Patient, the specific name, temperature raised, sleep is slow and comatose, chronic and comatose, took high dose of alcohol two days back, since then he is unconscious. What is the probable diagnosis and how to manage this?
Checking Date & Time
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer. Here is the full clinical analysis:
Probable Diagnosis: Wernicke's Encephalopathy (Wernicke-Korsakoff Syndrome in the making)
The clinical picture — a chronic alcohol user who consumed high-dose alcohol two days ago and has been unconscious/comatose since, with fever (raised temperature) and altered consciousness — fits Wernicke's Encephalopathy as the primary diagnosis, with hepatic encephalopathy and alcohol-induced metabolic coma as critical differentials that must be excluded concurrently.
Pathophysiology
Wernicke's Encephalopathy is an acute neuropsychiatric emergency caused by thiamine (Vitamin B₁) deficiency. In alcohol-dependent patients, thiamine deficiency arises from:
- Reduced dietary intake — alcohol replaces nutritious food
- Reduced intestinal absorption — chronic alcohol impairs thiamine uptake
- Acute precipitant — a large alcohol binge depletes remaining thiamine reserves and can precipitate acute Wernicke's
Thiamine is required for active ion transport at nerve terminals and maintenance of neuronal membrane potential. Without it, there is energy failure in metabolically active brainstem and diencephalic structures (periaqueductal gray, thalamus, mammillary bodies), causing the clinical syndrome.
"The ultimate cause of thiamine deficiency is absence of the vitamin from the diet, and the most frequent reason is that patients have substituted alcohol for vitamin-containing foods." — Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Clinical Features in This Patient
The classic triad of Wernicke's is:
- Confusion / encephalopathy (drowsiness, coma) ✅
- Ataxia (cerebellar involvement)
- Ophthalmoplegia / nystagmus (eye movement abnormalities)
Important: The full triad is present in only ~16% of cases. The Maudsley Prescribing Guidelines state that a presumptive diagnosis should be made in any alcohol-dependent patient who has any of:
- Unconsciousness/coma ✅ (present)
- Confusion ✅ (present)
- Hypothermia or hypotension
- Ataxia
- Ophthalmoplegia/nystagmus
This patient's prolonged unconsciousness (2 days) is particularly alarming, as:
"Deep stupor or coma is unusual, dangerous, and often a pre-terminal development." — Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Pathological Brain Changes
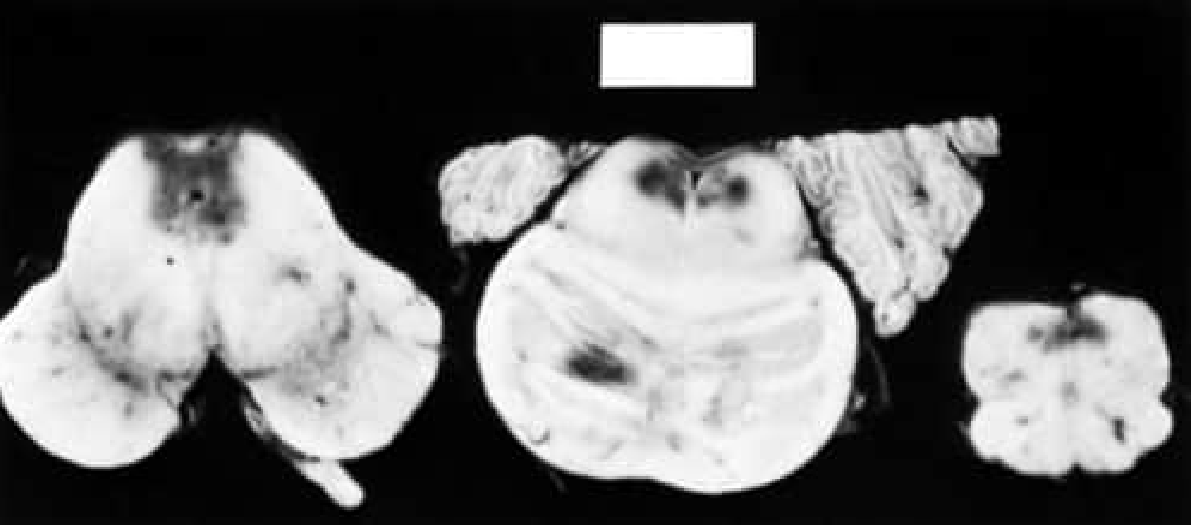
Fig. Acute Wernicke Disease: Hemorrhagic areas are seen adjacent to the fourth ventricle and aqueduct in the medulla, pons, and midbrain — Bradley & Daroff's Neurology in Clinical Practice
Lesions are symmetrically distributed around:
- Periaqueductal gray matter
- Medial thalami
- Mammillary bodies
- Cerebellar vermis and dentate nuclei
Differential Diagnoses to Exclude
| Diagnosis | Key Features |
|---|---|
| Hepatic encephalopathy | Chronic alcohol → cirrhosis → ammonia ↑ → encephalopathy; check LFTs, ammonia, asterixis |
| Hypoglycemia | Alcohol inhibits gluconeogenesis; check blood glucose urgently |
| Subdural hematoma | Alcoholics fall frequently; exclude with CT head |
| Alcohol withdrawal seizure | Usually 6–48 hours after last drink; postictal state possible |
| Delirium tremens (DTs) | Typically 48–72 hours after cessation; fever, autonomic instability |
| Aspiration pneumonia | Raised temperature in a comatose alcoholic; get CXR |
| Sepsis/meningitis | Fever + coma; do LP if clinically appropriate |
Management
🚨 Immediate — ABCDE Approach
- Airway — protect airway (intubate if GCS ≤ 8, consider ICU)
- Breathing — O₂ supplementation, watch for aspiration
- Circulation — IV access, fluids (caution: avoid glucose before thiamine)
- Disability — GCS, pupil check, blood glucose (hypoglycemia kills)
- Exposure — look for injuries, signs of liver disease, infection
💉 Specific Treatment
1. Thiamine (Vitamin B₁) — PRIORITY #1
"Wernicke-Korsakoff syndrome is a medical emergency, and early treatment with intravenous thiamine is essential." — Goodman & Gilman's Pharmacological Basis of Therapeutics
- Give thiamine BEFORE any glucose infusion — glucose infusion in a thiamine-deficient patient can precipitate acute Wernicke's or worsen existing disease
- Dose (acute Wernicke's/coma): 500 mg IV thiamine (in 100 mL normal saline over 30 min) three times daily for 2–3 days, then 250 mg IV/IM daily for 3–5 days, then switch to oral 100–300 mg/day
- Parenteral route is mandatory — oral absorption is unreliable in alcoholic/malnourished patients
2. Blood Glucose
- Check immediately; if hypoglycemic, give IV dextrose (after or with thiamine)
3. Treat Underlying Precipitants
- Infection (fever) → blood cultures, urine culture, CXR → empiric antibiotics if sepsis suspected
- Hepatic encephalopathy → lactulose, rifaximin, treat precipitating cause (GI bleed, infection)
- Electrolyte correction (Mg²⁺ is a cofactor for thiamine-dependent enzymes — replace IV magnesium if low)
4. Alcohol Withdrawal Management
- If not yet in withdrawal, anticipate it (DTs peak at 48–72 hours after last drink)
- Benzodiazepines (diazepam or lorazepam) for withdrawal seizures and agitation (titrate to Clinical Institute Withdrawal Assessment — CIWA-Ar score)
- Do not give benzodiazepines if patient is already deeply sedated/comatose (respiratory depression risk)
5. Nutritional Support
- IV multivitamins (B complex + Vitamin C)
- Nutritional supplementation as soon as airway is protected and patient can tolerate
6. Monitoring
- Continuous: ECG, SpO₂, blood pressure, urine output
- Labs: LFTs, renal function, ammonia, CBC, coagulation, electrolytes, blood cultures, blood glucose
- MRI brain (T2/FLAIR) — will show characteristic symmetric hyperintensities around mammillary bodies, periaqueductal gray, and thalami in Wernicke's
Prognosis
| Outcome | Data |
|---|---|
| Untreated Wernicke's → death | Up to 20% mortality |
| Survivors without treatment → Korsakoff syndrome | ~75–80% |
| With prompt IV thiamine | Eye signs reverse in hours; confusion improves over days |
| Korsakoff syndrome (permanent memory loss, confabulation) | Largely irreversible if thiamine is delayed |
"If untreated, Wernicke's encephalopathy progresses to Korsakoff's syndrome — permanent memory impairment, confabulation, confusion and personality changes." — Maudsley Prescribing Guidelines in Psychiatry, 15th ed.
Summary
This is a medical emergency. The most probable diagnosis is Wernicke's Encephalopathy precipitated by acute high-dose alcohol consumption on a background of chronic alcohol dependence and nutritional deficiency. The key life-saving intervention is immediate IV thiamine 500 mg TDS before any glucose, combined with airway protection, exclusion of concurrent hypoglycemia, infection, and structural brain lesions, and monitoring for alcohol withdrawal.
Sources:
- Bradley and Daroff's Neurology in Clinical Practice, 8th ed., p. 1803
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma, p. 388
- The Maudsley Prescribing Guidelines in Psychiatry, 15th ed., p. 512
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 542
This is a shared conversation. Sign in to Orris to start your own chat.