Venous thromboembolism classification based on cause
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer. Let me compile it.
VTE Classification Based on Cause
Venous thromboembolism (VTE) - encompassing deep vein thrombosis (DVT) and pulmonary embolism (PE) - is classified by cause into three broad etiologic categories, which in turn feed into two clinical categories (provoked vs. unprovoked).
I. Etiologic Classification
1. Hereditary (Inherited) Causes - Thrombophilia
These are genetic defects that either increase procoagulant activity (gain of function) or reduce natural anticoagulant activity (loss of function):
Loss-of-Function Mutations (reduced anticoagulation):
| Disorder | Notes |
|---|---|
| Antithrombin deficiency | Rare (~1/2000); can be quantitative or qualitative; heparin resistance |
| Protein C deficiency | Liver-synthesized; vitamin K-dependent; activates fibrinolysis |
| Protein S deficiency | Cofactor for activated protein C |
Gain-of-Function Mutations (increased coagulation):
| Disorder | Notes |
|---|---|
| Factor V Leiden | Most common inherited thrombophilia (~5% of whites); autosomal dominant; 5x VTE risk (heterozygous) |
| Prothrombin gene mutation (G20210A) | Second most common (~3% in whites); elevates prothrombin levels |
| Elevated factor VIII, IX, or XI levels | High heritability; factor VIII also raises arterial risk |
Suggested by: VTE at age <50 years, unprovoked/recurrent VTE, family history, thrombosis in unusual anatomic locations (mesenteric, portal, cavernous sinus veins).
2. Acquired Causes
These develop during life and create a hypercoagulable state:
| Category | Examples |
|---|---|
| Demographic/lifestyle | Advanced age, obesity, previous VTE |
| Malignancy | Active cancer (especially metastatic) - highest risk group |
| Immobility | Prolonged bed rest, long-haul travel, paralysis |
| Surgery/trauma | Major orthopedic, neurosurgery, polytrauma (highest surgical risk) |
| Medications | Estrogen (OCP, HRT), L-asparaginase, heparin (HIT) |
| Pregnancy/puerperium | 6x baseline risk; puerperium intermediate risk |
| Autoimmune | Antiphospholipid syndrome (APS), HIT |
| Systemic disease | Nephrotic syndrome, collagen vascular diseases, infection, DIC |
| Hematologic | Paroxysmal nocturnal hemoglobinuria (PNH), myeloproliferative disorders (JAK2 mutation) |
3. Mixed (Both Hereditary and Acquired)
| Condition | Notes |
|---|---|
| Hyperhomocysteinemia | Can arise from MTHFR mutation + folate deficiency; both arterial and venous risk. (Note: MTHFR mutation alone without elevated homocysteine does NOT cause VTE) |
II. Clinical Classification: Provoked vs. Unprovoked
This classification drives treatment duration decisions:
| Category | Definition | Recurrence Risk (after stopping anticoagulation) |
|---|---|---|
| Provoked | VTE triggered by an identifiable transient or persistent risk factor (surgery, trauma, cancer, immobility, estrogen) | ~5% per year |
| Unprovoked (idiopathic) | No clear precipitating factor identified | ~15% per year |
Important nuances:
- Active cancer is a persistent provoking factor (unlike surgery, which is transient)
- The 2019 ESC guidelines moved away from this binary classification toward individualized risk scoring, because "provoked" VTE with enduring risk factors can have recurrence risk comparable to "unprovoked" VTE
- Unprovoked VTE overall has a ~30-40% chance of recurrence within 10 years after stopping anticoagulation
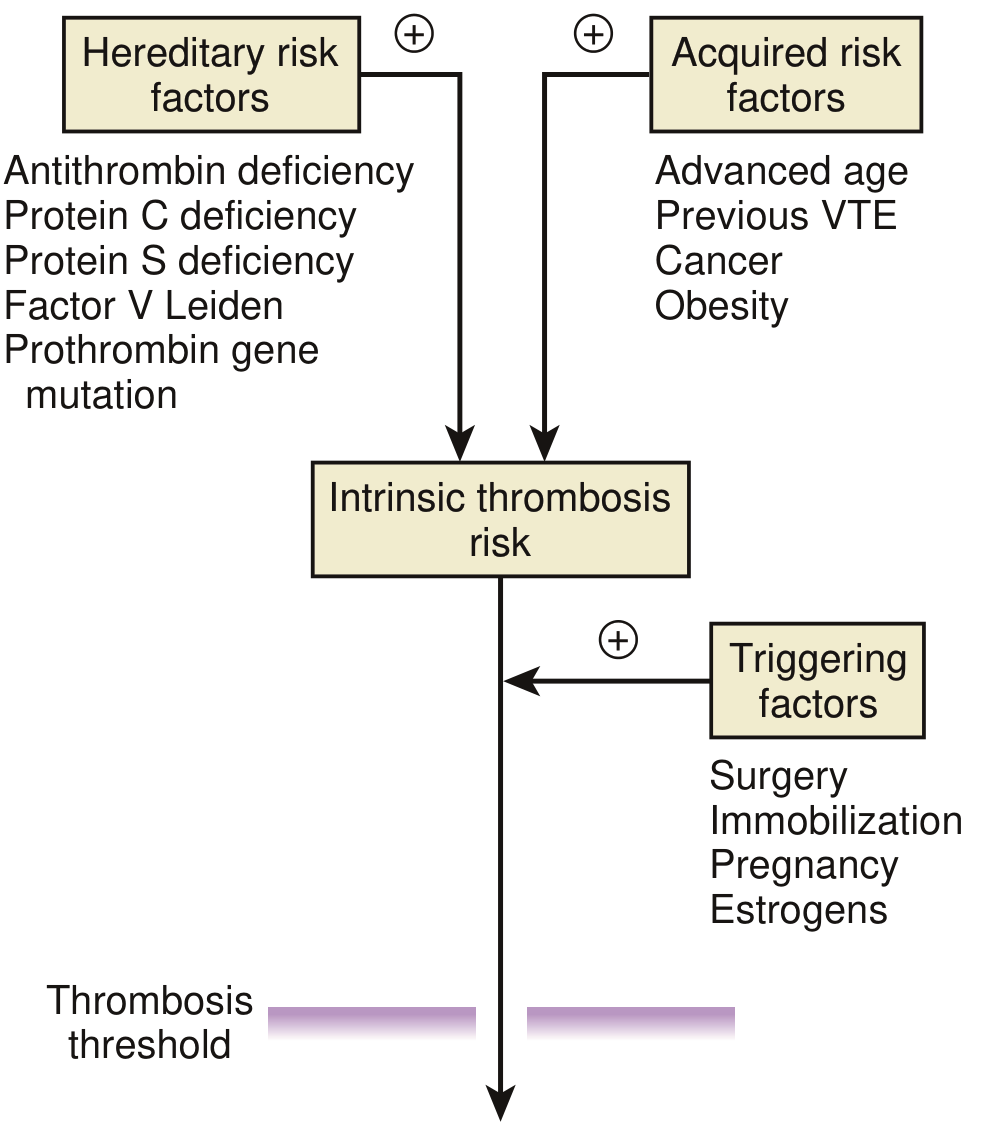
The Thrombosis Threshold Model
The following diagram from Braunwald's illustrates how these causes interact - hereditary and acquired factors combine to build an intrinsic risk, which is then tipped over the threshold by triggering events:
Risk Stratification by Level of Risk
| Risk Level | Examples |
|---|---|
| Highest | Major orthopedic surgery, neurosurgery, polytrauma, metastatic cancer |
| Intermediate | Prolonged bed rest, antiphospholipid antibodies, puerperium |
| Mild | Pregnancy, obesity, long-distance travel, oral contraceptives, HRT |
Sources: Braunwald's Heart Disease (Table 95.1, Fig. 95.9) | The Washington Manual of Medical Therapeutics | Tintinalli's Emergency Medicine | Braunwald's Heart Disease (anticoagulation duration section)
This is a shared conversation. Sign in to Orris to start your own chat.