All about facial paralysis diagnosis treatment
Reading File
Finding Sources
Finding Sources
Searching Images
facial paralysis Bell's palsy diagnosis clinical features
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive review of facial paralysis — its diagnosis, classification, and treatment — drawn from Cummings Otolaryngology, Adams & Victor's Neurology, K.J. Lee's Essential Otolaryngology, and other authoritative texts.
Facial Paralysis: Diagnosis and Treatment
1. Overview and Epidemiology
Facial paralysis refers to weakness or complete loss of motor function in the muscles of facial expression, supplied by the facial nerve (CN VII). The most common form is Bell palsy, an idiopathic peripheral facial neuropathy.
- Annual incidence of Bell palsy: 23–37 per 100,000
- Equal sex ratio, except female predominance in women <20 years; slight male predominance in men >40 years
- Higher incidence in patients >65 years (59/100,000); lower in children <13 years (13/100,000)
- Left and right sides equally affected
- ~30% of patients present with incomplete paralysis; 70% with complete paralysis
- Bilateral facial paralysis occurs in only 0.3% — always warrants a diligent search for systemic causes
— Cummings Otolaryngology Head and Neck Surgery
2. Clinical Photograph
Below: An elderly female patient with left-sided unilateral facial nerve paralysis (House-Brackmann Grade V). Note flattening of the left forehead wrinkles, drooping of the left lower eyelid, and pronounced drooping of the left labial commissure with an effaced nasolabial fold.

3. Etiology and Differential Diagnosis
The "all that palsies are not Bell" dictum is critical. Facial paralysis has many causes:
| Acute Paralysis | Chronic/Progressive Paralysis |
|---|---|
| Bell palsy (most common, ~70%) | Primary parotid tumor |
| Ramsay Hunt syndrome (herpes zoster oticus, ~15%) | Metastatic tumor |
| Guillain-Barré syndrome | Schwannoma |
| Lyme disease (Borrelia burgdorferi) | Glomus tumor |
| Otitis media (acute or chronic) | Cholesteatoma |
| Temporal bone fracture / barotrauma | |
| Sarcoidosis (Heerfordt syndrome) | |
| HIV infection | |
| Melkersson-Rosenthal syndrome | |
| Möbius syndrome (bilateral CN VII + VI agenesis) | |
| Perinatal/birth trauma | |
| Mononucleosis, mumps, MS |
— Cummings Otolaryngology, K.J. Lee's Essential Otolaryngology
Bilateral Facial Paralysis
The most common causes are: Guillain-Barré syndrome (most common single cause), Bell palsy, sarcoidosis, Lyme disease, brainstem encephalitis, syphilis, leukemia, and bacterial meningitis. Workup should include lumbar puncture, autoantibody titers, VDRL, and MRI.
4. Pathophysiology of Bell Palsy
The best current evidence implicates reactivation of latent herpes simplex virus type 1 (HSV-1). Murakami et al. found HSV-1 DNA in the endoneurial fluid surrounding the facial nerve in 11 of 14 Bell palsy cases using PCR. VZV was found in none of these cases — confirming the distinction from Ramsay Hunt syndrome (where VZV is isolated exclusively).
The immediate mechanism of paralysis is edema and demyelination at the labyrinthine segment of the facial nerve within the fallopian canal, which is the narrowest portion and therefore the most susceptible to compression from swelling.
5. Diagnostic Criteria
Taverner's Minimum Diagnostic Criteria for Bell Palsy:
- Paralysis or paresis of all muscle groups of one side of the face
- Sudden onset
- Absence of CNS disease signs
- Absence of ear or cerebellopontine angle disease signs
Bell palsy is a diagnosis of exclusion, though experienced clinicians make it based on characteristic clinical features.
6. Clinical Features
| Feature | Detail |
|---|---|
| Pain behind the ear | Precedes paralysis by 1–2 days in many cases; occasionally intense |
| Dysgeusia (altered taste) | Chorda tympani involvement; usually resolves by week 2 |
| Hyperacusis | Stapedius muscle dysfunction; present in ~30% |
| Decreased lacrimation | Greater superficial petrosal nerve (GSPN) involvement; 17% |
| Facial/retroauricular pain | ~60% |
| Hypesthesia of CN V or glossopharyngeal nerve | ~80% (indicating cranial polyneuritis) |
| Incomplete eye closure (lagophthalmos) | Orbicularis oculi weakness; risk of corneal exposure |
| Bell's phenomenon | Upward rotation of eyeball on attempted eye closure |
Onset is acute — about half of cases reach maximum paralysis within 48 hours, and nearly all within 3–4 days. A careful neurologic exam will reveal other cranial nerve weaknesses in more than 50% of Bell palsy patients, reflecting the cranial polyneuritis nature of the disease.
7. Grading: House-Brackmann Scale
| Grade | Description |
|---|---|
| I | Normal |
| II | Slight weakness/asymmetry with movement |
| III | Obvious asymmetry with movement, possible synkinesis; complete eye closure possible |
| IV | Incomplete eye closure; no forehead movement; asymmetry at rest |
| V | Asymmetric at rest; minimal movement with effort |
| VI | No movement at all |
— K.J. Lee's Essential Otolaryngology
8. Diagnostic Workup
Electrodiagnostic Testing
Testing should not be performed in the first 3 days — Wallerian degeneration requires 48–72 hours to reach extratemporal segments.
| Test | Principle | Clinical Use |
|---|---|---|
| Nerve Excitability Test (NET) | Threshold stimulation to elicit twitch | Difference >2.0–3.5 mA between sides = unfavorable prognosis |
| Electroneuronography (ENoG) | Measures compound muscle action potential (CMAP) | ≥90% degeneration = poor recovery; indication for surgical decompression |
| Electromyography (EMG) | Detects motor unit potentials | Fibrillation = denervation; polyphasic potentials = reinnervation |
| Nerve Conduction Velocity | Measured at stylomastoid foramen | <10 m/s = poor outcome; 37–58 m/s = good outcome |
ENoG is the cornerstone prognostic test. Excellent recovery occurs universally when degeneration does not reach 90%. The combination of ENoG with EMG is most useful — patients with preserved voluntary motor potentials despite reduced CMAP have excellent prognoses.
Topodiagnostic Tests
- Schirmer test: evaluates greater petrosal nerve function (lacrimal secretion)
- Stapedial reflex: evaluates the nerve to stapedius
- Taste testing / submandibular salivary flow: evaluates chorda tympani
Note: Accuracy of topodiagnostic localization in Bell palsy is disappointing due to the diffuse nature of demyelination.
Imaging
Gadolinium-enhanced MRI: Enhancement of the facial nerve is common even in healthy individuals; the most consistent finding in Bell palsy is enhancement of the distal meatal and labyrinthine segments. Enhancement degree does not correlate with recovery. MRI is not essential in typical Bell palsy but is indicated in:
- Progressive palsy over 3 weeks
- Recurrent palsy
- Facial hyperkinesis
- Development of associated cranial neuropathies
These features may indicate neoplastic involvement.
9. Prognosis
- 80–90% of Bell palsy patients recover completely
- Incomplete paralysis at presentation: 95–100% recover with no sequelae
- Recovery of taste in the first week = good prognostic sign
- Early return of motor function in days 5–7 = most favorable sign
- EMG showing denervation after 10 days = long recovery (months to years)
- Recurrence occurs in ~8–9% of cases
- Poor prognostic factors: age >60, complete paralysis, hyperacusis, decreased tearing, diabetes, hypertension, severe pain
10. Management
Management Algorithm
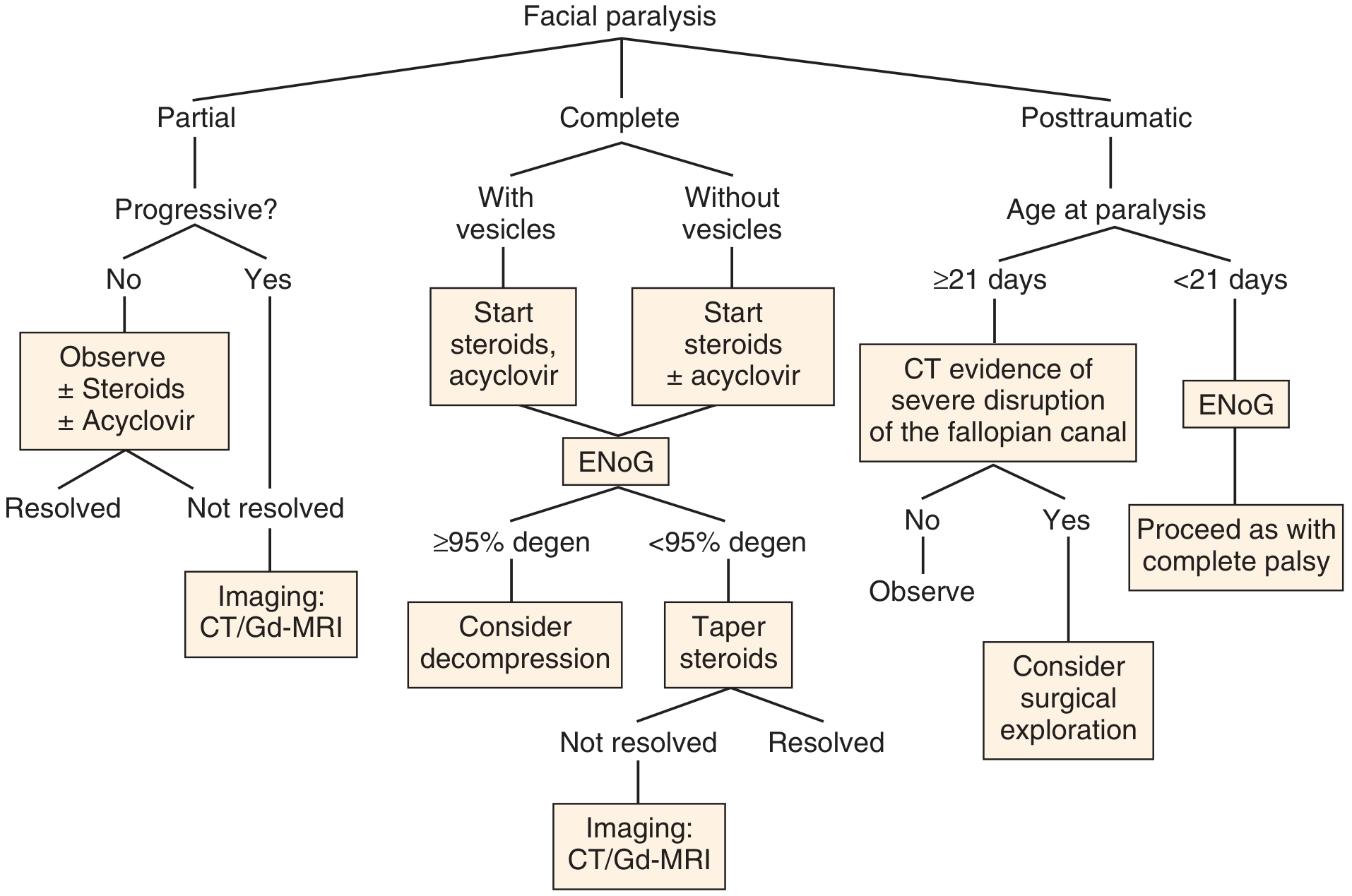
A. Corticosteroids
The cornerstone of treatment. Meta-analysis by Ramsey et al. showed treated patients had a 17% better chance of complete recovery; odds of recovery with steroids: 49–97% vs. 23–64% without.
- Prednisone 1 mg/kg/day for 10 days, then taper over 10 days
- Must be started within 48 hours of onset for maximum benefit
- Less evidence of benefit in children
- A Cochrane review (2,280 participants) found moderate-quality evidence that combination therapy (antivirals + corticosteroids) reduces synkinesis and excessive tearing vs. corticosteroids alone
B. Antiviral Agents
Evidence is mixed but antivirals are commonly added, especially in severe cases:
- Acyclovir 400 mg five times daily (option if seen within first 3 days)
- Valacyclovir 1,000 mg TID — may be more effective, particularly for Ramsay Hunt syndrome
- Sullivan et al.'s four-arm RCT: significant improvement with prednisolone alone, but no additional benefit from acyclovir beyond steroids
- Combination therapy is recommended for Ramsay Hunt syndrome (acyclovir + prednisone)
C. Eye Care
Lagophthalmos risks corneal exposure and ulceration:
- Lubricating eye drops during the day
- Eye ointment at night
- Eye taping or patching during sleep
- Moisture chambers in severe cases
D. Surgical Decompression
Indicated when ENoG shows ≥90% degeneration and no voluntary motor potentials on EMG within 2 weeks of onset:
- Decompression targets the meatal foramen and labyrinthine segment
- Gantz et al.: 91% of surgical patients achieved HB Grade I or II vs. 42% with steroids alone in this subgroup
- Timing is critical — must be within the first 2 weeks
E. Rehabilitation
| Modality | Notes |
|---|---|
| Botulinum toxin (Botox) | For synkinesis — particularly eyelid synkinesis; lowest effective dose ~40 units into orbicularis oculi |
| Physical therapy / mime therapy | Level C evidence; meta-analyses show modest benefit |
| Neuromuscular re-education / biofeedback | Visual biofeedback using mirrors; assists compensation for muscular weakness |
| Facial reanimation surgery | For permanent palsy; static (slings, muscle transfer) or dynamic (nerve grafts) reconstruction |
11. Special Situations
Ramsay Hunt Syndrome (Herpes Zoster Oticus)
- Caused by VZV reactivation (not HSV)
- Features: vesicular rash on the pinna, conchal bowl, retroauricular area, face, or mouth + facial palsy + otalgia
- Higher risk of complete nerve degeneration vs. Bell palsy
- ~10% have rash appearing after facial paralysis — do not miss this diagnosis
- Cochlear and vestibular disturbances more common
- Treatment: acyclovir + prednisone (combined)
Lyme Disease
- Borrelia burgdorferi; can cause unilateral or bilateral facial palsy (3:1 ratio)
- "Bull's eye" rash (erythema migrans)
- Treatment: tetracycline (adults), penicillin (children)
Otitis Media-Associated Palsy
- AOM: amoxicillin + myringotomy
- CSOM: surgical removal of disease + nerve decompression
Sarcoidosis (Heerfordt Syndrome)
- Uveitis + parotid enlargement + mild fever + CN palsy
- Facial nerve most commonly involved (may be bilateral)
- Elevated serum ACE generally confirms the diagnosis
- Requires systemic steroids
Melkersson-Rosenthal Syndrome
- Triad: recurrent unilateral facial palsy + facial edema + fissured tongue (lingua plicata)
Pregnancy
- Possible increased incidence in the third trimester and first 2 weeks postpartum (up to threefold in some series, though disputed)
Summary Table
| Aspect | Key Points |
|---|---|
| Most common cause | Bell palsy (~70%) — HSV-1 reactivation |
| Diagnosis | Clinical (Taverner's criteria); exclusion of other causes |
| Grading | House-Brackmann I–VI |
| Key electrodiagnostic test | ENoG — ≥90% degeneration = poor prognosis |
| First-line treatment | Prednisone 1 mg/kg × 10 days, started within 48h |
| Antivirals | Added for severe cases; mandatory in Ramsay Hunt |
| Eye protection | Critical to prevent corneal damage |
| Surgical decompression | ENoG ≥90% degen + no voluntary EMG potentials within 2 weeks |
| Prognosis | 80–90% complete recovery overall |
Sources: Cummings Otolaryngology Head and Neck Surgery; Adams and Victor's Principles of Neurology, 12th Ed.; K.J. Lee's Essential Otolaryngology; Harrison's Principles of Internal Medicine 22E; ROSEN's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.