Left anterior fascicular block note
Reading File
Finding Sources
Finding Sources
Searching the Web
left anterior fascicular block ECG criteria clinical significance
Reading File
Reading File
Searching Images
left anterior fascicular block ECG
Reading File
Reading File
Loading Image
Here is a comprehensive clinical note on Left Anterior Fascicular Block (LAFB):
Left Anterior Fascicular Block (LAFB)
Anatomy & Mechanism
The left bundle branch divides into two fascicles:
- Anterior fascicle — thin, long, supplied mainly by the LAD; innervates the anterolateral LV wall
- Posterior fascicle — short, thick, dual blood supply (LAD + RCA); innervates the inferoseptal LV wall
When the anterior fascicle is blocked, ventricular activation proceeds via the posterior fascicle → initial depolarization is inferior and rightward, then forces swing superior and leftward, producing marked left axis deviation without significant QRS widening. — Harrison's Principles of Internal Medicine 22E
ECG Diagnostic Criteria
| Criterion | Finding |
|---|---|
| QRS duration | < 120 ms (no major widening) |
| Frontal axis | More negative than −45° (typically −45° to −90°) |
| Lead I / aVL | qR pattern (small q, tall R) |
| Leads II, III, aVF | rS pattern (small r, deep S) |
| R-wave peak time in aVL | > 45 ms (prolonged) |
| Precordial leads | Normal (no significant change) |
LAFB is the most common cause of marked left axis deviation in adults. — Harrison's 22E, p. 1915
The LITFL ECG criteria additionally note that the R-wave amplitude in aVL may meet LVH voltage criteria (R > 11 mm) without an LV strain pattern — an important distinguishing point.
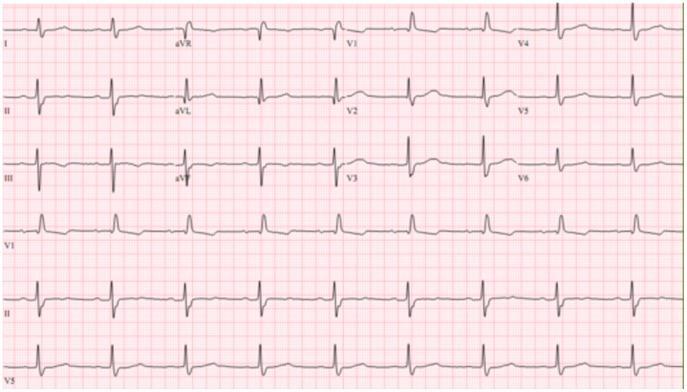
ECG Example
Below is a 12-lead ECG demonstrating RBBB + LAFB (bifascicular block), illustrating the characteristic left axis deviation with rS in the inferior leads and RBBB morphology in V1–V3:
Epidemiology
- Found in approximately 1% of otherwise healthy adults — Goldman-Cecil Medicine, p. 565
- Prevalence of any bundle branch block increases from ~1% at age 50 to ~17% by age 80
- Left posterior fascicular block is far rarer and almost always occurs with RBBB
Etiology / Associated Conditions
| Category | Examples |
|---|---|
| Degenerative | Lev's/Lenègre's disease (fibrosis of conduction system) |
| Ischemic | Coronary artery disease (LAD territory) |
| Structural | Cardiomyopathy, aortic valve disease |
| Infiltrative | Sarcoidosis, amyloidosis |
| Acute | Anterior MI (new LAFB is significant) |
| Idiopathic | Isolated LAFB in healthy adults (most common) |
Clinical Significance
- Isolated LAFB: generally asymptomatic and carries a benign prognosis in the absence of structural heart disease
- New LAFB in the setting of anterior MI: suggests proximal LAD occlusion with involvement of the septal perforators → clinically significant marker
- LAFB + RBBB = Bifascicular block: indicates disease of 2 of 3 fascicles; risk for complete heart block, especially if PR interval is also prolonged (trifascicular block)
- Bifascicular block + syncope: pacemaker implantation is preferred over monitoring, regardless of block morphology or PR interval — Goldman-Cecil Medicine, p. 566
- Bifascicular block + new PR prolongation in acute MI: prophylactic pacemaker often placed due to high risk of progression to complete heart block
Differentiation from Other Causes of Left Axis Deviation
LAFB must be distinguished from:
- Inferior MI — pathologic Q waves in II, III, aVF (vs. small r waves in LAFB)
- LVH — LVH axis rarely exceeds −30° to −45°; strain pattern present
- WPW (inferior accessory pathway) — delta waves, short PR
- Hyperkalemia / Class I antiarrhythmic toxicity — diffuse QRS widening
Management
- No treatment needed for isolated, asymptomatic LAFB
- Evaluate for underlying cause: echocardiography ± stress test; cardiac MRI if infiltrative cardiomyopathy suspected
- Rhythm monitoring if associated with PR prolongation, alternating blocks, or symptoms (presyncope/syncope)
- Pacemaker if: bifascicular block + syncope, or new bifascicular block + PR prolongation in acute MI setting — Goldman-Cecil Medicine
Summary
LAFB = QRS axis −45° to −90° + qR in I/aVL + rS in II/III/aVF + QRS < 120 ms. Isolated LAFB is common and benign; its significance lies in identifying underlying coronary/structural disease and its role in bifascicular/trifascicular block progression.
Sources: Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine (International Edition); LITFL ECG Library
This is a shared conversation. Sign in to Orris to start your own chat.