Tell about heart failure
Reading File
Finding Sources
Searching Images
heart failure pathophysiology diagram
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, authoritative content from multiple textbooks. Let me compile the full answer.
Heart Failure
Definition
Heart failure (HF) is a complex clinical syndrome with symptoms and signs that result from any structural or functional impairment of ventricular filling or ejection of blood. The European Society of Cardiology emphasizes cardinal symptoms — breathlessness, ankle swelling, and fatigue — accompanied by signs such as elevated jugular venous pressure, pulmonary crackles, and peripheral edema, due to a structural and/or functional abnormality of the heart resulting in elevated intracardiac pressures and/or inadequate cardiac output at rest or during exercise.
Because some patients present without signs of volume overload, the term heart failure is preferred over the older term "congestive heart failure."
— Harrison's Principles of Internal Medicine 22E, p. 2019
Epidemiology
- ~6.7 million American adults are currently treated for HF; over 56.2 million people live with HF globally
-
600,000 new cases diagnosed each year in the United States
- Prevalence increases markedly with age: 1–2% at age 40–49 → ≥10% in adults over 80
- Lifetime risk: approximately 1 in 4 persons will develop HF
- Mortality remains ~50% within 5 years of diagnosis
- One-month rehospitalization after discharge is approximately 25%
— Harrison's Principles of Internal Medicine 22E, p. 2020; Textbook of Family Medicine 9e
Classification
By Ejection Fraction
| Type | EF | Mechanism |
|---|---|---|
| HFrEF (HF with reduced EF) | < 40–50% | Impaired LV systolic contraction |
| HFpEF (HF with preserved EF) | > 45–50% | Impaired LV filling/relaxation (diastolic dysfunction) |
HFpEF and HFrEF are nearly equally common. Fluid retention and pulmonary congestion are hallmarks of HF but are not universally present in either type.
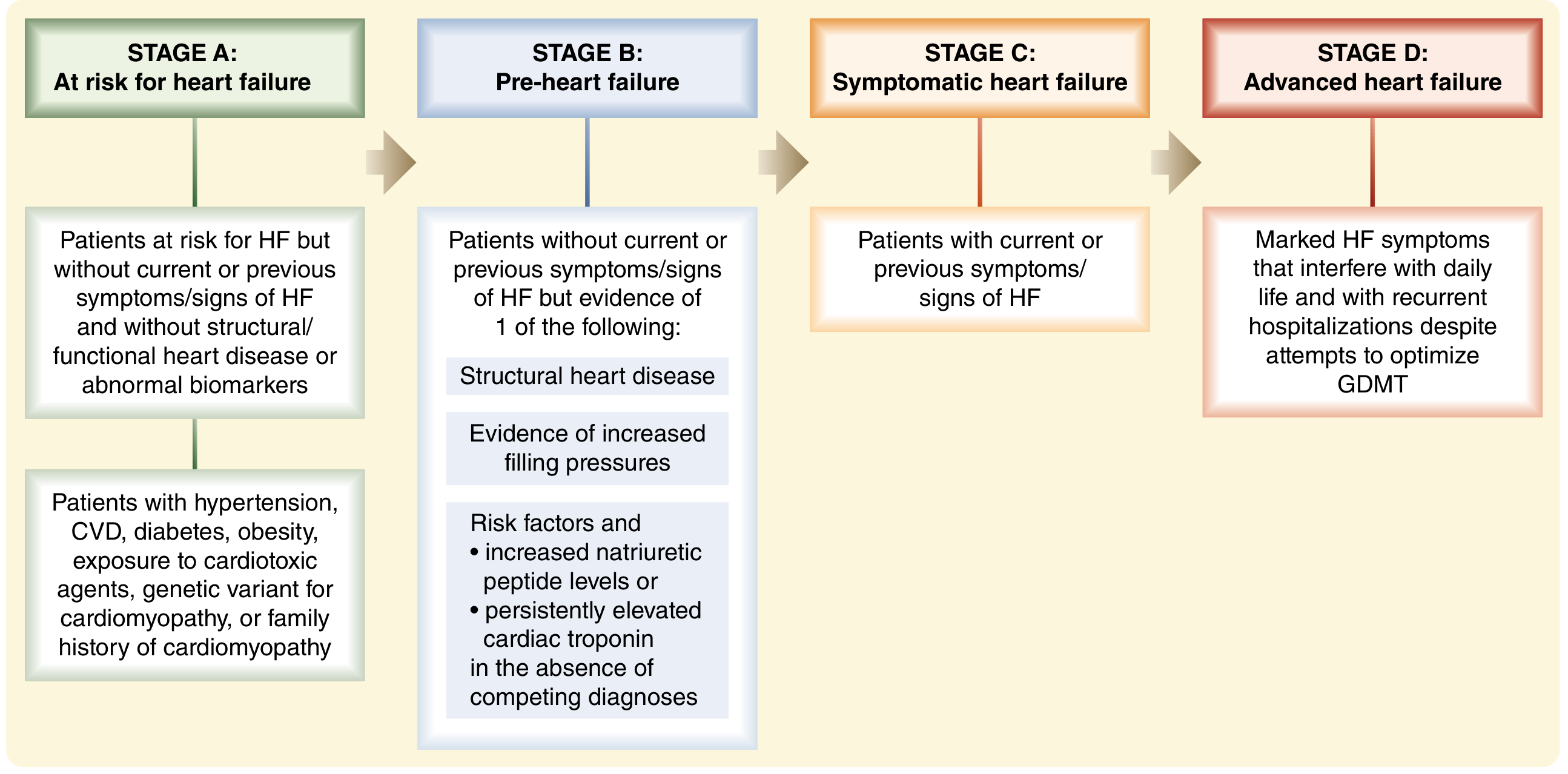
ACC/AHA Stages of Progression
| Stage | Description |
|---|---|
| A | At risk for HF but no structural disease or symptoms |
| B | Structural heart disease but no symptoms |
| C | Structural heart disease with prior or current symptoms |
| D | Refractory HF requiring advanced interventions |
NYHA Functional Classification
| Class | Limitation | Assessment |
|---|---|---|
| I | None | Ordinary activity does not cause symptoms |
| II | Mild | Comfortable at rest; ordinary activity causes symptoms |
| III | Moderate | Comfortable at rest; less-than-ordinary activity causes symptoms |
| IV | Severe | Symptoms at rest, worsen with any activity |
— Harrison's Principles of Internal Medicine 22E, p. 2024
Etiology
Common causes include:
- Ischemic cardiomyopathy (most common in adults in developed countries)
- Idiopathic dilated cardiomyopathy
- Hypertension (long-term pressure overload)
- Valvular heart disease (aortic stenosis, mitral regurgitation)
- Viral myocarditis
- Congenital heart disease
- Infiltrative conditions: amyloidosis, sarcoidosis
- Hypertrophic/restrictive cardiomyopathy
- Metabolic: diabetes mellitus, alcoholism, anemia, hyperthyroidism (high-output HF)
— Sabiston Textbook of Surgery, p. 1120; Textbook of Family Medicine 9e, p. 688
Pathophysiology
LV Remodeling
The central concept in modern HF pathophysiology is left ventricular remodeling — stretching and dilation of the LV with subsequent reduction in function. This is triggered by an index injury (MI, pressure overload, toxic exposure, etc.) and is — crucially — reversible with appropriate therapy.
- Concentric hypertrophy: increased mass out of proportion to chamber volume → pressure overload (e.g., hypertension, aortic stenosis)
- Eccentric hypertrophy: increased cavity size → volume overload (e.g., mitral/aortic regurgitation)
- Both are accompanied by myocyte hypertrophy, interstitial fibrosis, altered calcium-handling proteins, and re-expression of fetal genes
Neurohormonal Activation
Regardless of the precipitating injury, two major systems are activated and perpetuate remodeling:
-
Renin-Angiotensin-Aldosterone System (RAAS)
- Angiotensin II promotes myocyte apoptosis, hypertrophy, and ventricular fibrosis
- Aldosterone augments these effects and promotes adverse remodeling
- Aldosterone "escapes" angiotensin suppression — so selective aldosterone blockade is needed on top of ACE inhibitors/ARBs
-
Sympathetic Nervous System (SNS)
- Elevated catecholamines suppress β-adrenergic receptors
- Direct cardiotoxicity via cAMP-dependent calcium overload of myocytes
- Increased myocardial O₂ consumption and risk of fatal arrhythmias
Additional mediators include endothelin-1 (vasoconstriction), pro-inflammatory cytokines, matrix metalloproteinases (cardiac fibrosis and collagen deposition), and vasopressin (fluid retention).
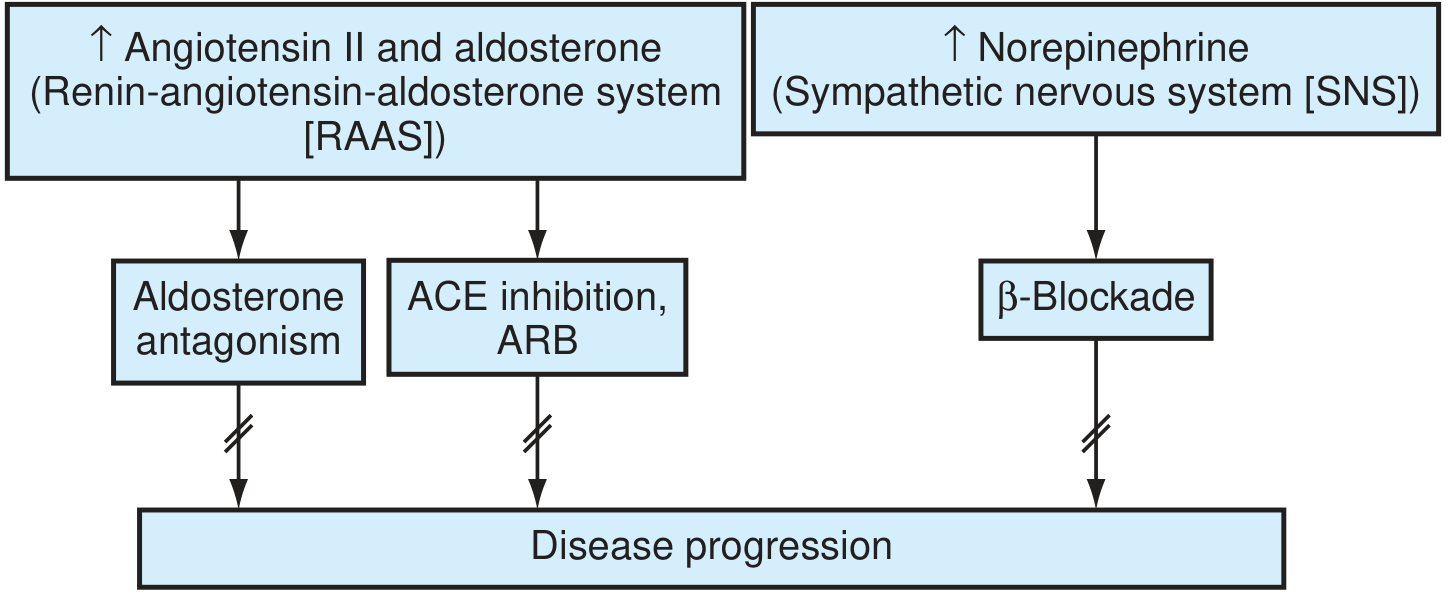
The renin-angiotensin-aldosterone and sympathetic nervous systems are key treatment targets in HF. (Textbook of Family Medicine 9e)
Frank-Starling Compensation
Early compensation increases preload → elevated end-diastolic volume → maintained stroke volume despite reduced EF. However, this raises pulmonary venous pressure, causing edema and eventually becoming maladaptive.
— Harrison's Principles of Internal Medicine 22E, p. 2021–2022; Textbook of Family Medicine 9e, p. 688–689; Sabiston Textbook of Surgery, p. 1120
Clinical Features
Symptoms
- Dyspnea: cardinal symptom of left HF — exertional dyspnea → orthopnea → paroxysmal nocturnal dyspnea (PND) → dyspnea at rest
- Orthopnea: dyspnea in the recumbent position, relieved by sitting up; occurs within 1–2 min of lying down
- PND: episodes that awaken patient from sleep; requires 30+ min upright for relief; may be accompanied by wheezing ("cardiac asthma")
- Bendopnea: dyspnea when bending forward — associated with elevated filling pressures
- Fatigue, reduced exercise tolerance
- Ankle and leg edema (right HF)
- Cheyne-Stokes respirations in advanced HF
Physical Examination Signs
- Elevated JVP (jugular venous pressure) — right atrial pressure estimate; hepatojugular reflux positive
- Pulmonary rales at lung bases (or throughout in severe HF)
- S3 gallop — implies volume overload and severe hemodynamic compromise; negative prognostic marker
- S4 gallop — seen in HFpEF with hypertension
- Displaced, diffuse apical impulse (dilated cardiomyopathy) or sustained (pressure overload)
- Bilateral pleural effusions (dullness to percussion at bases)
- Pulsus alternans — alternating strong/weak pulse due to incomplete ventricular recovery
- Holosystolic murmurs of mitral/tricuspid regurgitation in advanced HF
- Peripheral edema, hepatomegaly, ascites (right HF)
- Low-grade fever from cytokine activation in severe HF
— Harrison's Principles of Internal Medicine 22E, p. 2026–2028
Diagnosis
Key investigations include:
- ECG: arrhythmias, LVH, prior MI pattern
- Chest X-ray: cardiomegaly, pulmonary vascular congestion, pleural effusions
- Echocardiography: essential — measures EF, wall motion, diastolic function, valve disease, pericardial effusion
- BNP/NT-proBNP: biomarkers of myocardial wall stress; elevated in HF; useful for diagnosis and prognosis
- Laboratory: CBC (anemia), metabolic panel (renal function, electrolytes), thyroid function, LFTs
- Cardiac MRI: for cardiomyopathy characterization
- Coronary angiography: if ischemic etiology suspected
Management
Lifestyle Modifications
- Weight reduction, regular physical activity
- Sodium and fluid restriction
- Abstinence from alcohol, tobacco, and illicit drugs
- Optimization of comorbidities: diabetes, hypertension
Guideline-Directed Medical Therapy (GDMT) for HFrEF
Four pillars of evidence-based pharmacotherapy that reduce mortality:
| Drug Class | Examples | Mechanism |
|---|---|---|
| RAAS inhibitors ± neprilysin inhibitor | ACE inhibitors, ARBs, ARNI (sacubitril/valsartan) | Block angiotensin II/aldosterone harmful effects |
| Beta-blockers | Carvedilol, bisoprolol, metoprolol succinate | Block SNS toxicity, reduce remodeling |
| Mineralocorticoid receptor antagonists | Spironolactone, eplerenone | Block aldosterone-mediated fibrosis |
| SGLT2 inhibitors | Dapagliflozin, empagliflozin | Reduce HF hospitalizations and cardiovascular mortality |
Additional agents in select patients: hydralazine + nitrates (especially in Black patients), ivabradine (rate reduction), vericiguat (guanylate cyclase stimulator), diuretics (loop diuretics for congestion relief).
Device Therapy
- ICD (Implantable Cardioverter-Defibrillator): reduces sudden cardiac death in HFrEF with EF ≤35%
- CRT (Cardiac Resynchronization Therapy): biventricular pacing for patients with left bundle branch block and symptomatic HF — improves function and reduces mortality
- Transcatheter edge-to-edge repair (TEER): for secondary mitral regurgitation in advanced HF
Advanced/Refractory HF (ACC/AHA Stage D)
- LVAD (Left Ventricular Assist Device): durable mechanical circulatory support — used as bridge to transplant or destination therapy
- Heart transplantation: definitive therapy for eligible Stage D patients; improves survival and quality of life
- Absolute contraindication: pulmonary vascular resistance >6 Wood units
- Relative contraindications: PVR 4–6 Wood units, age >70, active malignancy, uncontrolled diabetes with end-organ damage
— Sabiston Textbook of Surgery, p. 1121; Textbook of Family Medicine 9e, p. 689; Harrison's Principles of Internal Medicine 22E
Prognosis
- 50% mortality within 5 years of diagnosis
- One-month readmission rate ~25%
- NYHA Class IV: 1-year mortality can exceed 50%
- Elevated BNP, low sodium, low EF, reduced peak VO₂, and elevated creatinine are adverse prognostic markers
- GDMT with all four drug pillars significantly reduces mortality and hospitalization
Sources: Harrison's Principles of Internal Medicine 22E | Textbook of Family Medicine 9e | Sabiston Textbook of Surgery | Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.