Compare ESC and AHA guidelines on heart failure management and generate an image
Reading File
Finding Sources
Finding Sources
Generating Image
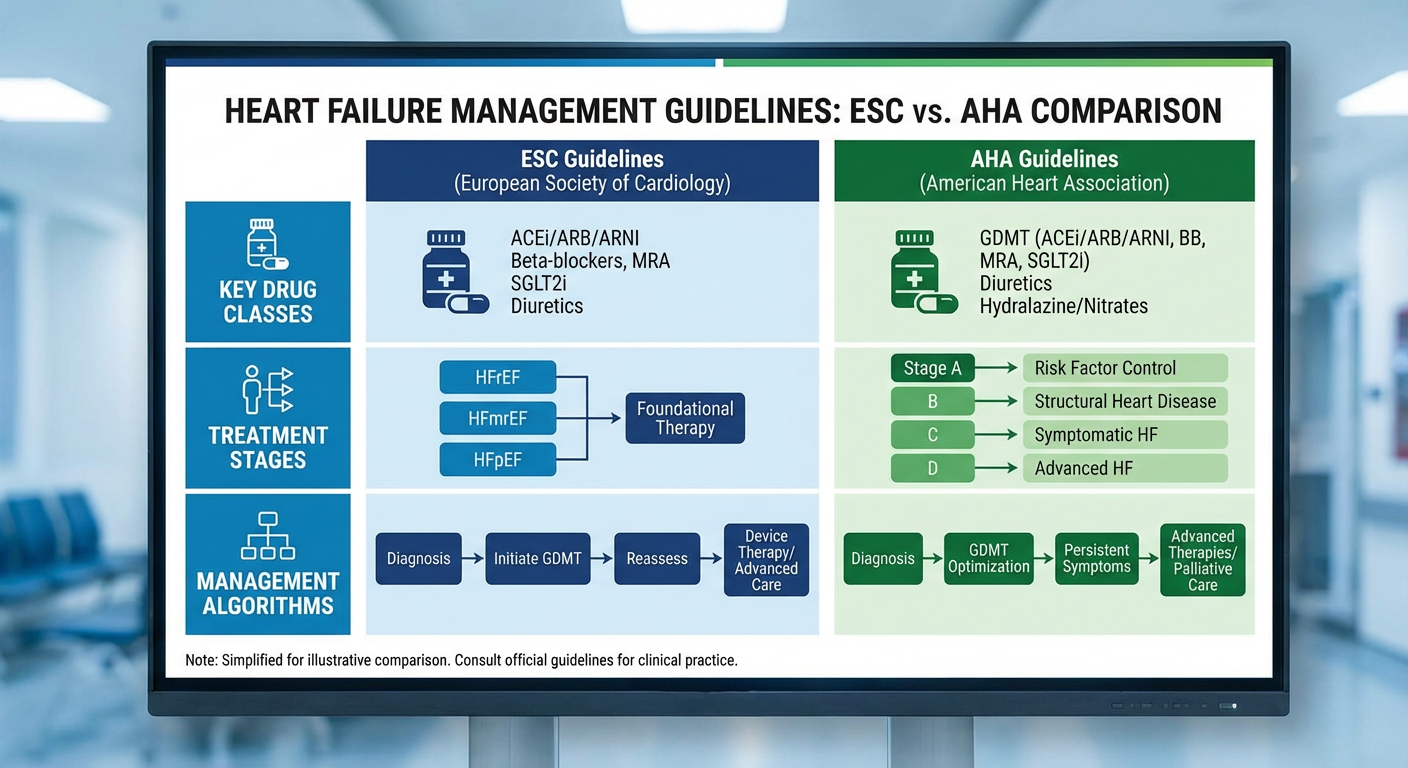
A professional medical comparison infographic of ESC vs AHA heart failure management guidelines, showing two columns with key drug classes, treatment stages, and management algorithms side by side
Reading File
Reading File
Reading File
I now have excellent comparative content. Let me compile the full comparison.
ESC vs AHA Guidelines on Heart Failure Management
Here is the generated infographic:
Overview
Both the ACC/AHA (2013, updated 2017) and ESC (2016) guidelines provide comprehensive frameworks for heart failure (HF) management, but differ meaningfully in several areas due to differing evidence weighting and publication timing.
Key Differences: ESC vs ACC/AHA
| Domain | ACC/AHA | ESC |
|---|---|---|
| ARNI (Sacubitril/Valsartan) | Class Ia — Switch all HFrEF patients with NYHA II/III from ACE-i/ARB to ARNI | Conditional — Only for persistent symptoms despite full triple neurohormonal blockade |
| CRT with intermediate QRS (130–149 ms) + LBBB | Class IIb recommendation | Class I recommendation |
| Hydralazine-nitrate (African American patients) | Class Ia for NYHA III/IV despite optimal therapy | Class IIa recommendation |
| Natriuretic peptides (BNP/NT-proBNP) for prognosis | Class I recommendation | Class IIa recommendation |
| Predischarge natriuretic peptide measurement | Class IIa recommendation | No specific recommendation |
| Biomarkers of fibrosis (ST2, galectin-3) | Class IIb — may be considered | Not addressed |
| Cardiac MRI | Class IIa — for myocardial scar or infiltration assessment | Class Ia — strongly advocated for tissue characterization (myocarditis, amyloid), and to distinguish ischemic vs non-ischemic etiology |
Areas of Agreement
Both guidelines share strong concordance on:
- ACE inhibitors / ARBs — foundational therapy in HFrEF (Class I)
- Beta-blockers — carvedilol, bisoprolol, metoprolol succinate; initiated within 24h in STEMI without contraindications and continued long-term
- Mineralocorticoid receptor antagonists (MRA) — spironolactone/eplerenone in symptomatic HFrEF with LVEF ≤35%
- Diuretics — for congestion relief
- ICD therapy — for sudden cardiac death prevention in LVEF ≤35%
- CRT — Class I in NYHA II–IV, LVEF ≤35%, QRS ≥150 ms with LBBB morphology
- Device therapy — ICD + CRT-D in eligible patients
- SGLT2 inhibitors — added in later updates (2021/2022 focused updates for both)
Notable Pharmacotherapy Comparison
| Drug Class | ACC/AHA | ESC |
|---|---|---|
| ACE inhibitor | Class I, all HFrEF | Class I, all HFrEF |
| ARB | Class I if ACE-i intolerant | Class I if ACE-i intolerant |
| ARNI | Class I, replace ACE-i/ARB in NYHA II/III | Class I, but after triple therapy failure |
| Beta-blocker | Class I | Class I |
| MRA | Class I, LVEF ≤35% | Class I, LVEF ≤35% |
| Hydralazine-nitrate | Class Ia (African Americans), IIa others | Class IIa (African Americans) |
| Ivabradine | Class IIa (HR ≥70, sinus rhythm on max beta-blocker) | Class IIa |
| Digoxin | Class IIb | Class IIb |
Clinical Takeaway
The main practical divergence is around ARNI positioning and CRT indications for intermediate QRS. ACC/AHA takes a more aggressive stance on ARNI as a first-line replacement, while ESC reserves it for refractory cases. ESC places greater emphasis on cardiac MRI for diagnostic characterization. ACC/AHA gives stronger recommendations for novel biomarkers (ST2, galectin-3) and natriuretic peptide monitoring.
— Fuster and Hurst's The Heart, 15th Edition, Table 48-17 and pp. 1549–1551
This is a shared conversation. Sign in to Orris to start your own chat.