Retinal detachment
Reading File
Finding Sources
Searching Images
retinal detachment fundoscopy clinical image
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Here is a comprehensive overview of retinal detachment drawn from authoritative ophthalmology and medical references.
Retinal Detachment
Definition
A retinal detachment (RD) is a separation of the neurosensory retina from the underlying retinal pigment epithelium (RPE). — Goldman-Cecil Medicine
Types
1. Rhegmatogenous RD (RRD) — Most Common
- Caused by a retinal break (tear or hole) that allows liquefied vitreous to seep under the neurosensory retina
- Nearly always requires concurrent vitreous liquefaction and traction — a break alone rarely causes detachment
- Affects ~1 in 10,000 per year; both eyes eventually affected in ~10% of patients
- Over 40% occur in myopic eyes — higher myopia = greater risk
- Also associated with posterior vitreous detachment (PVD), lattice degeneration, snail-track degeneration, prior cataract surgery, and laser capsulotomy
2. Tractional RD
- Caused by fibrocellular bands in the vitreous contracting and pulling the retina off
- Causes: proliferative diabetic retinopathy (most common), sickle cell retinopathy, retinopathy of prematurity, toxocariasis, trauma, proliferative vitreoretinopathy (PVR)
- Retina appears concave with a smooth surface; detachment rarely reaches the ora serrata; retina is immobile
3. Exudative (Serous) RD
- No break or traction — fluid accumulates under the retina due to breakdown of the blood-retinal barrier
- Causes: malignant hypertension, eclampsia of pregnancy, choroidal tumors, posterior scleritis, uveal effusion syndrome
- Generally resolves when the underlying cause is treated — no direct surgical intervention needed
Symptoms (RRD)
Classic premonitory symptoms (in ~60% of cases):
- Photopsia (flashing lights) — due to vitreoretinal traction from PVD
- Floaters — due to the causative vitreous detachment
- Curtain-like visual field defect — peripheral, progressing centrally; the quadrant of the field defect is in the opposite quadrant to the primary break
- Some patients note the field defect improves on waking (due to overnight SRF reabsorption) and worsens during the day
- Loss of central vision if the macula (fovea) becomes involved
Tractional RD may be asymptomatic or cause gradual visual field loss/visual decline.
Break Localization (Lincoff's Rules)
Distribution of breaks in eyes with RRD:
- 60% superotemporal
- 15% superonasal
- 15% inferotemporal
- 10% inferonasal
Subretinal fluid (SRF) spread can predict break location:
- Superior break → SRF first spreads inferiorly ipsilateral, then rises on opposite side
- 6 o'clock break → equal inferior fluid levels
- Bullous inferior RD → primary break usually above the horizontal meridian
- Superior nasal break → SRF revolves around the optic disc and rises on temporal side
Fundoscopic Appearance
Fresh RRD: Convex configuration, slightly opaque and corrugated (due to retinal edema), loss of underlying choroidal pattern
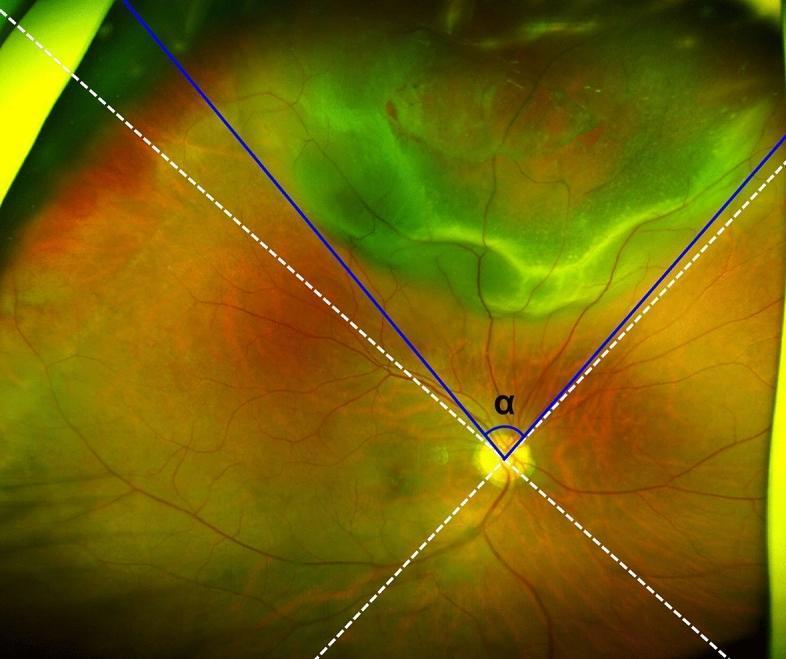
Wide-field fundus image of a rhegmatogenous retinal detachment — elevated, bullous, pale-green area in the superior quadrant. White dashed lines divide the fundus into quadrants; blue lines measure angular extent (α) from the optic disc for surgical planning.
Workup
- Dilated fundoscopy with indirect ophthalmoscopy + scleral depression of both eyes — identify all breaks
- Slit lamp with 90D or widefield lens — assess vitreous, peripheral retina
- B-scan ultrasound — if media opacity prevents fundus visualization (e.g., dense vitreous hemorrhage)
- OCT — useful in tractional RD to identify membranes and differentiate from other pathology
Differential Diagnosis
| Condition | Key Differentiating Feature |
|---|---|
| Retinoschisis | Bilateral, smooth, bullous, inferotemporal; no pigment cells in vitreous |
| Choroidal detachment | Brown, smooth, extends beyond ora serrata; limited posteriorly by vortex veins; low IOP |
| Uveal effusion syndrome | Idiopathic, bilateral; "leopard spot" RPE mottling after resolution |
Treatment
Urgency
- Macula-on RRD: Surgical emergency — repair as soon as possible; macula must be protected
- Macula-off RRD: Urgent but not emergent — visual outcomes comparable if surgery done within 7–10 days of onset
- Dense vitreous hemorrhage + RD on B-scan: Operate urgently
- Tractional RD: May observe if not threatening the macula; vitrectomy when indicated
- Exudative RD: Treat the underlying cause — usually no direct surgical intervention
Surgical Options
| Procedure | Description | Indications |
|---|---|---|
| Pneumatic retinopexy | Intravitreal gas bubble (SF6 or C3F8) + cryotherapy/laser to seal break; office-based | Uncomplicated RRD, single small break or cluster <2 clock hours, in upper 2/3 of retina |
| Scleral buckling | Silicone explant sutured to sclera creates inward indentation to close break and reduce traction | Preferred for post-traumatic dialysis; peripheral breaks; young patients |
| Pars plana vitrectomy (PPV) | Removal of vitreous, membrane peeling, fluid-gas exchange, laser/cryotherapy, tamponade | Complex RD, PVR, tractional RD, posterior breaks, failed prior repair |
Pre-op: Patient should fast if urgent surgery is planned; bed rest with head positioning so the break is most dependent reduces SRF.
TIP: Even if the macula is already off, surgery within 72 hours gives better visual results. — Kanski's Clinical Ophthalmology
Follow-Up
- Post-RRD repair: 1 day → 1 week → 1 month → 2–3 months → every 6–12 months
- Fellow eye must always be examined given ~10% bilateral risk
Sources: Kanski's Clinical Ophthalmology (10th ed.), The Wills Eye Manual, Goldman-Cecil Medicine, Robbins Pathology
Give retinal detachment for 10 marks
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
retinal detachment types rhegmatogenous tractional exudative diagram
Here is a structured, 10-mark postgraduate ophthalmology answer on retinal detachment.
Retinal Detachment — 10 Mark Answer
Definition
Retinal detachment (RD) is a separation of the neurosensory retina from the underlying retinal pigment epithelium (RPE), with accumulation of subretinal fluid (SRF) in the potential subretinal space.
Classification
1. Rhegmatogenous RD (RRD) — Most Common
A retinal break (tear or hole) allows liquefied vitreous to pass into the subretinal space. Requires two concurrent conditions: a break and at least partial vitreous liquefaction with traction.
Risk factors:
- High myopia (>40% of all RRDs)
- Posterior vitreous detachment (PVD)
- Predisposing lesions: lattice degeneration, snail-track degeneration, atrophic round holes
- Aphakia/pseudophakia, vitreous loss at cataract surgery, laser capsulotomy
- Trauma (dialysis at ora serrata)
- Family history; fellow eye at ~10% risk
2. Tractional RD
Fibrocellular proliferative membranes contract and physically pull the retina off the RPE. No retinal break is present (unless combined TRD-RRD).
Causes: Proliferative diabetic retinopathy (most common), sickle cell retinopathy, retinopathy of prematurity, penetrating trauma, toxocariasis, proliferative vitreoretinopathy (PVR)
3. Exudative (Serous) RD
Breakdown of the blood-retinal barrier causes fluid accumulation under the retina without a break or traction.
Causes: Malignant hypertension, eclampsia of pregnancy, VKH disease, posterior scleritis, choroidal tumors, uveal effusion syndrome
Symptoms (RRD)
In ~60% of patients, classic premonitory symptoms accompany acute PVD:
- Photopsia — flashing lights from vitreoretinal traction
- Floaters — pigment cells or vitreous debris (including "tobacco dust" = Shafer's sign)
- Curtain-like visual field defect — appears in the opposite quadrant to the primary break
- Decreased central vision — if the macula (fovea) is involved
The quadrant of the field defect corresponds to the opposite quadrant of the primary break. Photopsia location does not predict break location.
Signs
Anterior segment:
- Mild iritis (common); severe iritis suggests Schwartz-Matsuo syndrome
- Reduced IOP (~5 mmHg lower than fellow eye); extremely low IOP suggests associated choroidal detachment
- Relative afferent pupillary defect (RAPD) in extensive RD
- Tobacco dust (Shafer's sign) — pigment cells in anterior vitreous; highly specific for RRD
Fundus — RRD:
- Fresh RD: Convex, corrugated, opaque appearance (retinal edema); elevated with loss of choroidal pattern
- Longstanding RD: Retinal atrophy, intraretinal cysts (after ~1 year), subretinal demarcation lines/pigment "tide marks" (after ~3 months)
- Breaks: Red discontinuities in the retinal surface (colour contrast with choroid); may be less visible in high myopia
Fundus — Tractional RD: Concave, smooth, immobile retina; does not extend to ora serrata; vitreous/epiretinal membranes visible
Break Localization — Modified Lincoff's Rules
| Configuration of SRF | Likely location of primary break |
|---|---|
| Shallow inferior RD, higher on temporal side | Inferior temporal |
| Equal inferior fluid levels | 6 o'clock |
| Bullous inferior RD | Above horizontal meridian |
| SRF crosses vertical midline above | Near 12 o'clock |
| Superior nasal break | SRF revolves around disc, rises temporally |
Break distribution: 60% superotemporal · 15% superonasal · 15% inferotemporal · 10% inferonasal. ~50% of RRDs have more than one break, often within 90° of each other.
Investigations
- Indirect ophthalmoscopy with scleral depression — both eyes; essential to identify all breaks
- Slit lamp + 90D/widefield lens — vitreous assessment, tobacco dust, posterior breaks
- B-scan ultrasound — when fundal view is obscured (dense vitreous haemorrhage, media opacity)
- OCT — useful in tractional membranes, macular status, sub-foveal fluid, and differentiating retinoschisis from RD
Differential Diagnosis
| Condition | Key Feature |
|---|---|
| Retinoschisis | Bilateral, smooth, bullous, inferotemporal; no pigment in vitreous; inner/outer layer holes |
| Choroidal detachment | Brown, extends beyond ora serrata, limited posteriorly by vortex veins; low IOP; no vitreous pigment |
| Uveal effusion syndrome | Idiopathic; "leopard spot" RPE mottling after resolution |
Treatment
Urgency
- Macula-on RRD — surgical emergency; operate as soon as possible
- Macula-off RRD — visual outcome does not significantly change if surgery within 7–10 days of onset
- Dense vitreous haemorrhage + RD on B-scan — urgent surgery
- Exudative RD — treat the underlying cause; direct surgery not usually needed
Surgical Options
1. Pneumatic Retinopexy
- Intravitreal gas bubble (SF₆ or C₃F₈) + cryotherapy or laser
- Office-based, minimally invasive
- Indication: Single small break or cluster <2 clock hours in the upper 2/3 of peripheral retina; uncomplicated RRD
- Limitation: Lower success rate than scleral buckling
2. Scleral Buckling (External Surgery)
- Silicone explant sutured to sclera creates an inward indentation to close the break and reduce vitreoretinal traction
- Configurations: radial, segmental, circumferential, or encircling
- Procedure: Peritomy → break localization → cryotherapy → explant sutured → subretinal fluid drainage if needed
- Indication: Peripheral breaks, post-traumatic dialysis, young phakic patients
- Complications: Diplopia, CME (~25%), epiretinal membrane (~15%), anterior segment ischaemia, buckle extrusion/infection, elevated IOP, choroidal detachment
3. Pars Plana Vitrectomy (PPV) — Internal Surgery
- 3-port approach (infusion + vitreous cutter + light probe via sclerotomies)
- Steps: Core vitrectomy → posterior hyaloid separation → membrane peeling → fluid-air/gas exchange → laser/cryopexy → tamponade
- Tamponade agents: Expanding gas (SF₆, C₃F₈) or silicone oil (for complex cases, PVR, inferior breaks)
- Indications: Posterior/giant breaks, PVR (Grade B or C), tractional RD, haemorrhage obscuring breaks, pseudophakic RD, failed scleral buckle
- For PVR: Membrane peeling ± ILM peeling ± relaxing retinotomy + long-acting tamponade
Proliferative Vitreoretinopathy (PVR) — Major Complication
Epiretinal and subretinal membrane formation causing fixed retinal folds and traction; occurs after surgery or penetrating injury.
| Grade | Features |
|---|---|
| A (minimal) | Diffuse vitreous haze, tobacco dust, pigment clumps inferior retina |
| B (moderate) | Inner surface wrinkling, rolled break edges, retinal stiffness, vascular tortuosity |
| C (marked) | Rigid full-thickness folds (star-shaped), funnel RD in advanced disease |
Management: PPV + membrane peeling ± ILM peeling ± relaxing retinotomy + silicone oil tamponade
Prognosis
- Macula-on RRD repaired promptly: good visual recovery (>6/12 in most)
- Macula-off RRD: Better visual outcomes if surgery within 72 hours; results further decline beyond 7–10 days
- PVR is the leading cause of surgical failure in RRD repair
Sources: Kanski's Clinical Ophthalmology 10th ed., The Wills Eye Manual, Goldman-Cecil Medicine
Rhegmatogenous Rd
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
rhegmatogenous retinal detachment fundus horseshoe tear
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Here is a focused, postgraduate-level answer on Rhegmatogenous Retinal Detachment (RRD).
Rhegmatogenous Retinal Detachment (RRD)
Definition & Etymology
The term "rhegmatogenous" derives from the Greek rhegma = break. RRD is the most common form of retinal detachment, defined as separation of the neurosensory retina from the RPE caused by a full-thickness retinal break, through which liquefied vitreous passes into the subretinal space.
Epidemiology
- Incidence: ~1 in 10,000 per year
- Both eyes eventually affected in ~10%
- Peak age: 50–70 years (PVD-related); younger in high myopes and post-trauma
Pathogenesis
Two conditions must coexist:
- A full-thickness retinal break (tear or hole)
- Vitreous liquefaction (synchysis) + vitreoretinal traction
Without liquefaction and traction, a break alone will almost never cause detachment. Once these coexist, liquid vitreous flows through the break into the subretinal space, progressively separating the neurosensory retina from the RPE.
Types of Retinal Breaks
| Type | Mechanism | Appearance |
|---|---|---|
| Horseshoe (U-) tear | Vitreous traction avulses flap of retina | U-shaped, red, elevated flap — highest risk |
| Operculated hole | Flap completely torn off | Round hole with floating operculum |
| Atrophic round hole | Degeneration (e.g., lattice) | Small, round, no vitreous traction |
| Dialysis | Avulsion at ora serrata — blunt trauma | Circumferential tear; young males |
| Giant tear | ≥90° circumferential break | Large, rolled posterior flap |
| Macular hole | Posterior pole — in high myopia | Central hole with shallow SRF |
Risk Factors / Predisposing Lesions
Ocular:
- High myopia — >40% of all RRDs; elongated globe, vitreous degeneration, chorioretinal atrophy
- Posterior vitreous detachment (PVD) — the most common precipitant of horseshoe tears
- Lattice degeneration — present in ~8% of the population; found in ~40% of eyes with RRD. Areas of spindle-shaped retinal thinning with sclerosed vessels (white arborizing lines), exaggerated vitreous adhesions at margins → tractional tears on PVD
- Snailtrack degeneration — frost-like peripheral white areas; round holes common
- Aphakia/pseudophakia — especially with vitreous loss at surgery
- Trauma — dialysis at ora serrata
- Fellow eye — ~10% bilateral lifetime risk
Systemic:
- Marfan syndrome, Stickler syndrome (hereditary vitreoretinopathy)
- Family history
Symptoms
In ~60% of patients, premonitory symptoms occur with acute PVD:
- Photopsia (flashes) — traction on the retina; does not predict break location
- Floaters — vitreous debris or blood; a sudden "shower" of floaters suggests PVD with possible tear
- Curtain/shadow across visual field — field defect in the opposite quadrant to the primary break
- Lower field defect noticed sooner than upper; upper break → lower field curtain
- Some patients note relief on waking (overnight SRF absorption) that recurs later in day
- Loss of central vision — fovea involved by SRF, or large bullous RD obscuring visual axis
Signs
Anterior Segment
| Sign | Significance |
|---|---|
| Tobacco dust / Shafer's sign — pigment cells in anterior vitreous | Highly specific for RRD; virtually pathognomonic |
| Reduced IOP (~5 mmHg below fellow eye) | Increased RPE fluid pumping |
| Very low IOP | Associated choroidal detachment |
| Raised IOP + mild uveitis | Schwartz-Matsuo syndrome — photoreceptor outer segments clog trabecular meshwork; resolves with RD repair |
| Mild iritis | Common; do not overlook underlying RD |
| RAPD (Marcus Gunn pupil) | Extensive RD |
Fundus — Fresh RRD
- Convex, corrugated, slightly opaque retinal elevation (retinal edema)
- Loss of underlying choroidal pattern
- Retinal blood vessels appear darker and tortuous over detached area
- Retinal break: red discontinuity (colour contrast with choroid); less visible in high myopia
Fundus — Longstanding RRD
- Intraretinal cysts — develop after ~1 year
- Subretinal demarcation lines ("tide marks"/"high-water marks") — RPE cell proliferation at edge of SRF; appear after ~3 months; represent sites of increased adhesion
- Retinal atrophy and thinning
- Fixed folds, subretinal precipitates
Break Localization — Modified Lincoff's Rules
Subretinal fluid (SRF) spread governed by: gravity + anatomical limits (ora serrata, optic nerve) + break location.
| SRF Pattern | Likely Primary Break |
|---|---|
| Shallow inferior RD, higher on temporal side | Inferior temporal |
| Inferior RD with equal fluid levels | 6 o'clock |
| Bullous inferior RD | Above horizontal meridian |
| SRF crosses midline above | Near 12 o'clock; lower edge = side of break |
| Upper nasal break | SRF revolves round disc; rises on temporal side |
| Subtotal RD with superior wedge attached | Break in periphery nearest highest border |
Break distribution: 60% superotemporal · 15% superonasal · 15% inferotemporal · 10% inferonasal
~50% of eyes have more than one break, often within 90° of each other → systematic search of entire periphery mandatory.
Investigations
- Binocular indirect ophthalmoscopy (BIO) with scleral depression — both eyes; identify all breaks; note SRF extent and macula status
- Slit lamp + 90D/widefield lens — vitreous assessment, tobacco dust, posterior breaks
- B-scan ultrasound — when fundal view obscured (vitreous haemorrhage, dense cataract, corneal opacification); RD on B-scan = bright hyperechoic membrane attached at disc and ora
- OCT — macula status (on/off/sub-foveal fluid), epiretinal membrane, intraretinal cysts
- Examination of fellow eye — essential given 10% bilateral risk
Differential Diagnosis
| Condition | Key Differentiator |
|---|---|
| Retinoschisis | Bilateral, smooth, dome-shaped, inferotemporal; absolute VF defect; no pigment cells in vitreous; choroidal pattern visible |
| Tractional RD | Concave, smooth, immobile; fibrous membranes; doesn't reach ora serrata |
| Exudative RD | No break; convex; fluid shifts with gravity; underlying cause (tumour, inflammation) |
| Choroidal detachment | Brown, extends beyond ora serrata; limited posteriorly by vortex veins; low IOP; no vitreous pigment |
Treatment
Pre-operative
- Patient fasts if urgent surgery planned
- Bed rest with head positioning so break is most dependent (reduces SRF)
- Do not apply patch or pad (prevents visual monitoring)
Urgency
| Situation | Urgency |
|---|---|
| Macula-on RRD | Emergency — operate ASAP |
| Macula-off RRD | Surgery within 7–10 days (visual outcome equivalent if done within this window) |
| Dense vitreous haemorrhage + RD on B-scan | Urgent PPV |
| Combined tractional-RRD | Urgent — SRF spreads rapidly |
TIP: Even when the macula is already off, visual results are better if surgery is completed within 72 hours. — Kanski's Clinical Ophthalmology
Surgical Options
1. Pneumatic Retinopexy
- Principle: Intravitreal gas bubble (SF₆ or C₃F₈) expands, tamponades the break from inside; cryotherapy or laser applied to create permanent chorioretinal adhesion
- Head positioning: Patient positions so bubble directly covers the break
- Indication: Single break or cluster of breaks <2 clock hours in the upper 2/3 of peripheral retina; uncomplicated RRD; office-based procedure
- Limitation: Lower success rate than scleral buckling
2. Scleral Buckling (External Surgery)
- Principle: Silicone explant sutured to sclera creates inward indentation (buckle) → opposes RPE to sensory retina, reduces vitreoretinal traction, closes break
- Technique: Peritomy → break localization → cryotherapy to break → explant sutured (radial/segmental/circumferential/encircling) → SRF drainage if needed
- Mandatory: For post-traumatic dialysis
- Explant configuration: Radial (single peripheral tear), segmental (cluster), circumferential or encircling (multiple breaks/high PVR risk)
- Complications: Diplopia, CME (~25%), epiretinal membrane (~15%), buckle extrusion/infection, anterior segment ischaemia (encircling), elevated IOP, choroidal detachment
3. Pars Plana Vitrectomy (PPV — Internal Surgery)
- Principle: Remove vitreous + posterior hyaloid (relieving traction) → drain SRF internally → laser/cryopexy to break → intraocular tamponade to hold retina in place
- 3-port technique: Infusion cannula (4 mm from limbus in phakic; 3.5 mm in pseudophakic) + vitreous cutter + light probe at 10 and 2 o'clock
- Tamponade options: Air, SF₆, C₃F₈ gas (short-to-long acting); silicone oil (for PVR, inferior breaks, giant tears, unable to posture)
- PPV preferred over SB when:
- Breaks not visualizable (haemorrhage, media opacity)
- Giant tears, large posterior breaks
- Proliferative vitreoretinopathy (PVR)
- Pseudophakic RD
- Failed prior scleral buckle
Complications of RRD
1. Proliferative Vitreoretinopathy (PVR) — Leading Cause of Surgical Failure
Epiretinal/subretinal membrane formation → fixed retinal folds and traction
| Grade | Features |
|---|---|
| A (minimal) | Diffuse vitreous haze, tobacco dust, inferior pigment clumps |
| B (moderate) | Inner surface wrinkling, rolled break edges, vascular tortuosity, retinal stiffness |
| C (marked) | Rigid full-thickness star folds; anterior (A) or posterior (P); funnel RD in advanced disease |
Management of PVR: PPV + membrane/ILM peeling ± relaxing retinotomy + silicone oil tamponade
2. Macular complications (macula-off RD)
- Reduced final visual acuity even after successful reattachment
- Epiretinal membrane, CME, persistent subfoveal fluid, photoreceptor loss
Prognosis
- Macula-on, prompt repair: >6/12 visual acuity achievable in most cases
- Macula-off <72 hours: Good recovery likely
- Macula-off >1 week: Significant photoreceptor atrophy; poorer prognosis
- Primary anatomical success rate: ~80–90% with a single procedure; >95% with re-operations
- PVR is the principal cause of failure
Sources: Kanski's Clinical Ophthalmology 10th ed., The Wills Eye Manual, Goldman-Cecil Medicine
Cscr for 20 marks
Finding Sources
Searching Images
central serous chorioretinopathy OCT fundus fluorescein angiography
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Searching PubMed
central serous chorioretinopathy treatment photodynamic therapy mineralocorticoid
Reading File
Loading Image
Here is a comprehensive 20-mark answer on Central Serous Chorioretinopathy (CSCR/CSC), structured for a postgraduate ophthalmology examination.
Central Serous Chorioretinopathy (CSCR)
Definition
Central serous chorioretinopathy (CSCR) is an idiopathic disorder of the macula characterized by a localized serous detachment of the neurosensory retina at the posterior pole, secondary to leakage from the choriocapillaris through one or more hyperpermeable RPE sites. It belongs to the pachychoroid spectrum of diseases.
Epidemiology & Demography
- Predominantly affects young to middle-aged males (3rd–5th decade)
- Male : Female ratio = 3:1; females with CSCR tend to be older
- Usually unilateral, but fellow eye shows signs of pachychoroid pigment epitheliopathy in ~2/3 of cases
- Incidence: ~10 per 100,000 per year in males
- Associated with Type A personality (stress-prone, perfectionistic individuals)
Pathogenesis
The current understanding places CSCR within the pachychoroid spectrum:
Choroidal hyperpermeability / pachychoroid
↓
Dilated outer choroidal vessels (Haller's layer)
↓
Compression of choriocapillaris → ischaemia
↓
RPE dysfunction / decompensation
↓
Breakdown of outer blood-retinal barrier
↓
Leakage of fluid through RPE defect
↓
Accumulation of subretinal fluid → neurosensory detachment
Cortisol / mineralocorticoid pathway:
- Both endogenous (stress, Cushing syndrome) and exogenous corticosteroids upregulate mineralocorticoid receptors in the choroid → choroidal vasodilation and hyperpermeability
- This explains the strong association with steroid use and stress
Risk Factors / Associations
| Category | Examples |
|---|---|
| Steroid use | Systemic, inhaled, intranasal, topical skin, intra-articular — any route |
| Endogenous hypercortisolism | Cushing syndrome, cortisol-producing adrenal adenoma |
| Stress / Type A personality | Psychological or physiologic stress |
| Genetic | SNP in complement factor H gene (chromosome 1) → chronic CSCR in White individuals |
| Systemic | Hypertension, obstructive sleep apnoea, Helicobacter pylori infection, renal dialysis, organ transplantation |
| Pregnancy | Especially 3rd trimester; usually resolves postpartum |
| Autoimmune | Lupus (SLE) |
Classification
| Type | Duration | Features |
|---|---|---|
| Acute CSCR | <3–4 months | Classic presentation; spontaneous resolution common |
| Chronic CSCR | >4 months | Persistent SRF; diffuse RPE atrophy; gravitational tracts; greater risk of permanent visual loss |
| Recurrent CSCR | Multiple episodes | Progressive RPE damage with each episode |
| Bullous CSCR | Severe form | Large single or multiple serous retinal and RPE detachments |
Symptoms
- Unilateral blurring of central vision
- Metamorphopsia (distortion of straight lines)
- Micropsia (objects appear smaller — due to photoreceptor displacement by SRF)
- Acquired hypermetropia (visual acuity may improve with a low + power lens)
- Mild dyschromatopsia (colour desaturation)
- Central relative scotoma (detected on Amsler grid)
- Symptoms may fluctuate in morning (overnight reabsorption of SRF)
Signs
Visual acuity: Typically 6/9 to 6/18 (20/30–20/60); may be 20/200 in severe cases
Fundoscopy:
- Round or oval serous detachment at the macula — convex, dome-shaped, well-demarcated, with a sloping margin that merges gradually into attached retina
- Subretinal fluid is usually clear (early) or turbid (chronic); precipitates on posterior retinal surface may be present
- One or more small RPE detachments (PEDs) within the neurosensory detachment
- Focal RPE atrophy or hyperplasia at posterior pole — sites of previous episodes
- Gravitational tract — fluid tracks inferiorly from posterior pole in chronic cases (best seen on FAF)
- Bullous CSCR — extensive serous detachment, resembling exudative RD
Multimodal Imaging
1. Optical Coherence Tomography (OCT) — Primary Investigation
- Neurosensory detachment: Optically empty (black) space under the retina with dome-shaped elevation of the sensory retina
- RPE detachment (PED): Small focal elevation of RPE
- Pachychoroid: Choroidal thickening with dilated outer choroidal vessels (Haller's layer)
- Enhanced-depth imaging OCT (EDI-OCT): Demonstrates choroidal thickening — hallmark of pachychoroid
2. Fundus Fluorescein Angiography (FFA/IVFA)
Two classic patterns:
| Pattern | Frequency | Appearance |
|---|---|---|
| "Ink blot" | ~80–90% | Early hyperfluorescent spot that gradually enlarges and fills the detachment area |
| "Smoke stack" | ~10–20% | Vertical column of dye rising to the top, then spreading laterally — pathognomonic of CSCR |
- Underlying PEDs may be demonstrated
- Multiple foci of leakage in chronic CSCR
3. Indocyanine Green Angiography (ICGA)
- Early phase: Delayed choroidal artery filling, dilated outer choroidal vessels
- Mid-phase: Multifocal areas of choroidal hyperfluorescence (choroidal hyperpermeability) — often more extensive than clinically evident
- Late phase: Persistent hyperfluorescence
- ICGA is essential for identifying active leakage site(s) before PDT
4. Fundus Autofluorescence (FAF)
- Hypoautofluorescence at leakage site (RPE loss)
- Hyperautofluorescence — excessive RPE lipofuscin accumulation at adjacent areas
- Gravitational tract: Hyperfluorescent linear streak inferiorly in chronic/recurrent disease
5. Amsler Grid
- Confirms metamorphopsia; documents the area of field involvement
Multimodal Imaging Summary
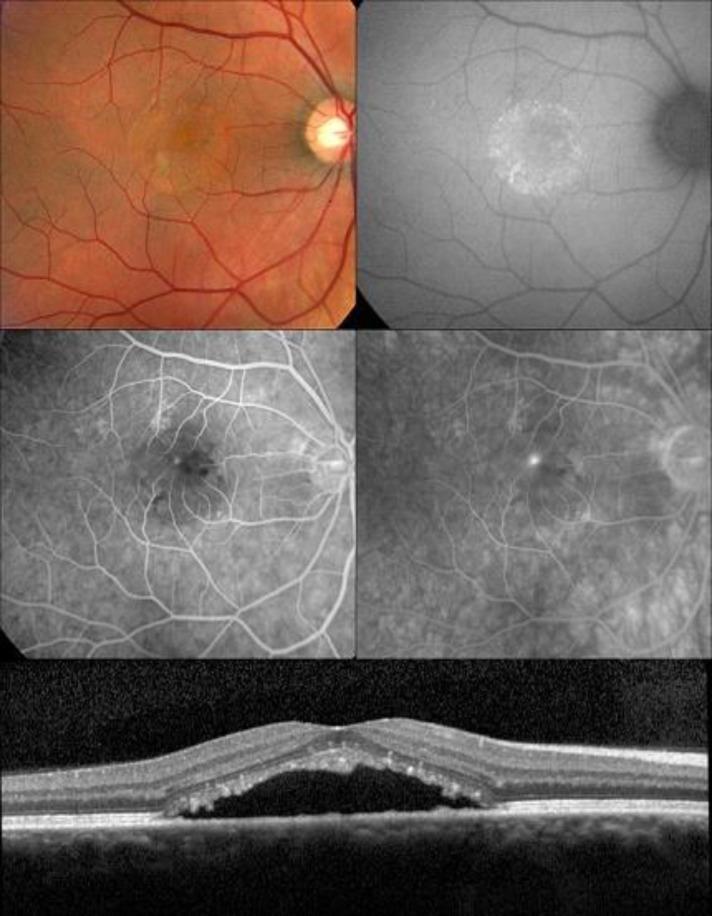
Multimodal imaging panel in CSCR: Color fundus, FAF, FA, ICGA, and OCT showing the pathognomonic findings — serous neurosensory detachment, focal leakage hotspot, and pachychoroid.
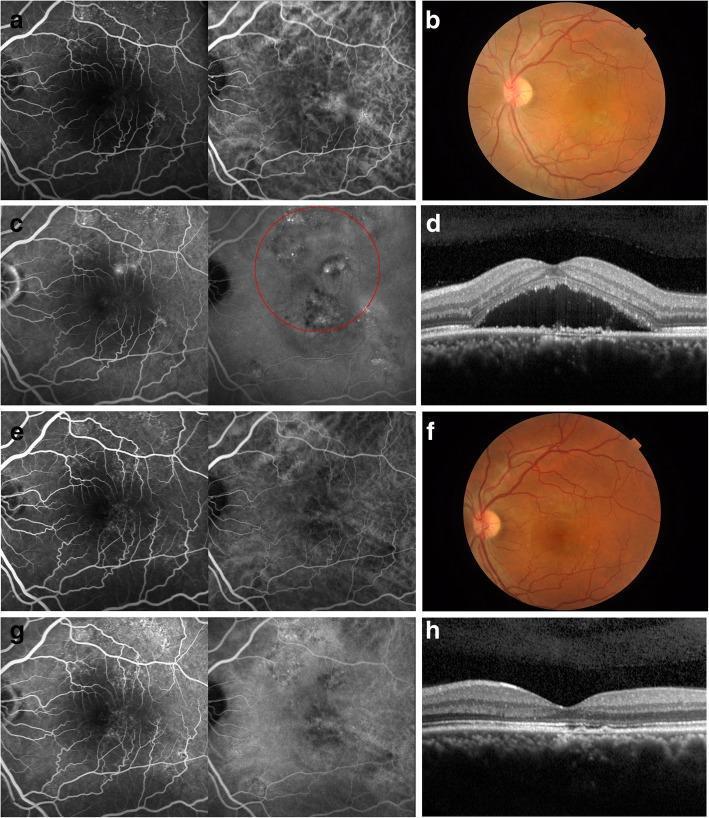
PDT treatment response in chronic CSCR: Complete resolution of SRF and leakage confirmed by FA and OCT at 6-month follow-up.
Differential Diagnosis
| Condition | Key Differentiating Feature |
|---|---|
| Age-related macular degeneration (wet) | Age ≥50; drusen; subretinal blood/exudates; CNV on OCT-A/ICGA |
| Optic disc pit maculopathy | Serous RD contiguous with optic disc; no leakage on FFA; pit visible on disc |
| Choroidal tumour (haemangioma, melanoma) | Solid lesion on B-scan; ICGA shows vascular tumour |
| Vogt-Koyanagi-Harada (VKH) disease | Bilateral; granulomatous uveitis; exudative; systemic features |
| Exudative RRD | Peripheral retinal break; SRF extends to periphery |
| Macular PED | More distinct, dome-shaped RPE elevation on OCT; no neurosensory detachment initially |
| Uveal effusion syndrome | Peripheral ciliochoroidal detachment; "leopard spot" RPE changes |
| Hypertensive retinopathy | Arteriolar changes; bilateral; flame haemorrhages; CWS |
Natural History / Course
- Acute CSCR: Spontaneous resolution within 3–6 months in ~80% of cases with return to near-normal vision
- Recurrence: Up to 50% of cases recur
- Chronic CSCR: ~15% follow a chronic course (>4 months); prolonged SRF leads to gradual photoreceptor and RPE degeneration → permanent visual loss
- Complications: Cystoid macular oedema (CMO), macular neovascularisation (MNV), RPE tears (in a small minority)
Management
Step 1 — Identify and Withdraw Precipitating Cause
- Stop all corticosteroids (systemic, topical, inhaled, intranasal) wherever possible — this alone may lead to resolution
- Avoid NSAIDs, excessive stress, and sleep deprivation
Step 2 — Observation (Acute CSCR)
- Most acute cases resolve spontaneously within 3–6 months
- Follow up every 6–8 weeks with OCT and VA monitoring
- All treatment modalities carry risk of RPE tear — do not over-treat early cases
Step 3 — Indications for Active Treatment
Active intervention is indicated when:
- SRF persists for >3–4 months without sign of resolution
- Recurrence in an eye with previous permanent visual deficit
- Visual deterioration affecting occupational or daily function
- Fellow eye previously suffered permanent visual loss
- Chronic CSCR with ongoing RPE damage
Treatment Options
A. Photodynamic Therapy (PDT) with Verteporfin — Gold Standard for Chronic CSCR
- Half-dose / reduced-fluence PDT: Verteporfin at 30–50% of standard MNV dose + 50% light intensity
- Mechanism: Selectively obliterates hyperpermeable choriocapillaris → reduces choroidal blood flow → resolves SRF
- Leakage site identified on ICGA before treatment
- Results: Complete resolution in the majority of cases, including severe chronic cases
- Lower risk of significant choroidal ischaemia compared to full-dose PDT
- Anti-VEGF agents commonly used in conjunction with PDT; bevacizumab alone is not effective unless coexisting MNV is present
B. Subthreshold (Micropulse) Diode Laser
- Delivers energy only to RPE cells at the leakage site without visible retinal damage
- Uses 810 nm diode laser in a micropulse mode (on/off cycling)
- Advantage: No scotoma, no chorioretinal scar, can treat juxtafoveal leaks
- Shows good results in several studies; significantly less OCT-detectable retinal damage than conventional laser
- Used when leakage site is away from the fovea and identifiable on FFA
C. Conventional Laser Photocoagulation
- Direct treatment of FFA-identified leakage site
- May accelerate visual recovery but no long-term benefit shown
- Risk: CNV formation at laser scar; use low intensity settings
- Indications: Leakage site is >300 µm from the foveal centre; occupational urgency; recurrent disease with prior visual loss
- Contraindicated if leakage is subfoveal or juxtafoveal
D. Mineralocorticoid Receptor Antagonists (MRAs)
- Spironolactone (40 mg twice daily) and Eplerenone (25–50 mg daily)
- Mechanism: Block mineralocorticoid receptors in choroidal endothelium → reduce choroidal hyperpermeability
- Evidence (2025 Cochrane network meta-analysis [PMID 40522203]; 2025 meta-analysis of eplerenone/spironolactone [PMID 40513762]): Associated with improved anatomic and visual outcomes in chronic CSCR
- Oral spironolactone may accelerate SRF resorption even in acute CSCR
- Side effects: Hyperkalaemia, gynaecomastia (spironolactone); eplerenone has better tolerability
E. Anti-VEGF Therapy
- Not first-line for uncomplicated CSCR
- Indicated when macular neovascularisation (MNV) develops as a complication
- Bevacizumab alone: no benefit in CSCR without MNV
F. Others (limited evidence)
- Aspirin, beta-blockers, mifepristone (anti-progesterone): case reports only; not routine practice
Treatment Decision Algorithm
Acute CSCR (<3–4 months)
↓
Withdraw steroids + Observe
↓
No resolution at 3–4 months / occupational urgency
↓
Leakage site identifiable?
├─ Away from fovea → Micropulse diode laser OR conventional laser (low intensity)
└─ Subfoveal/diffuse → Half-dose PDT (preferred) + consider MRA
Chronic CSCR (>4 months)
↓
Half-dose verteporfin PDT (first line) ± MRA (spironolactone/eplerenone)
↓
MNV develops → Add anti-VEGF
Prognosis
| Type | Visual Outcome |
|---|---|
| Acute CSCR | ~80% resolve spontaneously; near-normal VA recoverable |
| Recurrent CSCR | Progressive RPE damage; permanent VA reduction risk |
| Chronic CSCR | Significant risk of permanent photoreceptor and RPE degeneration; worse outcome with delay |
| Post-PDT | Majority achieve complete SRF resolution; visual improvement in most |
Recent Evidence
- A 2025 Cochrane network meta-analysis (PMID 40522203) comparing all interventions for CSCR confirmed PDT and mineralocorticoid antagonists as the treatments with the strongest evidence base for chronic CSCR.
- A 2025 systematic review and meta-analysis (PMID 40513762) specifically on eplerenone and spironolactone confirmed improved anatomic and visual outcomes in chronic CSCR with both agents.
Sources: Kanski's Clinical Ophthalmology 10th ed., The Wills Eye Manual, Harrison's Principles of Internal Medicine 22nd ed.; Cochrane Database Syst Rev 2025; Am J Ophthalmol 2025
Eales disease
Finding Sources
Searching Images
Eales disease retinal vasculitis periphlebitis fundus fluorescein angiography
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Here is a comprehensive answer on Eales Disease, structured for a postgraduate ophthalmology examination.
Eales Disease
Definition & Historical Note
Eales disease is an idiopathic occlusive peripheral periphlebitis of the retina, characterised by three overlapping stages — inflammatory, occlusive, and neovascular — with recurrent vitreous haemorrhage as the hallmark clinical presentation. It was first described by Henry Eales in 1880 in young men with epistaxis and recurrent vitreous haemorrhage ("retinal haemorrhage in young men").
Epidemiology
- Predominantly affects young males in the 2nd–4th decade of life
- Male : Female ratio ≈ 3:1
- Rare in White people; important cause of visual morbidity in young South Asian males (Indian subcontinent, Middle East)
- Typically bilateral, though presentation is often asymmetrical
- Incidence higher in regions with high prevalence of tuberculosis
Aetiology & Pathogenesis
Eales disease is considered an idiopathic condition — a diagnosis of exclusion after ruling out other causes of retinal vasculitis and peripheral neovascularization.
Proposed Mechanisms:
1. Tubercular protein hypersensitivity (most widely accepted theory)
- It is hypothesized that Eales disease represents a delayed-type hypersensitivity reaction to Mycobacterium tuberculosis antigens (tuberculoprotein)
- Evidence: High prevalence in TB-endemic regions; positive Mantoux test in many patients; PCR detection of mycobacterial DNA in vitreous; some cases classified as frank tuberculous vasculitis
- However, evidence is conflicting and TB is not isolated in all cases
2. Autoimmune mechanism
- Cell-mediated immune response targeting retinal vascular endothelium
- Activated T lymphocytes infiltrate perivascular spaces → perivenous inflammation
3. Oxidative stress
- Impaired free radical scavenging; increased lipid peroxidation demonstrated in patients with Eales disease
Pathological sequence:
Perivenous inflammation (periphlebitis)
↓
Endothelial cell damage → vascular wall thickening
↓
Venous occlusion → peripheral capillary non-perfusion
↓
Retinal ischaemia → VEGF upregulation
↓
Peripheral retinal neovascularization
↓
Vitreous haemorrhage / tractional retinal detachment
Staging (Three Overlapping Stages)
| Stage | Features |
|---|---|
| Stage 1 — Inflammatory (Periphlebitis) | Perivenous sheathing, superficial retinal haemorrhages, cotton-wool spots, engorgement of peripheral veins |
| Stage 2 — Occlusive | Branch retinal vein occlusion, peripheral capillary non-perfusion, microaneurysms, arteriovenous shunts, telangiectasia |
| Stage 3 — Proliferative (Neovascular) | Peripheral NVE (neovascularization elsewhere), disc NVD (neovascularization of disc), recurrent vitreous haemorrhage |
Progression through stages is not inevitable and stages often overlap.
Symptoms
- Floaters — early symptom; black dots or cobwebs
- Sudden painless visual reduction — due to vitreous haemorrhage (most common presentation)
- Symptoms may be recurrent (vitreous haemorrhage recurs in about 1/3 of eyes)
- Bilateral visual symptoms — though not always simultaneous
- Neurological features (headache, cerebrovascular events) — rarely reported; Eales disease is also listed as a rare cause of brain infarction
Signs
Anterior Segment
- Mild anterior uveitis — common
- Vitreous haemorrhage — fresh or resolving (orange-red or yellowish opacity)
- Posterior vitreous detachment with fibrovascular membranes in advanced cases
Fundus (in order of stage)
Inflammatory stage:
- Perivenous sheathing — white cuffing around peripheral retinal veins (periphlebitis)
- Superficial retinal haemorrhages (flame-shaped) around affected veins
- Cotton-wool spots (nerve fibre layer infarcts) in area of ischaemia
- Pigmented chorioretinal scars (evidence of old lesions)
Occlusive stage:
- Branch retinal vein occlusion (BRVO) in periphery
- Peripheral capillary non-perfusion — detected best on FFA; avascular zones
- Microaneurysms, arteriovenous shunts, telangiectatic vessels at junction of perfused and non-perfused retina
Proliferative stage:
- Peripheral NVE — frond-like new vessel networks at ischaemia margin
- NVD (disc new vessels) — occasionally
- Vitreous haemorrhage — recurrent; usually limited in amount; absorbs over weeks (may persist)
- Macular involvement — uncommon but can occur with CMO or ERM
Complications:
- Tractional retinal detachment (TRD)
- Macular epiretinal membrane
- Neovascular glaucoma (rubeosis iridis)
- Complicated cataract
- Vitreous fibrosis
Fundus and FFA Images
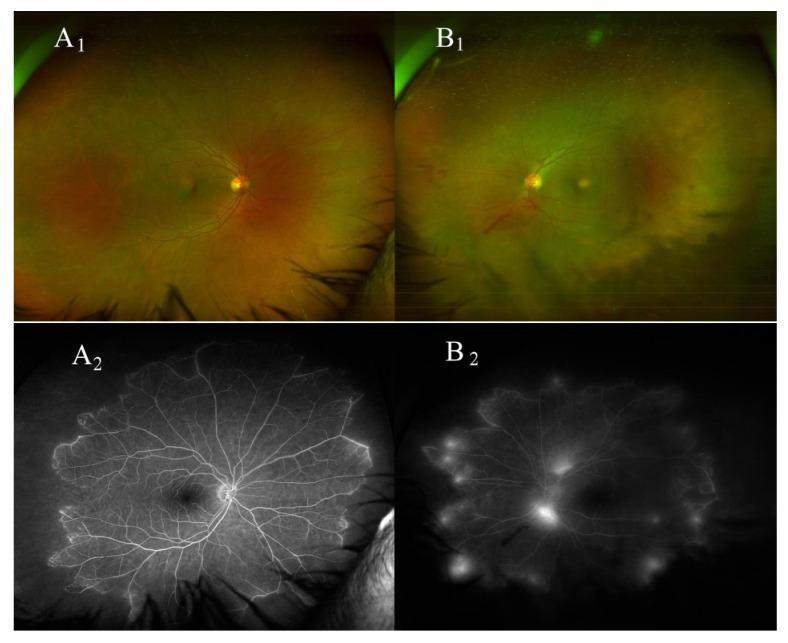
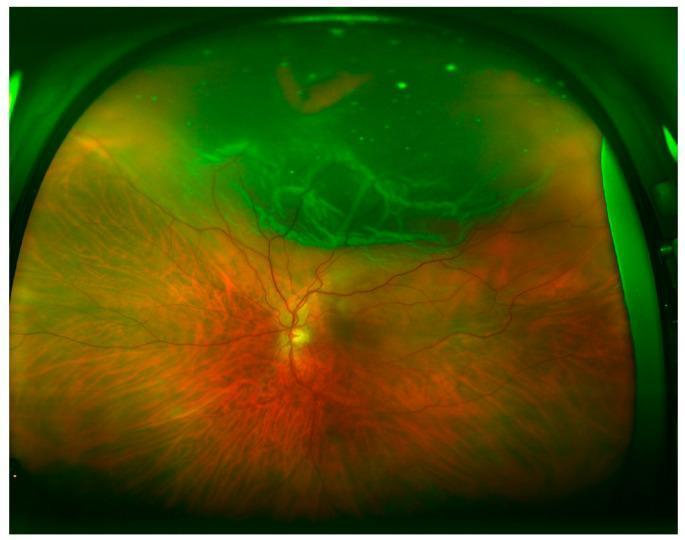
Bilateral Eales disease on wide-field imaging and FFA: peripheral periphlebitis, extensive capillary non-perfusion, and active neovascularization with leakage.

Obliterative periphlebitis in Eales disease: sclerosed peripheral vessels and active NVE on FFA with zones of non-perfusion.
Investigations
Ocular
- Fundus fluorescein angiography (FFA) / Wide-field FFA — essential
- Active vasculitis: perivenous hyperfluorescence (staining of vessel walls), leakage
- Areas of capillary non-perfusion (dark avascular zones)
- Neovascularization: bright hyperfluorescent fronds with late leakage
- Wide-field imaging is particularly helpful for peripheral disease mapping
- B-scan ultrasonography — if vitreous haemorrhage obscures the fundus; rules out TRD
- OCT — macular assessment; CMO, ERM, sub-foveal fluid
- Indirect ophthalmoscopy with scleral depression — assess peripheral retina
Systemic (to exclude other causes)
- Mantoux (tuberculin skin test) / IGRA (QuantiFERON-TB Gold) — for TB exposure
- Chest X-ray / CT chest — hilar lymphadenopathy, TB, sarcoidosis
- ACE (angiotensin-converting enzyme) levels — sarcoidosis
- Haemoglobin electrophoresis — sickle cell disease
- VDRL / FTA-ABS — syphilis
- FBC, ESR, CRP — systemic inflammation
- ANA, ANCA — collagen vascular disease
- Serum glucose, HbA1c — diabetes
- PCR of vitreous — for Mycobacterium tuberculosis DNA (in selected cases)
Differential Diagnosis
| Condition | Key Differentiating Feature |
|---|---|
| Diabetic retinopathy | Bilateral symmetric; posterior > peripheral; microaneurysms, hard exudates |
| Sickle cell retinopathy | "Sea fan" NVE; salmon-patch haemorrhages; Hb electrophoresis abnormal |
| Sarcoidosis | "Candlewax drippings" periphlebitis; hilar adenopathy; raised ACE |
| Syphilis | Serological tests positive; treatable |
| Tuberculosis | Active TB lesions elsewhere; AFB; response to ATT |
| Branch retinal vein occlusion | Unilateral; sectoral distribution; posterior; no periphlebitis |
| Pars planitis | Snowbanking in inferior pars plana; "snowballs" in vitreous |
| Retinopathy of prematurity | History of prematurity; stage-based presentation |
| Behçet disease | Occlusive arteritis/phlebitis; oral and genital ulcers; HLA-B51 |
| Multiple sclerosis | Periphlebitis; neurological features; MRI white matter lesions |
Eales disease is a diagnosis of exclusion — all the above must be ruled out before the diagnosis is made. — The Wills Eye Manual
Treatment
Management is stage-directed:
Stage 1 — Inflammatory (Periphlebitis)
Corticosteroids:
- Periocular, systemic, topical and intravitreal steroids are helpful in the inflammatory stage
- Systemic prednisolone (1 mg/kg/day tapered over weeks) for active periphlebitis
- Topical steroids for associated anterior uveitis
Antitubercular therapy (ATT):
- Strongly advocated by some authorities but controversial
- Recommended in combination with steroids when:
- Strongly positive tuberculin test (Mantoux) or QuantiFERON positive
- Severe ocular inflammatory signs
- To avoid reactivation of latent TB during steroid therapy
- Standard 4-drug ATT: RHEZ (Rifampicin, Isoniazid, Ethambutol, Pyrazinamide) × 2 months → RH × 4 months
- Monitor for ethambutol-related optic neuropathy
Stage 2 — Occlusive (Ischaemic)
Scatter laser photocoagulation (PRP to non-perfused retina):
- Applied to all areas of capillary non-perfusion (identified on FFA)
- Mechanism: Destroys hypoxic outer retinal cells → reduces VEGF → prevents/treats neovascularization
- Performed in sessions; wide-field FFA guides treatment
- Cryotherapy of non-perfused retina — an alternative if laser is not feasible (anterior lesions, media opacity)
Stage 3 — Proliferative (Neovascular)
Intravitreal anti-VEGF agents (bevacizumab / ranibizumab):
- Commonly used for active neovascularization
- Causes rapid regression of NVE/NVD
- Used as adjunct to laser (pre-operatively before vitrectomy to reduce bleeding risk)
- Multiple injections may be needed
Vitrectomy (Pars plana vitrectomy — PPV):
- Indicated for:
- Persistent/dense vitreous haemorrhage (non-clearing despite 3–4 months)
- Tractional retinal detachment (TRD)
- Macular epiretinal membrane causing significant visual loss
- Combined TRD-RRD
- Combined with intraoperative laser (endolaser photocoagulation) and anti-VEGF
Treatment Summary Table
| Stage | Treatment |
|---|---|
| Inflammatory | Corticosteroids (systemic/periocular/topical/IVT) ± ATT |
| Occlusive | Scatter laser PRP to non-perfused retina; cryotherapy |
| Neovascular | Anti-VEGF (bevacizumab/ranibizumab) + laser PRP |
| Vitreous haemorrhage (persistent) | PPV + endolaser ± anti-VEGF |
| TRD | PPV + membrane peeling + tamponade |
| ERM macula | PPV + membrane peeling |
Prognosis
- Good in the majority — most cases resolve with treatment
- Spontaneous resolution of vitreous haemorrhage within weeks in many patients
- Poor prognosis factors: TRD involving the macula, neovascular glaucoma, delayed presentation, bilateral severe disease
- Recurrences are common — long-term follow-up essential
- Visual prognosis depends largely on macular sparing — macular involvement is uncommon but significantly worsens outcome
Sources: Kanski's Clinical Ophthalmology 10th ed., The Wills Eye Manual, Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.