Mechanics of breathing 10/10 mark answer for final exam for PG pulmonary medicine
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed. Here is the comprehensive 10/10 PG pulmonary medicine exam answer:
Mechanics of Breathing
Introduction
The mechanics of breathing encompasses all the physical forces involved in moving air into and out of the lungs. Understanding it requires knowledge of the respiratory muscles, pressure relationships, elastic properties of the lung and chest wall, surface tension, surfactant, airway resistance, and the work of breathing. The diaphragm was recognized as the primary muscle of breathing as early as the time of Erasistratus; modern understanding began with Donders, Neergaard, and the discovery of surfactant between 1954-1960.
(Fishman's Pulmonary Diseases and Disorders, 2-Volume Set)
1. Respiratory Muscles
Muscles of Inspiration
The diaphragm is the most important muscle of inspiration. On contraction, it pushes the abdominal contents downward and lifts the ribs upward and outward, increasing intrathoracic volume. This decreases intrathoracic pressure, establishing the pressure gradient that drives air in. During exercise and increased ventilatory demand, the external intercostal muscles and accessory muscles (sternocleidomastoid, scalene, pectoral muscles) are recruited for augmented inspiration.
Muscles of Expiration
Normal quiet expiration is entirely passive - elastic recoil of the lungs and chest wall drives air out. No muscular energy is required. Active expiration occurs during exercise or in diseases with increased airway resistance (e.g., asthma, COPD). The muscles of active expiration are:
- Abdominal muscles (rectus abdominis, internal/external obliques, transversus) - compress the abdominal cavity and push the diaphragm up
- Internal intercostal muscles - pull the ribs downward and inward
(Costanzo Physiology 7th Edition)
2. Pressure Terminology and Relationships
All pressures in respiratory physiology are expressed relative to atmospheric pressure (zero reference) unless stated otherwise.
| Pressure Term | Definition |
|---|---|
| P_ao | Pressure at the airway opening (mouth) |
| P_A (P_alv) | Alveolar pressure |
| P_pl | Intrapleural (pleural) pressure |
| P_bs | Pressure at the body surface |
| Transpulmonary pressure (P_L) | P_A - P_pl = pressure across the lung |
| Transthoracic pressure | P_A - P_bs |
| Chest wall pressure | P_pl - P_bs |
At rest (FRC), no airflow:
- P_alv = 0 cmH₂O (equals atmospheric)
- P_pl = -5 cmH₂O (negative due to outward chest wall recoil vs. inward lung recoil)
- Transpulmonary pressure = +5 cmH₂O (keeps lungs expanded)
(Fishman's Pulmonary Diseases and Disorders)
3. The Breathing Cycle - Pressure and Volume Changes
The diagram below shows the interplay of lung volume, intrapleural pressure, and alveolar pressure during a normal breathing cycle:
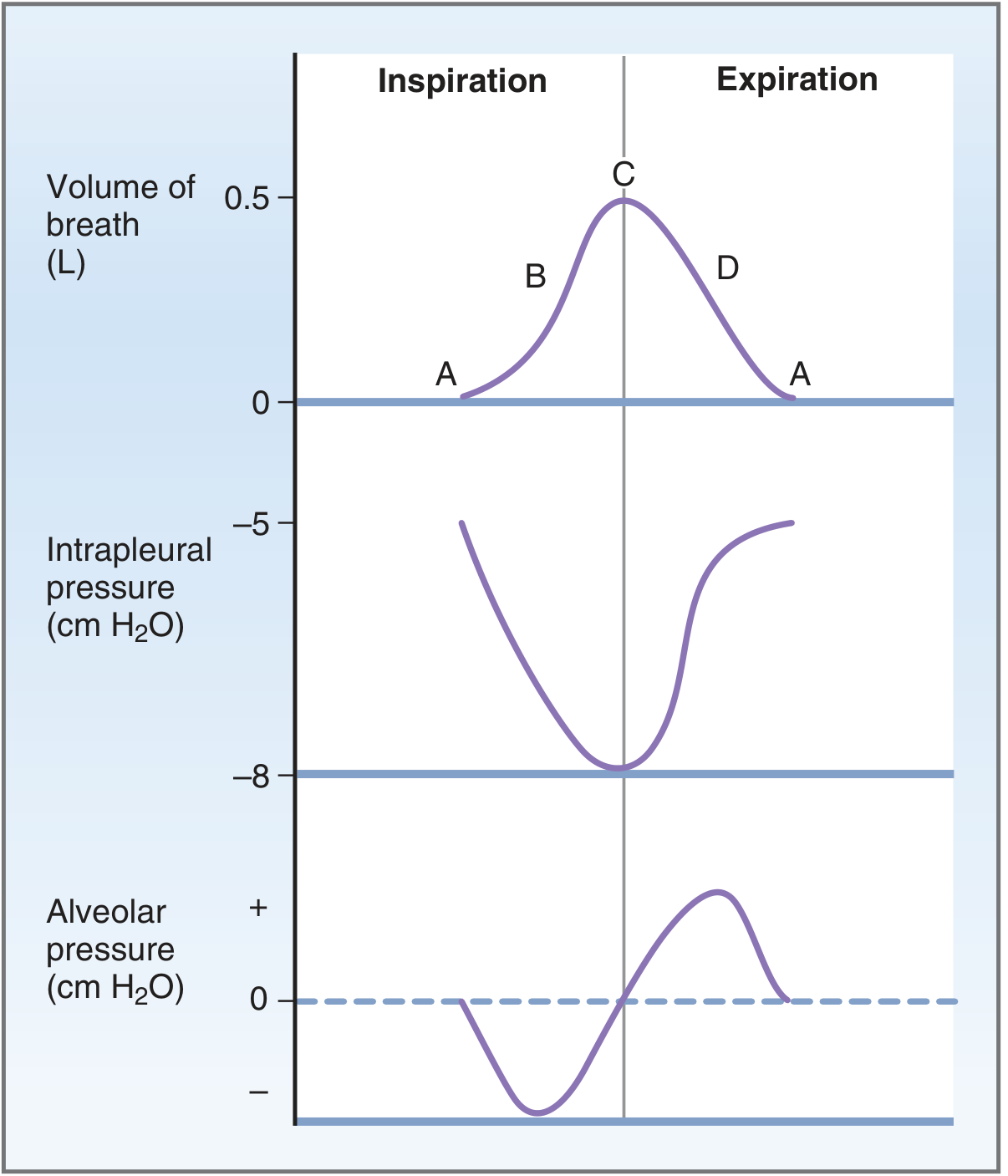
Fig: Volumes and pressures during the normal breathing cycle. Intrapleural pressure and alveolar pressure are referred to atmospheric pressure. (Costanzo Physiology)
Inspiration (Phases A→B→C):
- Diaphragm contracts → intrathoracic volume increases
- Lung volume increases by ~500 mL (tidal volume)
- P_pl falls from -5 to -8 cmH₂O (more negative)
- P_alv falls below atmospheric (becomes negative, ~-1 cmH₂O)
- Pressure gradient: atmosphere > alveolus → air flows INTO lungs
- At end-inspiration (point C): airflow ceases, P_alv returns to zero
Expiration (Phases C→D→A):
- Diaphragm relaxes → elastic recoil drives lung volume down
- P_pl returns toward -5 cmH₂O
- P_alv rises above atmospheric (becomes positive, ~+1 cmH₂O)
- Pressure gradient: alveolus > atmosphere → air flows OUT
- At end-expiration (point A): P_alv = 0, airflow ceases, FRC restored
4. Elastic Properties - Compliance
Compliance (C) is the change in volume per unit change in distending pressure. It is the inverse of elastance (stiffness).
$$C = \frac{\Delta V}{\Delta P}$$
Lung Compliance (C_L)
- Pressure applied = transpulmonary pressure (P_A - P_pl)
- Normal static lung compliance = 0.2 L/cmH₂O
- Measured as the slope of the static pressure-volume curve
Low compliance (stiff lung): pulmonary fibrosis, pulmonary edema, neonatal RDS - lungs resist expansion, more pressure needed per unit volume.
High compliance (floppy lung): emphysema - destruction of alveolar walls reduces elastic tissue.
Chest Wall Compliance (C_w)
- Pressure applied = transthoracic pressure (P_pl - P_bs)
- Normal = ~0.2 L/cmH₂O
- Reduced in: obesity, kyphoscoliosis, ankylosing spondylitis, circumferential burns
Total Respiratory System Compliance (C_RS)
Total compliance is less than either component alone:
$$\frac{1}{C_{RS}} = \frac{1}{C_L} + \frac{1}{C_W}$$
Normal C_RS = 0.1 L/cmH₂O
Static vs. Dynamic Compliance
- Static compliance (Cst): measured at points of zero airflow (true elastic property)
- Dynamic compliance (Cdyn): measured during breathing - includes resistive components. Normally ~80% of Cst. Frequency-dependence of dynamic compliance (Cdyn falls at high breathing frequencies) indicates small airway disease.
5. Elastic Recoil and Surface Tension
Determinants of Lung Elastic Recoil
Two components contribute to elastic recoil:
- Elastic tissue (collagen and elastin) in alveolar walls (~30% of total)
- Surface tension at the air-liquid interface lining alveoli (~70% of total)
Law of Laplace
$$P = \frac{2T}{r}$$
Where P = collapsing pressure, T = surface tension, r = alveolar radius.
This means:
- Large alveoli (large r) → LOW collapsing pressure → more stable
- Small alveoli (small r) → HIGH collapsing pressure → tend to collapse (atelectasis)
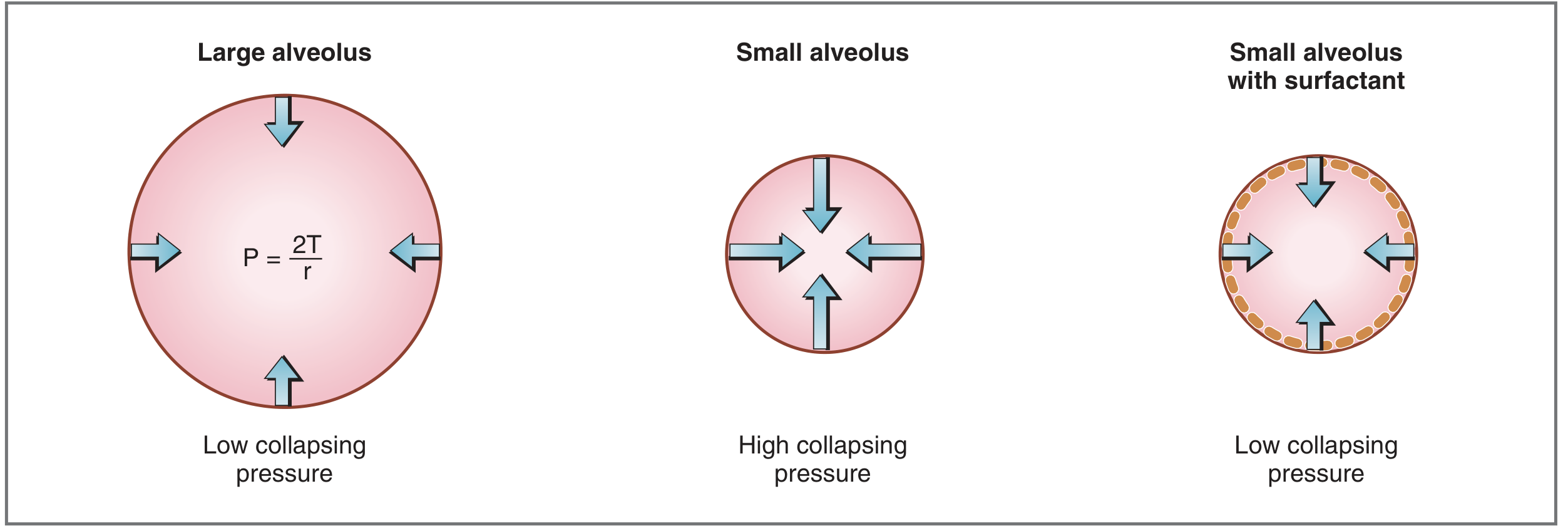
Fig: Effect of alveolar size and surfactant on collapsing pressure (Costanzo Physiology)
6. Surfactant
Surfactant is a mixture of phospholipids that lines the alveolar surface and reduces surface tension, thereby reducing the collapsing pressure and preventing alveolar collapse.
Composition
- Most important constituent: dipalmitoyl phosphatidylcholine (DPPC)
- Also contains phosphatidylglycerol, apoproteins (SP-A, SP-B, SP-C, SP-D)
Mechanism of Action
DPPC is amphipathic (hydrophobic + hydrophilic ends). Molecules align at the air-liquid interface with hydrophobic tails facing air, disrupting intermolecular cohesion of water molecules - this directly reduces surface tension.
Unique property: As alveoli shrink (expiration), surfactant molecules become more concentrated, further reducing surface tension proportionally to radius - this counteracts the Laplace effect and prevents small alveoli from collapsing and large alveoli from over-expanding (stabilizes alveoli of different sizes).
Functions of Surfactant
- Reduces surface tension → prevents alveolar collapse
- Increases lung compliance → reduces work of breathing
- Keeps alveoli dry (opposes transudation of fluid)
- Immunological role (SP-A, SP-D are collectins)
Synthesis
- By Type II pneumocytes (Type II alveolar cells)
- Synthesis begins at gestational week 24, reliably present by week 35
- Deficiency in premature infants → Neonatal Respiratory Distress Syndrome (NRDS / Hyaline Membrane Disease)
(Costanzo Physiology 7th Edition)
7. Airway Resistance
Airway resistance (R_aw) is the ratio of the pressure difference between alveoli and airway opening to airflow:
$$R_{aw} = \frac{P_A - P_{ao}}{\dot{V}} \quad \text{(normal: 0.5–2.0 cmH}_2\text{O/L/s)}$$
Normal R_aw at FRC = 1.5 cmH₂O/L/s; Normal airway conductance (G_aw = 1/R_aw) = 0.66 L/s/cmH₂O.
Poiseuille's Law (Laminar Flow)
$$R = \frac{8\eta l}{\pi r^4}$$
- Resistance is inversely proportional to the 4th power of radius - a small decrease in airway caliber causes a dramatic increase in resistance
- Applies to laminar (non-turbulent) flow in small airways
Laminar vs. Turbulent Flow
- Laminar flow: orderly, streamlined, governed by Poiseuille. Occurs in small airways.
- Turbulent flow: chaotic, occurs at high flow rates and in large airways. Described by the Reynolds number: $Re = \frac{2r \cdot v \cdot \rho}{\eta}$. Turbulence occurs when Re > 2000.
- Transitional flow at branching points
Distribution of Airway Resistance
- The large airways (trachea, main bronchi, upper airways) account for the majority (~80%) of total airway resistance
- Small airways (<2 mm diameter) are in parallel and contribute only ~20% of total R_aw - this is the "silent zone" where early disease may not be detected by standard spirometry
Factors Modifying Airway Resistance
| Factor | Effect on R_aw |
|---|---|
| Parasympathetic stimulation (cholinergic) | ↑ R_aw (bronchoconstriction) |
| Sympathetic stimulation (β₂ agonists) | ↓ R_aw (bronchodilation) |
| Increased lung volume | ↓ R_aw (radial traction/mechanical tethering opens bronchioles) |
| Decreased lung volume | ↑ R_aw (airways narrow; airway collapse at RV) |
| Increased gas viscosity (η) | ↑ R_aw |
| Helium breathing (low density) | ↓ R_aw (reduces turbulence) |
| Asthma/bronchospasm | ↑ R_aw |
Specific Conductance (sG_aw)
$sG_{aw} = G_{aw}/V_L$ - corrects airway conductance for lung volume. Normal = 0.22 /cmH₂O/s.
8. Dynamic Airway Compression and Effort Independence
During forced expiration, pleural pressure becomes positive. Beyond a critical point in the airways (the Equal Pressure Point, EPP), intraluminal pressure equals pleural pressure - downstream to this point, airways are compressed.
- Airways upstream (alveolar side) of EPP: R_us - upstream resistance
- Airways downstream (mouth side) of EPP: R_ds - downstream resistance; these airways collapse during forced expiration
Clinical significance: The maximal expiratory flow at any lung volume below 75% of TLC is effort-independent - determined entirely by upstream airway resistance, lung recoil pressure, and lung volume, NOT by expiratory muscle force. This explains the flow-volume curve plateau and why COPD patients cannot increase flow by more forceful effort.
In emphysema: loss of elastic recoil → EPP shifts upstream (toward smaller airways) → dynamic compression occurs at higher lung volumes → air trapping and hyperinflation.
9. Work of Breathing (WOB)
Work = Force × Distance = Pressure × Volume. WOB can be broken into three components:
Components of WOB
- Elastic work (~65%): Overcome elastic recoil of lungs and chest wall during inspiration. Stored as potential energy, released during passive expiration.
- Resistive work (~30%): Overcome frictional (viscous) resistance of airflow in airways.
- Inertial work (<5%): Accelerate gas and tissue mass - negligible at normal breathing rates.
Normal WOB
- ~0.5 J/breath at rest
- O₂ cost of breathing: ~1-3% of total body VO₂ at rest
- Relationship between ventilation and respiratory muscle O₂ consumption is curvilinear - O₂ cost increases dramatically at high minute ventilation
Pathological WOB
- Restrictive disease (e.g., fibrosis, pulmonary edema): elastic work greatly increased. Patients adopt rapid, shallow breathing (minimizes elastic work).
- Obstructive disease (e.g., COPD, asthma): resistive work predominates. Patients adopt slow, deep breathing (minimizes resistive work).
- In severe COPD, respiratory muscle O₂ demand during high ventilatory effort may outstrip O₂ delivery → anaerobic metabolism → lactic acidosis
Optimal Breathing Pattern
The respiratory control system automatically adjusts frequency and tidal volume to minimize total WOB - this is the physiological basis for different breathing patterns in different diseases.
(Fishman's Pulmonary Diseases and Disorders)
10. Functional Residual Capacity and the Relaxation Pressure Curve
FRC is the volume at which the inward elastic recoil of the lungs exactly equals the outward elastic recoil of the chest wall - the resting equilibrium of the respiratory system with no muscular activity.
- At FRC: P_pl = -5 cmH₂O; respiratory muscles are relaxed
- Above FRC: lungs recoil inward more than chest walls recoil outward → net force to deflate
- Below FRC: chest walls dominate → net force to inflate
The Campbell diagram (pressure-volume diagram with both lung and chest wall curves) is used to partition WOB into elastic (lung) and resistive components, and is used to estimate inspiratory muscle effort.
11. Key Normal Values (Fishman's Reference)
| Parameter | Normal Value |
|---|---|
| Static lung compliance (Cst,L) | 0.2 L/cmH₂O |
| Respiratory system compliance (CRS) | 0.1 L/cmH₂O |
| Airway resistance at FRC (R_aw) | 1.5 cmH₂O/L/s |
| Total pulmonary resistance at FRC | 2.0 cmH₂O/L/s |
| Airway conductance (G_aw) | 0.66 L/s/cmH₂O |
| Specific conductance (sG_aw) | 0.22 /cmH₂O/s |
| Maximum inspiratory pressure | -75 mmHg |
| Maximum expiratory pressure | +120 mmHg |
(Fishman's Pulmonary Diseases and Disorders, Appendix B)
12. Clinical Correlations for PG Pulmonary
| Condition | Compliance | R_aw | Dominant WOB | Breathing Pattern |
|---|---|---|---|---|
| Pulmonary fibrosis | ↓↓ (stiff) | Normal/↑ | Elastic | Rapid, shallow |
| Emphysema | ↑↑ (floppy) | ↑ (loss of tethering) | Resistive | Slow, deep; pursed-lip |
| Asthma | Normal | ↑↑ | Resistive | Slow, deep; high lung volumes |
| Pulmonary edema | ↓ | ↑ (fluid) | Elastic | Rapid, shallow |
| Obesity | Normal (lung) / ↓ (chest) | Normal-↑ | Elastic (chest) | Rapid, shallow |
| NRDS (premature) | ↓↓ | Normal | Elastic | Gasping; intercostal recession |
Summary
The mechanics of breathing is determined by the interplay of:
- Respiratory muscles (diaphragm primary for inspiration; passive expiration at rest)
- Pressure gradients (alveolar-atmospheric) driven by thoracic volume changes
- Lung compliance (elastic tissue + surface tension; reduced by surfactant/DPPC)
- Airway resistance (4th-power radius relationship; modulated by autonomic tone, lung volume, flow regime)
- Work of breathing (elastic + resistive + inertial; minimized by automatic adjustment of breathing pattern)
Understanding these principles explains the pathophysiology of obstructive vs. restrictive lung disease, the basis of pulmonary function tests, the rationale for bronchodilator therapy, and the oxygen cost of breathing in critically ill patients.
Sources: Fishman's Pulmonary Diseases and Disorders (2-Volume Set); Costanzo Physiology 7th Edition
This is a shared conversation. Sign in to Orris to start your own chat.