Anal fistula
Reading File
Finding Sources
Searching Images
anal fistula classification Parks diagram
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of anal fistula:
Anal Fistula (Fistula-in-Ano)
Definition & Epidemiology
An anal fistula represents the chronic form of a perianal abscess — a tract from an infected anal gland that fails to heal after the abscess drains. It occurs in 30–50% of patients following a perianal abscess. Incidence is approximately 8.6 per 100,000, and fistulae are 2–3× more common in men than women.
Pathogenesis
The cryptoglandular theory is the basis: anal glands drain into the crypts at the dentate line. When these glands become infected, an intersphincteric abscess forms and spreads through the surrounding spaces. After drainage — surgical or spontaneous — the internal opening at the dentate line may remain patent, creating a persistent tract.
Parks Classification
The most widely used classification is based on the tract's relationship to the anal sphincter complex:
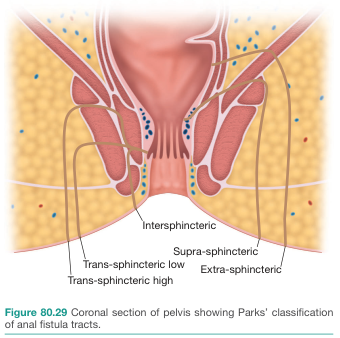
| Type | Frequency | Description |
|---|---|---|
| Intersphincteric | ~70% | Runs between internal and external sphincter; most common |
| Transsphincteric | ~20–25% | Traverses both sphincters; "low" (distal EAS) or "high" (proximal EAS) |
| Suprasphincteric | Rare | Arises at dentate line, loops over entire sphincter complex before descending |
| Extrasphincteric | Rare | Internal opening remote from dentate line; bypasses sphincter entirely; often from pelvic abscess (diverticulitis, Crohn, ruptured appendix) |
A horseshoe fistula has external openings on both sides of the midsagittal plane, typically with a single internal opening in the posterior midline.
Goodsell's Rule
A useful clinical guide for predicting internal opening location:
- External opening posterior to a transverse line across the anus → internal opening in the posterior midline
- External opening anterior → internal opening at the nearest crypt
Clinical Features
- Recurrent perianal abscess in the same location
- Persistent or intermittent purulent discharge from perianal skin
- Perianal nodule or induration
- External opening with granulation tissue (may intermittently close over)
- Patients often describe cycles of a "boil" forming, rupturing spontaneously, and relieving pain — then recurring
Key differentials: Hidradenitis suppurativa (superficial tracts, no anal canal involvement), pilonidal disease (gluteal cleft, hair-related foreign body reaction)
Evaluation
History: Duration, prior anorectal surgery, sphincter function, urogenital symptoms, bowel changes (Crohn disease suspicion)
Examination: Visualize external opening; palpate fibrous tract; anoscopy may reveal internal opening at dentate line
Investigations:
- MRI (modality of choice): Fat-suppressed T2W sequences show fistula tracts as high signal against sphincter complex; identifies supralevator extensions and abscesses; preoperative MRI reduces recurrence in complex fistula
- Endoanal ultrasound: Delineates tract and internal opening well
- Hydrogen peroxide injection into external opening (with or without EAUS): helps identify smaller fistulas
- CT/fistulography (water-soluble contrast + fluoroscopy): complex or multiple tracts
Multiple or atypical fistulae should always raise suspicion for Crohn disease.
Management
Treatment is surgical. The goal is elimination of the internal opening and eradication of the tract.
Principles
- Identify the full length of the tract (examination under anesthesia)
- Assess the proportion of sphincter involved
- Choose procedure based on fistula complexity and continence risk
Fistulotomy (laying open)
- First-line for simple fistulae (intersphincteric, low transsphincteric)
- Unroofing the tract allows healing by secondary intention
- Safe when <30% of sphincter is involved and baseline continence is normal
- Healing rates up to 90%
- Caution: Anterior fistulotomy in women (short anterior sphincter, risk of obstetric injury)
Seton
- Used for high or complex fistulae involving >30% of sphincter
- A suture or Silastic vessel loop passed through the tract and tied to itself
- Cutting seton — gradually tightened to divide muscle slowly (less incontinence risk)
- Draining seton — maintains drainage, prevents abscess recurrence; allows tract to mature before definitive repair
- After several weeks, the tract scars, allowing a subsequent sphincter-sparing procedure
Sphincter-sparing options (complex/high fistulae)
- Advancement flap — mucosal or full-thickness flap used to close the internal opening
- Fistula plug (bioprosthetic)
- LIFT procedure (ligation of intersphincteric fistula tract)
- Fibrin glue — lower success but minimal continence risk
- Anti-TNF therapy (infliximab, adalimumab) for Crohn disease–associated fistulae
Fistula and Crohn Disease
Complex, multiple, or recurrent fistulae mandate evaluation for Crohn disease. Crohn perianal fistulae are treated with a combination of medical (immunosuppression, biologics) and surgical (drainage seton, abscess control) approaches, prioritizing continence preservation over cure.
Sources: Mulholland and Greenfield's Surgery 7e, p. 3558–3562 | Goldman-Cecil Medicine | Grainger & Allison's Diagnostic Radiology | Bailey and Love's Short Practice of Surgery, p. 1457
This is a shared conversation. Sign in to Orris to start your own chat.