reproductive system patholgy explain me everything i dont know anything from refernce of book
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have more than enough content from Robbins to give you a complete, well-structured explanation. Here is the full guide:
Reproductive System Pathology - Complete Guide
Based on: Robbins & Kumar Basic Pathology + Robbins, Cotran & Kumar Pathologic Basis of Disease
PART 1: FEMALE GENITAL SYSTEM
1. VULVA
Vulvitis
Inflammation of the vulva is common and usually a result of infection (Candida, Trichomonas, herpes). Constant moisture and chemical irritants contribute.
Nonneoplastic Epithelial Disorders
Lichen Sclerosus
- Thinning of the epidermis, loss of rete ridges, and dense fibrous tissue in dermis
- White, parchment-like plaques on vulva
- Seen in postmenopausal women and young girls
- Associated with slightly increased risk of squamous cell carcinoma (SCC)
Squamous Cell Hyperplasia (Lichen Simplex Chronicus)
- Hyperkeratosis and acanthosis (thickening) of the epithelium
- Caused by chronic rubbing/scratching
- White, thickened skin patches
Tumors of the Vulva
Condylomas (Genital Warts)
- Caused by HPV (low-risk types 6 and 11)
- Two types:
- Condyloma acuminatum - raised, verrucous (cauliflower-like) lesion; benign
- Condyloma latum - flat lesion of secondary syphilis; NOT HPV related
- Histology: koilocytes (vacuolated cells with wrinkled nuclei = pathognomonic for HPV)
Carcinoma of the Vulva
- ~3% of female genital cancers
- Two pathways:
- HPV-related (younger women): High-risk HPV (16, 18) → VIN (Vulvar Intraepithelial Neoplasia) → basaloid/warty SCC
- Non-HPV-related (older women): Background of lichen sclerosus → keratinizing SCC
- Spreads to inguinal, then pelvic lymph nodes
Extramammary Paget Disease
- Paget cells (large cells with pale cytoplasm) in the vulvar epithelium
- Presents as red, crusted, eczematous lesion
- Unlike breast Paget, vulvar Paget usually has NO underlying carcinoma (only ~25% do)
2. VAGINA
Vaginitis
- Most common cause: Gardnerella vaginalis (bacterial vaginosis) - "fishy" odor, clue cells on smear
- Trichomonas vaginalis - strawberry cervix, flagellated protozoan
- Candida albicans - cottage cheese discharge, pseudohyphae on KOH prep
- Mucosal atrophy in postmenopausal women → atrophic vaginitis
Malignant Neoplasms
Squamous Cell Carcinoma of Vagina
- Rare; mainly in older women
- Most are extensions from cervical carcinoma
Embryonal Rhabdomyosarcoma (Sarcoma Botryoides)
- Most common vaginal tumor in infants and children under 5
- Gross: grape-like polypoid masses protruding from vagina
- Micro: "cambium layer" - dense zone of malignant rhabdomyoblasts beneath the epithelium
- Highly aggressive but responds to combination therapy
3. CERVIX
Cervicitis
- Extremely common; often asymptomatic
- Acute cervicitis: Chlamydia trachomatis (#1 STI cause), Neisseria gonorrhoeae, HSV
- Chronic cervicitis: Most common; caused by normal vaginal flora
Endocervical Polyp
- Benign, soft, pedunculated, mucus-secreting mass in cervical canal
- Presents with abnormal vaginal bleeding
- Treated by simple excision
Neoplasia of the Cervix - VERY HIGH YIELD
HPV and Cervical Cancer - The Key Link
- Nearly ALL cervical cancers caused by high-risk HPV (types 16 and 18)
- HPV proteins E6 (degrades p53) and E7 (inactivates Rb) = drive malignant transformation
- The transformation zone (squamocolumnar junction) is the critical target area
Squamous Intraepithelial Lesion (SIL) / Cervical Intraepithelial Neoplasia (CIN)
| Grade | Also Called | Description |
|---|---|---|
| CIN 1 (Low-grade SIL) | LSIL | Mild dysplasia; lower 1/3 of epithelium involved; mostly regresses |
| CIN 2 (High-grade SIL) | HSIL | Moderate; lower 2/3 involved |
| CIN 3 (High-grade SIL) | HSIL | Severe dysplasia/carcinoma in situ; full thickness |
- Pap smear is the gold-standard screening tool
- Koilocytes = pathognomonic of HPV infection on Pap smear
Invasive Carcinoma of the Cervix
- Squamous cell carcinoma = 80% (from exocervix, SIL)
- Adenocarcinoma = 20% (from endocervical glands, also HPV-related)
- Clinical: abnormal vaginal bleeding (especially postcoital), watery discharge
- Spreads locally → bladder, rectum, then lymphatics
- FIGO staging determines treatment:
- Stage I: Confined to cervix
- Stage II: Beyond cervix, not to pelvic wall
- Stage III: To pelvic wall or lower 1/3 vagina
- Stage IV: Bladder/rectum or distant
4. UTERUS
Endometritis
- Acute: Postpartum, post-abortion; caused by Group B Streptococcus, Staphylococcus; retained products of conception predispose
- Chronic: Chlamydia, gonorrhea, TB (in endemic areas); plasma cells in endometrium = diagnostic hallmark (plasma cells are NOT normally present in endometrium)
Adenomyosis
- Endometrial glands and stroma present deep within the myometrium
- Causes: uterine enlargement, dysmenorrhea, menorrhagia
- Differs from endometriosis (adenomyosis is INSIDE the uterine wall, not outside)
Endometriosis
- Endometrial glands/stroma outside the uterus
- Common sites: ovaries (#1), uterine ligaments, rectovaginal septum, pelvic peritoneum
- Classic triad: dysmenorrhea, dyspareunia, infertility
- Ovaries → "chocolate cysts" (endometriomas filled with old blood)
- Theories of origin: retrograde menstruation (Sampson), coelomic metaplasia
- Responds to hormonal therapy (estrogen-suppressive) or surgical excision
Abnormal Uterine Bleeding
- Most common cause varies by age:
- Reproductive age: anovulation → unopposed estrogen → endometrial hyperplasia
- Postmenopausal: endometrial carcinoma until proven otherwise
- Also: fibroids (leiomyomas), polyps, coagulation defects
Proliferative Lesions of the Endometrium and Myometrium
Endometrial Hyperplasia
- Caused by unopposed estrogen (anovulation, obesity, HRT without progesterone, estrogen-secreting ovarian tumors)
- Classification:
- Simple hyperplasia (without atypia): Low risk of cancer (~1%)
- Complex hyperplasia (without atypia): ~3% risk
- Simple/Complex with atypia (EIN - Endometrial Intraepithelial Neoplasia): ~30% risk of carcinoma; precursor lesion
- Treated with progestins or hysterectomy if atypia present
Endometrial Carcinoma
- Most common gynecologic malignancy in the US (NOT the most common cause of cancer death - ovarian is more deadly)
- Two types:
| Feature | Type I (Endometrioid) | Type II (Serous/Clear Cell) |
|---|---|---|
| Age | Younger, peri-menopausal | Older, postmenopausal |
| Background | Hyperplasia, unopposed estrogen | Atrophic endometrium |
| Grade | Low-grade | High-grade |
| Genes | PTEN, KRAS, microsatellite instability, PIK3CA | TP53 |
| Prognosis | Better | Worse |
- Presents as postmenopausal bleeding (#1 symptom)
- Diagnosis: endometrial biopsy
- Treatment: hysterectomy + bilateral salpingo-oophorectomy ± radiation
Endometrial Polyps
- Benign, protruding masses of endometrial glands and stroma
- Cause abnormal uterine bleeding
- Small malignant potential
Uterine Leiomyoma (Fibroids)
- Most common tumor in women; found in ~25% of reproductive-age women
- Benign smooth muscle tumors of the myometrium
- Estrogen-dependent → grow during reproductive years, shrink after menopause
- Gross: well-circumscribed, firm, whorled white masses
- Multiple types: intramural, submucosal (bleed most), subserosal
- Symptoms: menorrhagia, pelvic pressure, urinary symptoms
- Most are asymptomatic; treatment if symptomatic (myomectomy, hysterectomy, GnRH agonists)
Leiomyosarcoma
- Malignant smooth muscle tumor; usually arises de novo (NOT from pre-existing leiomyoma)
- More common in older/postmenopausal women
- Criteria: >10 mitoses per 10 HPF, coagulative tumor cell necrosis, cytologic atypia
- Poor prognosis
5. FALLOPIAN TUBES
Salpingitis (Pelvic Inflammatory Disease - PID)
- Most common cause of fallopian tube pathology
- Agents: Chlamydia trachomatis (#1), N. gonorrhoeae; often polymicrobial
- Leads to: hydrosalpinx (tube distended with fluid), pyosalpinx (pus), adhesions
- Major complication: ectopic (tubal) pregnancy (risk increases 6-10x with prior salpingitis)
- Also causes infertility via tubal scarring
Ectopic Pregnancy
- 95% in fallopian tube (ampulla most common site)
- Risk factors: prior PID, previous ectopic, endometriosis, IUD
- Presents with: missed period, pelvic pain, rupture → surgical emergency
- Rupture → hemoperitoneum, shock
6. OVARIES
Follicle and Luteal Cysts
- Common, usually asymptomatic
- Follicular cysts: unruptured Graafian follicle lined by granulosa cells; may cause pain or abnormal bleeding
- Corpus luteum cysts: may cause delayed menstruation, rupture → hemoperitoneum
Polycystic Ovarian Syndrome (PCOS)
- Most common endocrine disorder in women of reproductive age
- Features: oligomenorrhea/amenorrhea, hirsutism, obesity, infertility
- Labs: elevated LH:FSH ratio (>2:1), elevated androgens, insulin resistance
- Grossly: enlarged ovaries with multiple small follicular cysts (≤1 cm), thickened cortex
- Long-term risk: endometrial hyperplasia/carcinoma (from unopposed estrogen), type 2 diabetes, metabolic syndrome
Tumors of the Ovary - HIGH YIELD
Overview
- 80% arise from surface epithelium (covering of ovary = modified peritoneum)
- Risk factors: family history (BRCA1/2), nulliparity, early menarche, late menopause
- Protective: OCPs, multiparity, breastfeeding, tubal ligation
Surface Epithelial Tumors (80%)
(A) Serous Tumors
- Most common ovarian tumors
- Lined by Fallopian tube-type epithelium (tall, ciliated columnar cells)
- Types: Benign (serous cystadenoma), Borderline, Malignant (serous cystadenocarcinoma)
- Serous cystadenocarcinoma = most common ovarian malignancy
- Psammoma bodies (laminated calcified concentric spheres) = characteristic finding in serous carcinoma
- Bilateral in ~30% of malignant cases
- Genetic: low-grade → KRAS/BRAF mutations; high-grade → TP53 mutations
(B) Mucinous Tumors
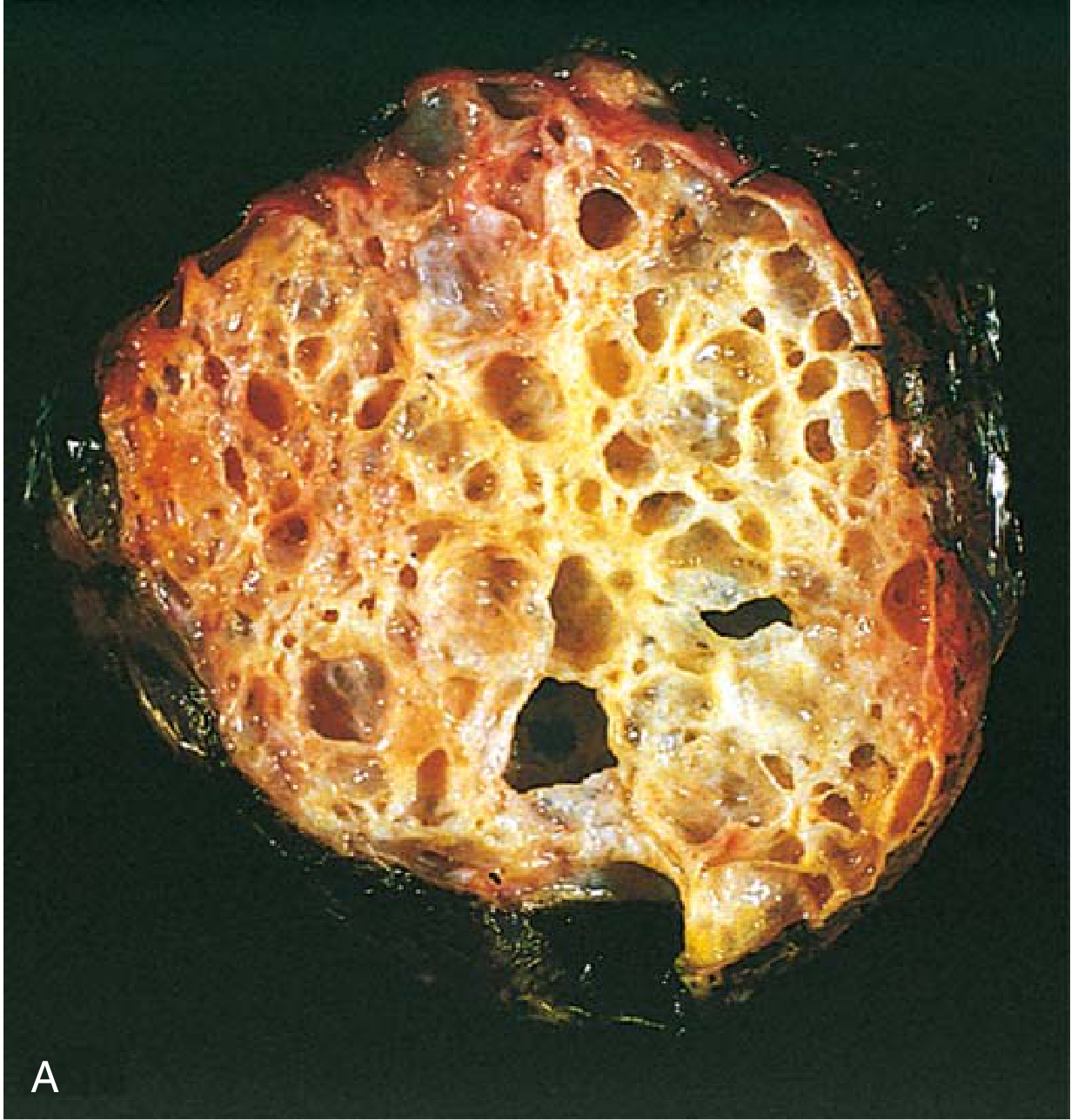
- Lined by mucin-secreting columnar cells (resembling endocervical or intestinal epithelium)
- Tend to be large, multilocular
- Rupture → pseudomyxoma peritonei (jelly-like mucin filling peritoneal cavity)
- Bilateral in only ~5% of benign cases
- Less common than serous
(C) Endometrioid Tumors
- Glands resembling endometrium
- Usually malignant
- 15-20% coexist with endometrial carcinoma (synchronous tumors)
- Mutations: PTEN, PI3K-AKT pathway
(D) Clear Cell Carcinoma
- Large cells with clear cytoplasm
- Associated with endometriosis
- Same mutations as endometrioid (PIK3CA, ARID1A, KRAS, PTEN, TP53)
Germ Cell Tumors (15%)
(A) Teratomas
-
15-20% of ovarian tumors; >90% are benign
-
Mature (Dermoid Cyst):
- Contains fully differentiated tissues from all 3 germ layers (skin, hair, teeth, thyroid, bronchial epithelium)
- Most common ovarian tumor in young women and children
- Usually unilateral (right side more common)
- Usually <10 cm
- Risk: torsion; rarely malignant transformation (SCC most common)
-
Immature Teratoma:
- Contains immature (fetal) tissue, especially immature neural elements
- Malignant; occurs in first 2 decades
- Graded 1-3 based on amount of immature neural tissue
-
Monodermal Teratoma:
- Struma ovarii (thyroid tissue) → can cause hyperthyroidism
- Carcinoid tumors
(B) Dysgerminoma
- Counterpart of testicular seminoma
- Most common malignant germ cell tumor of ovary
- Occurs in young women
- Radiosensitive; excellent prognosis
- Cells: large, pale, glycogen-rich; lymphocytic infiltrate + fibrous septa
(C) Yolk Sac Tumor (Endodermal Sinus Tumor)
- Occurs in children/young adults
- Produces AFP (alpha-fetoprotein) = tumor marker
- Schiller-Duval bodies (perivascular structures resembling fetal glomeruli)
Sex Cord-Stromal Tumors (5%)
(A) Granulosa Cell Tumor
- Most common malignant stromal tumor
- Produces estrogen → precocious puberty (in children) or postmenopausal bleeding
- Call-Exner bodies (small follicle-like structures with eosinophilic fluid) = pathognomonic
- Tumor marker: Inhibin
- Low-grade malignancy; late recurrence possible
(B) Thecoma-Fibroma
- Fibroma: benign, fibrous stromal cells; associated with Meigs syndrome (ovarian fibroma + ascites + hydrothorax)
- Thecoma: produces estrogen
(C) Sertoli-Leydig Cell Tumor (Androblastoma)
- Produces androgens → virilization
- Low malignant potential
7. GESTATIONAL TROPHOBLASTIC DISEASE (GTD)
A spectrum of tumors arising from the placental trophoblast.
| Entity | Features | hCG |
|---|---|---|
| Hydatidiform Mole (Complete) | No fetal parts; all cells diploid (46,XX paternal); grape-like villi; ~2-3% → choriocarcinoma | Very high |
| Hydatidiform Mole (Partial) | Fetal parts present; triploid (69,XXX or 69,XXY); rarely → choriocarcinoma | High |
| Choriocarcinoma | Highly malignant; no villi; sheets of cyto- and syncytiotrophoblasts; early hematogenous spread (lungs #1) | Extremely high |
| Placental Site Trophoblastic Tumor | Rare; produces HPL (human placental lactogen); may not produce much hCG | Variable |
- Complete mole karyotype: 46,XX (both chromosomes paternal - "androgenetic diploid")
- All GTD monitored by serial serum beta-hCG levels
- Choriocarcinoma is HIGHLY chemosensitive (methotrexate, actinomycin-D); excellent cure rates even with metastases
PART 2: MALE GENITAL SYSTEM
8. PENIS
Congenital Anomalies
- Hypospadias: Urethral opening on ventral (under) surface of penis - more common (~1/300 births)
- Epispadias: Urethral opening on dorsal (upper) surface - less common
- Both can cause: urinary obstruction, ascending infections, infertility (if at base of penis)
Phimosis
- Prepuce (foreskin) orifice too small to retract over glans
- Causes: congenital or acquired (from recurrent infections and scarring)
- Complications: accumulation of smegma → secondary infections → increased risk of penile carcinoma
Inflammation
- Balanoposthitis: Infection of glans + prepuce; organisms include Candida, anaerobes, Gardnerella
- More common in uncircumcised males
Tumors of the Penis
Condyloma Acuminatum
- Benign wart from HPV types 6 and 11
- Histology: koilocytes; papillary lesion
Penile Intraepithelial Neoplasia (PIN) / Carcinoma In Situ
- Three histologic subtypes; all caused by high-risk HPV 16, 18:
- Bowen Disease: Leukoplakia-like plaque on shaft
- Erythroplasia of Queyrat: Red, velvety, moist plaque on glans (higher risk of invasive carcinoma)
- Bowenoid Papulosis: Multiple small papules; occurs in younger men; rarely progresses
Squamous Cell Carcinoma of the Penis
- ~1% of male cancers in the US
- Risk factors: phimosis, HPV 16/18, poor hygiene, no circumcision (circumcision is protective)
- Slow-growing, spreads to inguinal → iliac lymph nodes
- Prognosis depends on lymph node involvement
9. TESTIS
Cryptorchidism (Undescended Testis)
- ~1% of males at 1 year of age
- Most common anomaly of male genitalia
- Risk: germ cell tumors (3-5x increased risk, even in contralateral testis); infertility
- Histology: tubular atrophy, Leydig cell hyperplasia, basement membrane thickening
- Treatment: orchiopexy before age 2 (improves fertility; does NOT eliminate cancer risk)
Orchitis
- Granulomatous orchitis: Idiopathic; presents as painless testicular mass
- Mumps orchitis: In post-pubertal males (prepubertal = usually asymptomatic); 20-30% bilateral → infertility
Testicular Torsion
- Twisting of spermatic cord → venous obstruction → arterial ischemia → infarction
- Classic "bell-clapper deformity" (improperly attached tunica vaginalis)
- Surgical emergency; must be corrected within 4-6 hours
Testicular Tumors - HIGH YIELD
- Most common cancer in males aged 15-35
- 95% are germ cell tumors
- Risk factors: cryptorchidism, Klinefelter syndrome, family history
- Presents as painless testicular mass (pain = late or torsion)
- Tumor markers: AFP, beta-hCG, LDH
Classification:
| Tumor | Age | Marker | Features | Behavior |
|---|---|---|---|---|
| Seminoma | 30-40 | hCG (10%) | Large pale cells, lymphocytic infiltrate, fibrous septa; PLAP+ | Radiosensitive; excellent prognosis |
| Embryonal Carcinoma | 20-30 | AFP, hCG | Poorly differentiated, necrosis, hemorrhage; aggressive | Aggressive |
| Yolk Sac Tumor | Infants (most common in children) | AFP | Schiller-Duval bodies; yellow, mucinous | Malignant |
| Choriocarcinoma | 20-30 | hCG (very high) | Hemorrhagic; hematogenous spread to lungs first | Most aggressive |
| Teratoma | Any age | None typically | Multiple tissue types; benign in children, malignant in adults | Varies |
| Mixed | Any adult | Varies | Most common type in adults | Varies |
Seminoma vs. Non-seminoma distinction is clinically important:
- Seminoma: radiosensitive, spreads to para-aortic nodes first, excellent cure
- Non-seminoma: chemotherapy (BEP - bleomycin, etoposide, cisplatin)
Spermatocytic Tumor (formerly spermatocytic seminoma)
- Older men (>50)
- No known association with cryptorchidism
- Benign behavior; does NOT metastasize
10. EPIDIDYMIS AND SPERMATIC CORD
Epididymitis
- Most common cause:
- Young sexually active men: Chlamydia trachomatis or N. gonorrhoeae
- Older men or children: E. coli, Pseudomonas (from UTI)
- Clinical: painful testicular swelling, fever; Prehn sign (elevation of testis relieves pain in epididymitis - helps distinguish from torsion)
11. PROSTATE
Benign Prostatic Hyperplasia (BPH)
- Extremely common in men >50 (50% by age 60, 90% by age 80)
- Hyperplasia (not hypertrophy) of both glandular epithelium AND stromal smooth muscle
- Occurs in the central/transitional zone (periurethral zone)
- Obstructive symptoms (LUTS): hesitancy, poor stream, dribbling, nocturia, urinary retention
- PSA may be mildly elevated
- Histology: nodular glandular and stromal proliferation with corpora amylacea (prostatic concretions)
- Treatment: alpha-blockers (tamsulosin), 5-alpha-reductase inhibitors (finasteride), surgery (TURP)
Prostatitis
- Acute bacterial: Fever, dysuria, perineal pain; E. coli most common; PSA elevated
- Chronic bacterial: Recurrent UTIs, perineal discomfort; E. coli most common
- Chronic pelvic pain syndrome (non-bacterial): Most common form; no organism identified
- Granulomatous prostatitis: After BCG therapy for bladder cancer
Prostatic Adenocarcinoma - VERY HIGH YIELD
- Most common cancer in men in the US
- Second most common cause of cancer death in men (after lung)
- Risk factors: age (>50), African-American race, family history, high-fat diet
- Arises in the peripheral zone (posterior aspect, palpable on DRE)
- Often initially asymptomatic (contrast with BPH which is symptomatic)
- Symptoms when advanced: obstructive symptoms, bone pain (osteoblastic metastases - lumbar spine most common)
Grading - Gleason Score
- Based on glandular architecture (not cytology)
- Grade 1 = well-formed glands; Grade 5 = no glandular differentiation
- Gleason score = primary pattern + secondary pattern (most common + second most common)
- Range: 2-10; higher score = worse prognosis
- Grade Groups 1-5 (modern system):
- Grade Group 1 = Gleason ≤6 (low risk)
- Grade Group 5 = Gleason 9-10 (very high risk)
Molecular Pathology
- Most common driver: TMPRSS2-ERG gene fusion (androgen-regulated TMPRSS2 promoter fused to ETS transcription factor ERG) → androgen-dependent overexpression of ERG
- Other: PTEN loss, TP53 mutations in advanced disease
PSA (Prostate-Specific Antigen)
- Organ-specific (not cancer-specific) serine protease
- Elevated in: cancer, BPH, prostatitis, trauma
- PSA density, PSA velocity, free:total PSA ratio improve specificity
- Screening: controversial; benefits vs. overdiagnosis
TNM Staging (Pathologic)
| Stage | Description |
|---|---|
| pT2 | Organ confined |
| pT3a | Extraprostatic extension |
| pT3b | Invades seminal vesicles |
| pT4 | Invades bladder/rectum/pelvic wall |
Treatment
- Localized: radical prostatectomy or radiotherapy (external beam or brachytherapy)
- Metastatic: androgen deprivation therapy (ADT) via orchiectomy OR LHRH agonists (leuprolide, goserelin) - desensitize pituitary → suppress LH → reduce testosterone
- Castration-resistant prostate cancer (CRPC): enzalutamide, abiraterone
SUMMARY TABLE: KEY Tumor Markers
| Tumor | Marker |
|---|---|
| Endodermal sinus tumor (Yolk Sac) | AFP |
| Choriocarcinoma | beta-hCG |
| Granulosa cell tumor | Inhibin |
| Sertoli-Leydig cell tumor | Testosterone |
| Prostate cancer | PSA |
| Gestational trophoblastic disease | beta-hCG |
| Mature teratoma (struma ovarii) | Thyroid hormones |
SUMMARY TABLE: Key Histologic Findings
| Pathognomonic Finding | Disease |
|---|---|
| Koilocytes | HPV infection |
| Psammoma bodies | Serous cystadenocarcinoma ovary |
| Call-Exner bodies | Granulosa cell tumor |
| Schiller-Duval bodies | Yolk sac tumor |
| Cambium layer | Embryonal rhabdomyosarcoma |
| Chocolate cyst | Ovarian endometrioma |
| Reinke crystals | Leydig cell tumor |
| Plasma cells in endometrium | Chronic endometritis |
| Corpora amylacea | BPH |
SUMMARY TABLE: HPV Types to Know
| HPV Type | Disease |
|---|---|
| 6, 11 | Condyloma acuminatum (genital warts); low risk |
| 16, 18 | Cervical cancer, vulvar cancer, penile cancer, anal cancer; HIGH RISK |
| 16 | Most commonly found in cervical SCC |
| 18 | Most commonly found in cervical adenocarcinoma |
Sources:
- Robbins & Kumar Basic Pathology, Chapter 17: Female Genital System and Breast
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter on Male Genital Tract
This covers the complete scope of reproductive system pathology as taught in medical school. Let me know if you want any topic expanded further - for example, a deeper dive into ovarian tumor classification, GTD, or staging systems.
Create an ovarian and testicular tumor classification poster
Generating Image
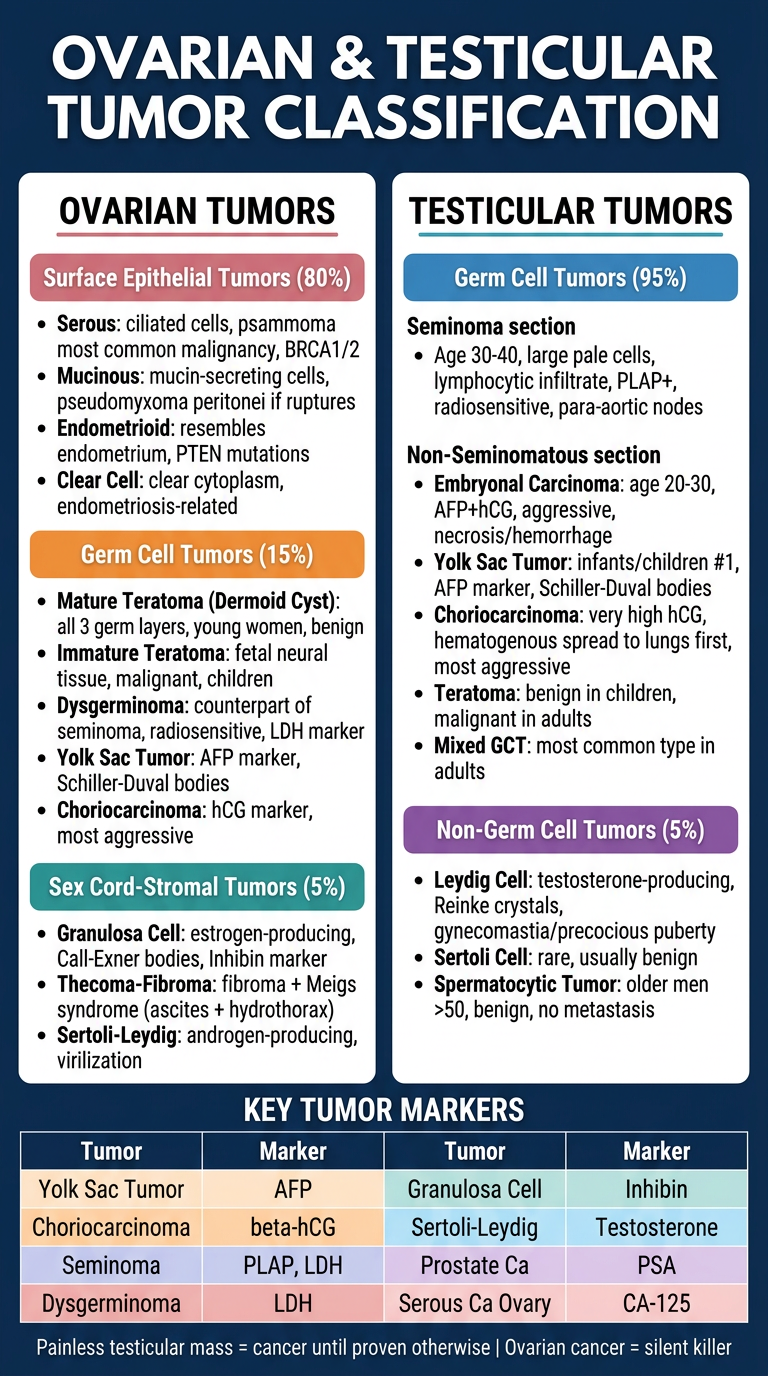
Here is your Ovarian & Testicular Tumor Classification Poster! It covers:
Ovarian side (left):
- Surface Epithelial Tumors (80%) - serous, mucinous, endometrioid, clear cell
- Germ Cell Tumors (15%) - teratoma, dysgerminoma, yolk sac, choriocarcinoma
- Sex Cord-Stromal Tumors (5%) - granulosa cell, thecoma-fibroma, Sertoli-Leydig
Testicular side (right):
- Seminoma vs. Non-seminomatous GCT breakdown
- Embryonal, yolk sac, choriocarcinoma, teratoma, mixed GCT
- Non-germ cell: Leydig, Sertoli, Spermatocytic tumor
Bottom bar: Quick-reference tumor markers table (AFP, hCG, Inhibin, PLAP, LDH, CA-125, PSA)
Let me know if you want a separate, more detailed poster for any specific subtopic - for example, just ovarian tumors with microscopic descriptions, or a Gleason grading poster for prostate cancer.
This is a shared conversation. Sign in to Orris to start your own chat.