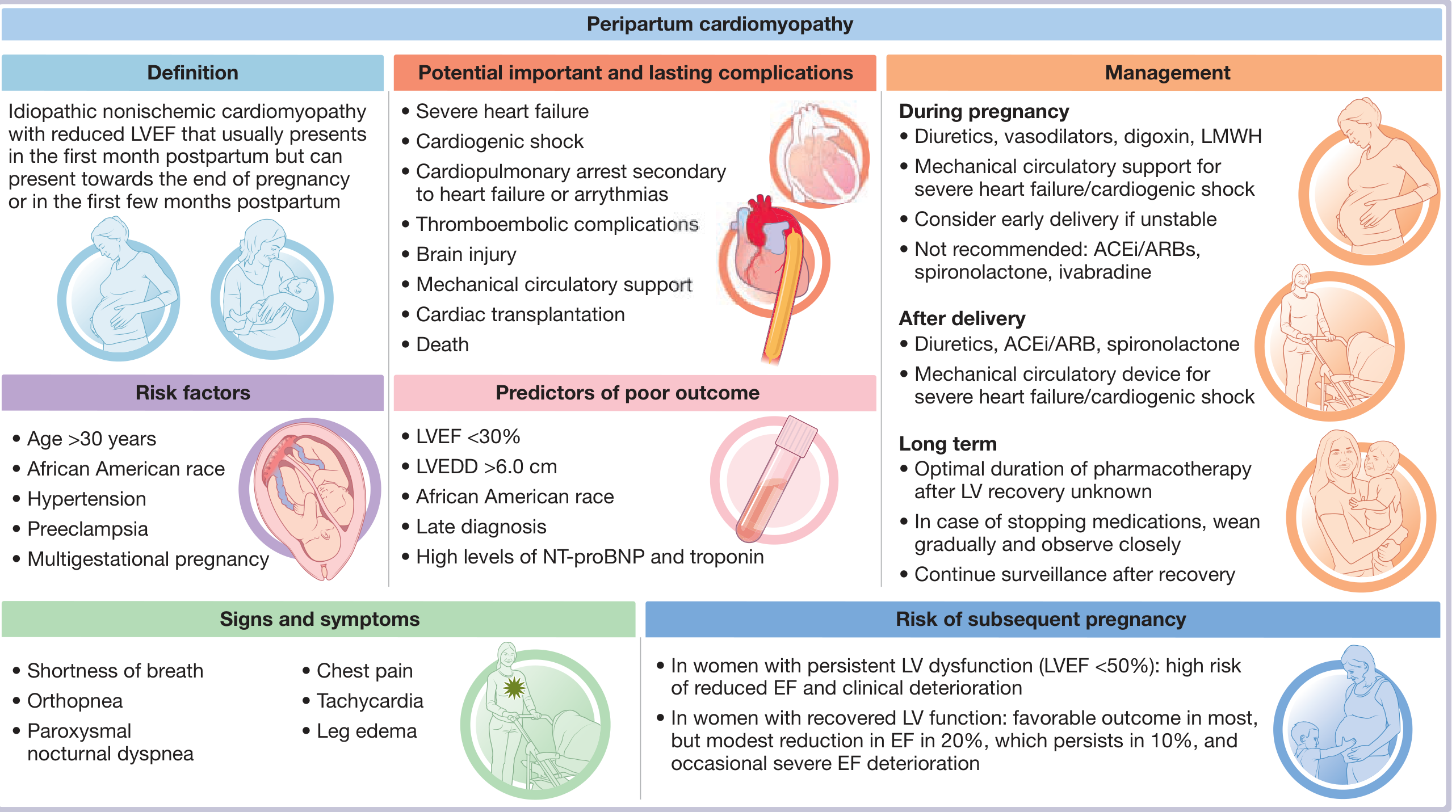
Fuster and Hurst's The Heart, 15th Ed. - PPCM Central Illustration
A. DURING PREGNANCY (Pre-delivery)
Goal: Stabilize mother while protecting fetus
| Drug Class | Safe in Pregnancy | Drug/Dose | Notes |
|---|---|---|---|
| Diuretics | Yes (cautiously) | Furosemide | Avoid over-diuresis - may compromise uteroplacental flow |
| Vasodilators | Yes | Hydralazine + Isosorbide dinitrate | ACEi/ARB/Sacubitril-valsartan are CONTRAINDICATED - fetal renal injury, oligohydramnios |
| Beta-blockers | Yes | Metoprolol, carvedilol | For arrhythmia, rate control |
| Digoxin | Yes | Standard doses | For arrhythmia, positive inotropy |
| Anticoagulation | Yes | LMWH (preferred) | UFH second choice; warfarin CONTRAINDICATED (embryopathy, fetal hemorrhage) |
| Spironolactone | NO | Contraindicated | Anti-androgenic effects on fetus |
| Ivabradine | NO | Contraindicated | Fetal harm |
Key principle: Early delivery should be considered if hemodynamic instability persists - collaboration with maternal-fetal medicine team is essential.
B. AFTER DELIVERY (Postpartum)
Full HFrEF guideline-directed medical therapy (GDMT):
- ACE inhibitors/ARBs (enalapril, lisinopril) - reduce afterload, promote recovery
- Beta-blockers (metoprolol tartrate, carvedilol) - shown compatible with breastfeeding
- Spironolactone - shown compatible with breastfeeding
- Loop diuretics (furosemide) - for fluid overload
- Sacubitril/valsartan can be used postpartum (not breastfeeding)
- SGLT2 inhibitors - emerging; limited data in PPCM specifically
C. ANTICOAGULATION
- Indication: LVEF <0.35 OR marked LV dilation (high thrombus/embolic risk)
- Duration: First 6 weeks postpartum (once obstetric bleeding has resolved)
- Agent: LMWH preferred; warfarin can be used postpartum (does NOT cross into breast milk in significant amounts)
- LV thrombus on echo: anticoagulate until thrombus resolves
D. BROMOCRIPTINE - The Key Exam Drug
- Mechanism: Dopamine D2 agonist → inhibits pituitary prolactin secretion → prevents cleavage into toxic 16 kDa fragment
- Dose: Various regimens studied; Goldman-Cecil: 2.5 mg twice daily for 2 weeks, then once daily for 6 weeks
- Evidence: Small RCTs (notably Sliwa et al., South Africa) showed improved LVEF recovery and reduced mortality
- Status: Still experimental/controversial - no large RCT with placebo control
- 2025 Meta-analysis (PMID 41213878): Confirms potential benefit in LV recovery; awaits large confirmatory RCT
- Important: Bromocriptine suppresses lactation - therefore breastfeeding must be stopped if bromocriptine is used
- Current approach: Reasonable to add if traditional measures are insufficient; supported by ESC Heart Failure guidelines
E. DEVICES AND ADVANCED HEART FAILURE
| Device/Intervention | Indication | Notes |
|---|---|---|
| Wearable defibrillator (LifeVest) | LVEF <0.35 at presentation | Bridge to recovery (6 weeks-3 months); higher recovery rate than other DCMs |
| ICD (implantable) | Sustained VT/VF, or LVEF <35% despite >3 months optimal therapy | Consider if no recovery |
| IABP / Impella | Cardiogenic shock not responding to medical therapy | Bridge to recovery |
| ECMO | Refractory cardiogenic shock with oxygenation failure | Bridge to recovery/decision |
| Durable LVAD | Severe persistent HF | Bridge to transplant; INTERMACS data shows only 6% recover on LVAD |
| Cardiac transplantation | Refractory HF not amenable to other therapies | ~4% require transplant; younger age, higher sensitization rates in PPCM |
Important PG Exam point: Because recovery rates in PPCM are higher than in other DCMs, temporary devices as bridge to recovery should be attempted before committing to cardiac transplantation.
- Harrison's 22E; Fuster and Hurst's The Heart, 15th Ed.; Creasy & Resnik's; Goldman-Cecil Medicine
PROGNOSIS
Recovery of LV Function
- 50-80% recover to LVEF ≥50%, mostly within 2-6 months of diagnosis
- Later recovery (beyond 6 months) is possible in some patients
- German cohort (IPAC study): ~50% recovery at 12 months
- The one-year mortality in the USA: 4-11% (4% in IPAC study; 11% in predominantly Black women populations)
- Global registry (worldwide): 6-month mortality ~6% (lowest Europe 4%, highest Middle East 10%)
Predictors of POOR Recovery (Exam Favorite!)
| Predictor | Significance |
|---|---|
| LVEF <30% | Most important; much less likely to recover |
| LVEDD >6.0 cm | Severe dilation = poor recovery |
| Black/African-American ethnicity | Slower and less complete recovery |
| Late diagnosis (>6 weeks postpartum) | Missed window of treatment |
| Elevated troponin | Extensive myocardial injury |
| High BNP/NT-proBNP | Worse prognosis |
| Positive TTN truncating variant | Lower EF at 1 year |
| LV thrombus | Predictor of complications |
| Presentation >6 weeks postpartum | Less favorable than early postpartum |
Predictors of GOOD Recovery
- LVEF at presentation >30-35%
- White/non-Black ethnicity
- Prompt diagnosis and treatment
- LVEDD <5.5 cm
- No LV thrombus
SUBSEQUENT PREGNANCY - Critical Exam Topic
This topic is frequently tested and has important clinical implications:
| Scenario | Risk of Relapse | Maternal Mortality |
|---|---|---|
| Previous PPCM, LV recovered (LVEF ≥50%) | ~20% recurrence of HF | Low (no deaths in major US studies) |
| Previous PPCM, persistent LV dysfunction (LVEF <50%) | ~40-50% recurrence | ~19% maternal mortality |
| Haiti cohort with persistent dysfunction | ~50% recurrence | High |
ESC Guidelines recommendation: Discourage subsequent pregnancy when EF has not recovered to >50-55%.
Key points:
- Even in women with recovered LV function, ~20% have modest EF reduction with subsequent pregnancy (persists in ~10%)
- Isolated cases of severe deterioration and life-threatening arrhythmias have been described even in recovered patients
- Contraception counseling is mandatory - unintended pregnancy should be prevented
- Early termination of unintentional pregnancy should be considered in women with persistent LV dysfunction
Management Algorithm for Subsequent Pregnancy in Women with Persistent LV Dysfunction:
-
Baseline echo and BNP before/at first visit
-
Monthly symptom monitoring up to 30 weeks, then biweekly
-
Continue beta-blockers; switch ACEi/ARB/sacubitril-valsartan to hydralazine/nitrates
-
Anticoagulation with LMWH
-
Delivery planning with maternal-fetal medicine and cardiology team
-
Creasy & Resnik's Maternal-Fetal Medicine; Fuster and Hurst's The Heart, 15th Ed.
BREASTFEEDING
- Previously prohibited (concern about fluid balance and prolactin)
- Now generally encouraged in patients where fluid balance can be maintained
- If bromocriptine is used, breastfeeding must be stopped
- Metoprolol tartrate, enalapril, and spironolactone are compatible with breastfeeding
GENETIC CONSIDERATIONS (Emerging PG Topic)
- Obtain comprehensive 3-generation family history in all PPCM patients
- Perform clinical cardiac screening of first-degree relatives (echo, ECG)
- Offer genetic testing - TTN truncating variants in ~15%; also DSP, MYH7, LMNA, SCN5A
- Positive genetic test = worse prognosis AND family member risk
- Treat PPCM like DCM genetically - follow same guidelines for family counseling
SUMMARY TABLE FOR EXAMS
| Feature | Key Point |
|---|---|
| Definition | LV systolic dysfunction (LVEF <45%) in last month of pregnancy or within 5 months postpartum, no other cause |
| Most common timing | First 2 weeks postpartum |
| Incidence (USA) | 1:1000 to 1:4000 deliveries |
| Highest incidence | Africa (1:100), Haiti (1:300) |
| Highest risk group | Black/African-American women (5-15x) |
| Key pathophysiology | Prolactin → Cathepsin D → 16 kDa fragment + sFLT-1 + TTN genetic risk |
| Diagnosis | Echocardiography (LVEF <45%) - diagnosis of exclusion |
| Contraindicated in pregnancy | ACEi, ARB, sacubitril-valsartan, spironolactone, warfarin, ivabradine |
| Safe vasodilator in pregnancy | Hydralazine + isosorbide dinitrate |
| Anticoagulation agent | LMWH (preferred over UFH; warfarin contraindicated antepartum) |
| Bromocriptine | Inhibits prolactin; experimental; suppresses lactation |
| Recovery rate (USA) | 50-80% within 2-6 months |
| Worst prognostic sign | LVEF <30% + LVEDD >6.0 cm + Black race + late diagnosis |
| Subsequent pregnancy risk | 20% with recovered LV; 40-50% + 19% mortality with persistent dysfunction |
| Genetic link | TTN truncating variants in ~15% |
RECENT EVIDENCE (2024-2025) - Stay Updated
| Study | Key Finding |
|---|---|
| PMID 41213878 (2025 Meta-analysis, ESC Heart Fail) | Bromocriptine associated with improved LV recovery in PPCM; needs large RCT confirmation |
| PMID 40819912 (2025 Meta-analysis, Open Heart) | RV dysfunction in PPCM is prevalent and associated with significantly worse outcomes |
| PMID 39295149 (2025 Meta-analysis, ESC Heart Fail) | Cardiac MRI - late gadolinium enhancement predicts failure of LV recovery |
| PMID 40308031 (2025 Meta-analysis, Acta Obstet Gynecol) | Subsequent pregnancy after PPCM: significant maternal risk especially with persistent dysfunction |
| PMID 40701904 (2025 Meta-analysis, Heart Lung Circ) | Systematic review confirming key risk factors: Black race, preeclampsia, multiparity, advanced age |
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Fuster and Hurst's The Heart 15th Ed. (Chapter 51, Elkayam & Pizula) | Braunwald's Heart Disease 11th Ed. | Goldman-Cecil Medicine | Creasy & Resnik's Maternal-Fetal Medicine | ROSEN's Emergency Medicine | Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.