Respiratory distress in newborn.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"neonatal respiratory distress" management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Now I have comprehensive information. Let me compile a thorough answer.
Respiratory Distress in the Newborn
Respiratory distress is the most common emergency presentation in newborns. It presents as tachypnea (>60 breaths/min), grunting, nasal flaring, intercostal/subcostal retractions, and cyanosis. The causes range from structural lung immaturity to aspiration, infection, and vascular abnormalities.
Overview of Causes
| Condition | Typical Infant | Onset |
|---|---|---|
| Respiratory Distress Syndrome (RDS) | Preterm (<34 wks) | Birth - 1st hours |
| Transient Tachypnea of Newborn (TTN) | Term/near-term, C-section | Within 6 hours, resolves <72 hrs |
| Meconium Aspiration Syndrome (MAS) | Post-mature (>42 wks) | Birth |
| Neonatal Pneumonia | Any | Variable |
| Persistent Pulmonary Hypertension (PPHN) | Term/late preterm | First hours |
| Pneumothorax | Any (esp. with MAS/RDS) | Any time |
1. Neonatal Respiratory Distress Syndrome (RDS) / Hyaline Membrane Disease
Epidemiology & Risk Factors
RDS is the most common cause of respiratory insufficiency in the newborn. It occurs in:
- ~60% of infants born before 28 weeks' gestation
- ~30% born at 28-34 weeks
- <5% born after 34 weeks
Additional risk factors: male sex, maternal diabetes (elevated insulin suppresses surfactant synthesis), cesarean section before onset of labor, multiple gestation.
Protective factors: intrauterine stress and fetal growth restriction (increase cortisol -> stimulate surfactant); antenatal corticosteroids.
Pathogenesis
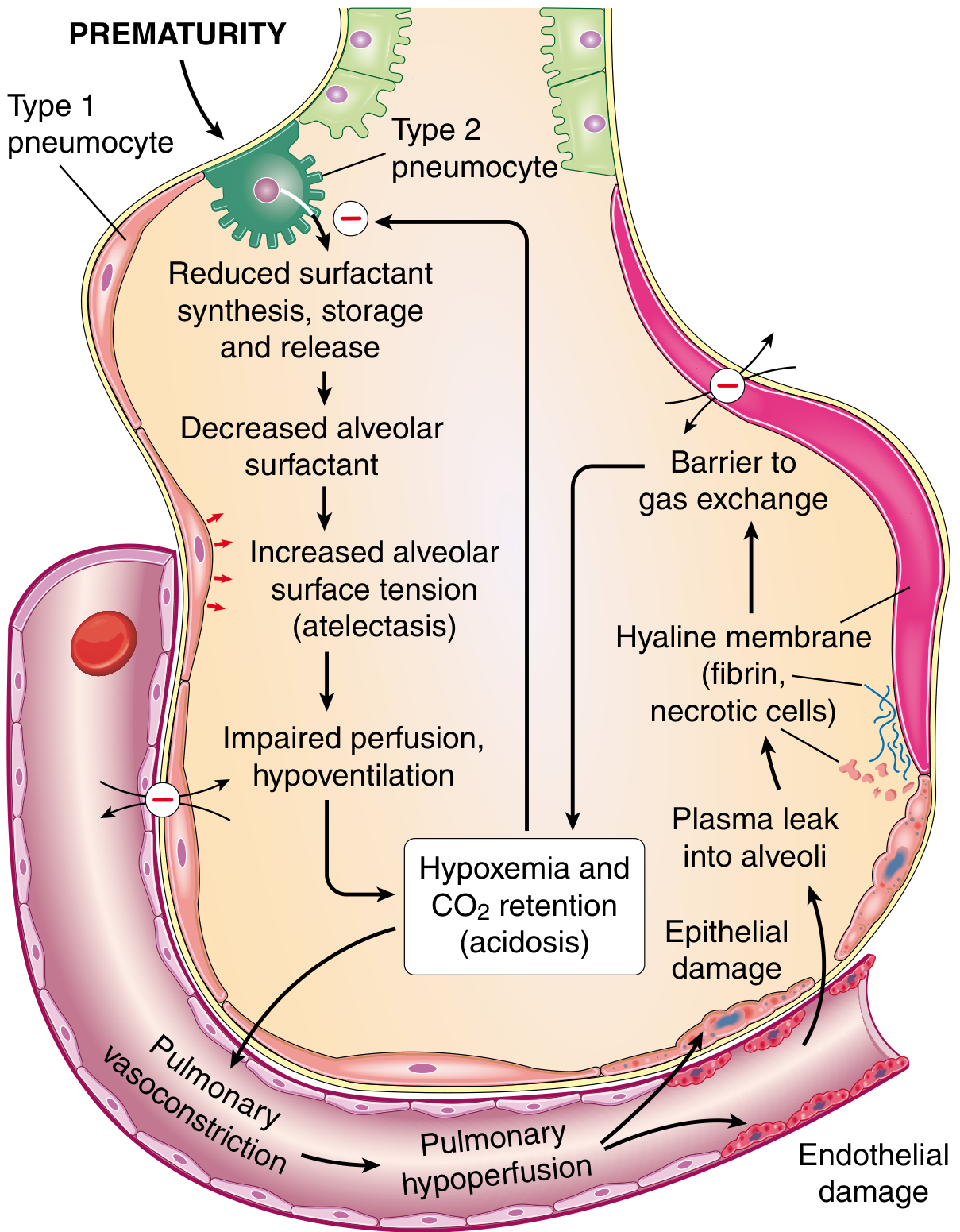
The fundamental defect is surfactant deficiency due to pulmonary immaturity. Surfactant is a complex of surface-active phospholipids (principally dipalmitoyl phosphatidylcholine/lecithin) plus hydrophilic proteins SP-A and SP-D (innate immunity) and hydrophobic proteins SP-B and SP-C (reduce alveolar surface tension). Surfactant is synthesized by type II pneumocytes and production accelerates after the 35th week.
Without adequate surfactant:
- Increased alveolar surface tension -> progressive atelectasis
- Infant must work as hard with every breath as the first
- Hypoxemia and CO2 retention develop
- Acidosis -> pulmonary vasoconstriction -> endothelial and epithelial damage
- Plasma proteins leak into alveoli -> fibrin-rich hyaline membranes form
- Hyaline membranes act as a barrier to gas exchange -> worsens hypoxemia -> further impairs surfactant synthesis (vicious cycle)
Morphology
- Lungs: normal size but heavy, airless, mottled purple
- Microscopically: collapsed (atelectatic) alveoli
- Early deaths: only necrotic debris in terminal bronchioles
- After several hours: eosinophilic hyaline membranes lining respiratory bronchioles, alveolar ducts, and alveoli - composed of necrotic type II pneumocytes + plasma proteins (mainly fibrin). Notably, minimal neutrophilic inflammation.
- With survival: reparative changes - type II pneumocyte proliferation and interstitial fibrosis
Clinical Features
- Grunting, tachypnea, nasal flaring, intercostal/subcostal retractions within minutes of birth
- Progressive worsening over the first 48-72 hours
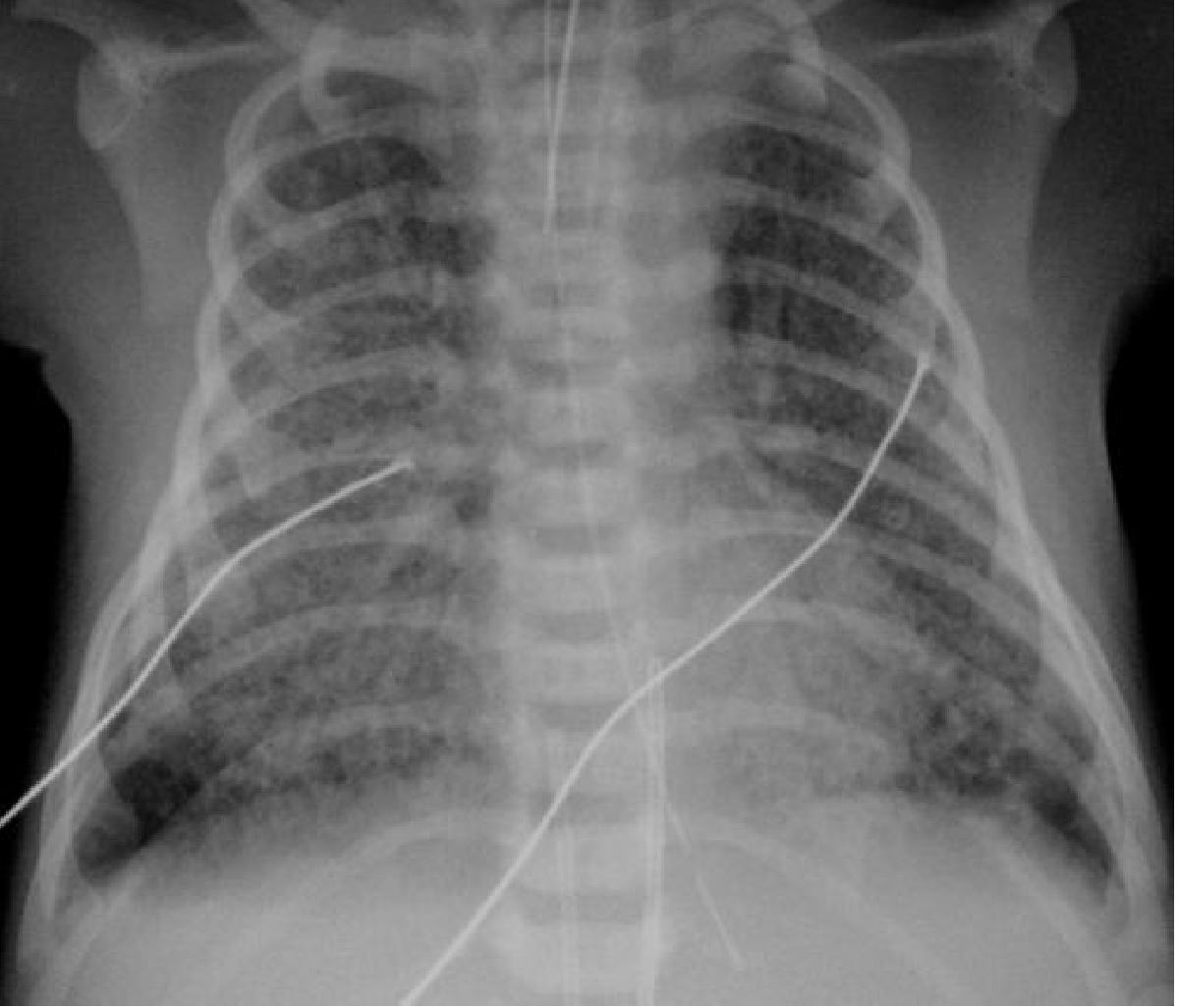
- CXR: diffuse "ground glass" appearance, air bronchograms, low lung volumes
Management
- Antenatal corticosteroids (betamethasone/dexamethasone) given to mothers at 24-34 weeks if preterm delivery anticipated - accelerate lung maturation
- Exogenous surfactant therapy (intratracheal) - standard of care; dramatically reduces mortality
- Respiratory support: CPAP, mechanical ventilation as needed
- Oxygen supplementation (target SpO2 90-95% in preterm to minimize retinopathy risk)
- Blended oxygen (30%) or room air recommended for initial resuscitation of preterm infants
Long-term Complications
- Bronchopulmonary dysplasia (BPD): chronic lung disease resulting from oxygen toxicity, barotrauma/volutrauma from ventilation, and inflammation. Diagnosed by need for supplemental O2 at 36 weeks' corrected gestational age. "New BPD" seen in extremely preterm (<1000 g) infants with large simplified alveolar structures and impaired capillary configuration.
- Retinopathy of prematurity: from oxygen exposure
- Both complications have decreased in incidence with modern management
2. Transient Tachypnea of the Newborn (TTN)
Etiology: Incomplete or delayed resorption of amniotic fluid from the lungs due to immaturity of respiratory epithelial Na+ transport.
Risk factors: Cesarean section (no "thoracic squeeze"), male sex, macrosomia, lower gestational age, maternal diabetes, maternal asthma, maternal smoking.
Clinical features:
- Symptoms within the first 6 hours, resolving within 72 hours (usually)
- Tachypnea >60 breaths/min, often 80-100 breaths/min
- Retractions, grunting, nasal flaring may be present; cyanosis/hypoxia are rare
- CXR: perihilar streaking, fluid in the interlobar fissure, congestion ("wet lung")
- Diagnosis of exclusion (rule out pneumonia, aspiration, congenital malformations, HIE, pneumothorax, acidosis, RDS)
Management:
- NPO with IV 10% dextrose for persistent tachypnea
- Supplemental oxygen and/or CPAP as indicated
- Diuretics and racemic epinephrine have no proven benefit
- Self-limiting; reassurance is key
3. Meconium Aspiration Syndrome (MAS)
Pathophysiology: Fetal hypoxia causes intestinal hyperperistalsis and passage of meconium into amniotic fluid. Meconium is then aspirated by the fetus (especially with gasping movements). Most common in post-mature infants (>42 weeks). Meconium causes:
- Mechanical obstruction - thick viscous material migrates to distal airways
- Ball-valve effect - partial obstruction causes alternating atelectasis and overinflation
- Chemical pneumonitis
- Alterations in pulmonary vasculature -> pulmonary arterial hypertension
Diagnosis: Infant born through meconium-stained amniotic fluid with respiratory symptoms that cannot otherwise be explained; meconium found below the level of the vocal cords.
CXR findings: Bilateral hyperinflation, asymmetric coarse opacification, small pleural effusions; air leaks (pneumothorax) are common.
Management:
- ~30% of affected infants require mechanical ventilation
- Inhaled nitric oxide for severe pulmonary hypertension
- ECMO (extracorporeal membrane oxygenation) for cases failing conventional therapy, using either veno-arterial (VA) or veno-venous (VV) approach
4. Neonatal Pneumonia
Acquisition:
- Transplacental (TORCH infections): toxoplasmosis, rubella, CMV, herpes - rare, seldom cause pulmonary abnormalities
- Perinatal: ascending vaginal infection, transvaginally during birth, or hospital-acquired (nosocomial)
- Most cases occur at birth via aspiration/swallowing of infected amniotic fluid or vaginal secretions
- Most common organism: Group B Streptococcus (GBS)
- Risk factor: prolonged rupture of membranes
CXR: Non-specific. Most common features in term infants presenting acutely within 24-48 hours: coarse bilateral asymmetrical alveolar opacification ± interstitial change. Radiographic changes may mimic MAS or severe TTN.
Management: IV antibiotics (ampicillin + gentamicin for empiric coverage of GBS and gram-negatives); respiratory support as needed.
5. Persistent Pulmonary Hypertension of the Newborn (PPHN)
Incidence: ~2/1000 live births in term and late preterm infants.
Pathophysiology: Failure of normal transition from high-resistance fetal circulation to low-resistance neonatal circulation. At delivery, pulmonary vascular resistance (PVR) should drop 8-10 fold. PPHN occurs when PVR remains high, causing right-to-left shunting through foramen ovale and ductus arteriosus -> refractory hypoxemia.
Etiologies:
- Idiopathic (abnormally remodeled pulmonary vasculature)
- Lung parenchymal disease (MAS, pneumonia/sepsis)
- Abnormal transition at birth (TTN, RDS, perinatal asphyxia)
- Congenital lung malformations (congenital diaphragmatic hernia, pulmonary hypoplasia)
Additional risk factors: maternal SSRIs/NSAIDs, maternal smoking, uncontrolled maternal diabetes.
Management:
- Treat underlying etiology
- Optimize oxygenation and ventilation (avoid overdistention; monitor preductal SpO2)
- Inhaled nitric oxide (iNO): best-studied agent; clear evidence in term and late preterm infants
- Adjuvant pulmonary vasodilators: sildenafil, bosentan, milrinone, prostacyclin (in selected cases)
6. Pneumothorax
- Occurs in 1-2% of normal newborns; higher with underlying RDS, MAS, or pneumonia
- Associated with use of high ventilatory pressures
- If tension pneumothorax suspected: needle thoracostomy and/or chest tube placement
- Monitor in NICU
7. Apnea of Prematurity
- Respiratory pause >20 seconds, or shorter pause with cyanosis, pallor, hypotonia, or bradycardia <100 bpm
- Types: central (no diaphragmatic activity), obstructive (upper airway), or mixed
- Occurs in most infants born at <28 weeks, ~20% at 34 weeks, <10% beyond 34 weeks
- Typically resolves by 34-36 weeks postmenstrual age
- Treatment: caffeine citrate (first line), CPAP, mechanical ventilation for severe cases
Summary of Key Points
- RDS (hyaline membrane disease) is the most common cause; fundamentally a surfactant deficiency disease of prematurity. Antenatal steroids and exogenous surfactant are the cornerstones of prevention/treatment.
- TTN is self-limiting (resolves within 72 hours) and is a diagnosis of exclusion.
- MAS carries risk of severe PPHN and may require iNO or ECMO.
- Neonatal pneumonia (most often GBS) radiographically mimics MAS and TTN.
- PPHN can complicate any of the above conditions and is treated with iNO.
- Long-term sequelae of prematurity and RDS management include BPD and retinopathy of prematurity, both reduced by modern ventilatory and oxygen management strategies.
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Creasy & Resnik's Maternal-Fetal Medicine; The Harriet Lane Handbook (Johns Hopkins Hospital); Grainger & Allison's Diagnostic Radiology
Birth aspixia en Newborn.
Finding Sources
Finding Sources
Searching PubMed
"birth asphyxia" OR "hypoxic ischemic encephalopathy" neonatal
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Now I have all the data needed for a comprehensive answer. Let me compile it.
Birth Asphyxia in the Newborn
Birth asphyxia (perinatal asphyxia) refers to impaired gas exchange around the time of delivery, resulting in hypoxemia, hypercapnia, and metabolic acidosis. When severe, it causes hypoxic-ischemic encephalopathy (HIE) - the primary neurological consequence. It affects approximately 1-6 per 1,000 live births, carries a 20% mortality rate in the newborn period, and leaves ~25% of survivors with permanent neurodevelopmental disability.
Definition & Causes
Birth asphyxia occurs when oxygen delivery to the fetus/newborn is interrupted. Common precipitants include:
- Cord prolapse or coiling of the umbilical cord around the neck
- Abruptio placentae or placenta previa
- Maternal hypotension or hemorrhage
- Prolonged or obstructed labor
- Uterine rupture
- Breech presentation, forceps delivery
- Maternal fever or infection
Note: Many infants with a complicated delivery have no brain damage, and many cases of cerebral palsy occur without any identifiable intrapartum event. Only ~5% of neonatal encephalopathy can be attributed to purely intrapartum factors - prenatal and multifactorial causes are far more common than historically assumed.
Pathophysiology
Asphyxia causes two phases of brain injury:
Phase 1 - Primary neuronal injury:
- Oxygen deprivation -> failure of Na+/K+-ATPase pumps -> cellular energy failure
- Glutamate release -> excitotoxicity -> neuronal depolarization
- Intracellular Ca²+ accumulation -> activation of destructive enzymes
- Immediate cell death (necrosis) in the most vulnerable regions
Phase 2 - Reperfusion injury (secondary energy failure, 6-24 hours later):
- Even after restoration of circulation, a second wave of neuronal death occurs
- Free radical generation, inflammatory cytokine release, mitochondrial dysfunction
- Apoptotic cell death ensues
- This latent phase is the therapeutic window for intervention (hypothermia acts here)
Brain regions most vulnerable:
- Term infant: deep grey matter (basal ganglia, thalamus), parasagittal cortex, hippocampus
- Preterm infant: periventricular white matter (periventricular leukomalacia)
Clinical Assessment
The Apgar Score
Assessed at 1, 5, and 10 minutes. Reflects heart rate, respiratory effort, muscle tone, reflex irritability, and color.
| Sign | 0 | 1 | 2 |
|---|---|---|---|
| Heart rate | Absent | <100 bpm | ≥100 bpm |
| Respirations | Absent | Slow, irregular | Good, crying |
| Muscle tone | Limp | Some flexion | Active, good flexion |
| Reflex irritability | No response | Grimace | Cough, sneeze |
| Color | Blue/pale | Pink body, blue extremities | Completely pink |
- 7-10: Normal
- 4-6: Moderate depression
- 0-3: Severe depression
A score of 0-3 at 5 minutes may correlate with neonatal death. However, a low Apgar score alone does NOT predict neurologic outcome or confirm that a hypoxic event occurred in utero - it is primarily a tool to guide resuscitative measures, not a diagnostic label.
Hypoxic-Ischemic Encephalopathy (HIE) - Staging (Sarnat Classification)
| Feature | Mild (Stage I) | Moderate (Stage II) | Severe (Stage III) |
|---|---|---|---|
| Level of consciousness | Hyperalert, irritable | Lethargic, obtunded | Stupor or coma |
| Muscle tone | Mild hypertonia | Hypotonia | Flaccid |
| Primitive reflexes | Exaggerated | Suppressed | Absent |
| Seizures | Rare | Common | Uncommon (EEG often silent) |
| Brain stem dysfunction | Rare | Rare | Common |
| Elevated ICP | Rare | Rare | Variable |
| Duration of symptoms | <24 hours | >24 hours (variable) | >5 days |
| Poor outcome | 0% | 20-40% | ~100% |
Mild HIE: Jittery baby, tremulousness, brisk reflexes, ankle clonus, soft fontanel; EEG normal. Recovery usually complete.
Moderate HIE: Lethargy, hypotonia, seizures at 48-72 hours, abnormal EEG with epileptiform activity/voltage suppression. Can improve or worsen. Unfavorable signs: abnormal visual and auditory evoked potentials.
Severe HIE: Stupor/coma from birth, irregular respirations requiring ventilation, seizures within 12 hours, hypotonia, absent Moro response, progressive loss of pupillary reactions. Very poor prognosis.
Diagnosis Criteria for Therapeutic Hypothermia
HIE is suspected and hypothermia initiated based on the following criteria (>35 weeks gestation):
-
Blood gas criteria: Cord gas or arterial blood gas in the first hour of life showing:
- pH <7.0 OR base deficit >16 mEq/L
-
If pH 7.01-7.15 or base deficit 10-15.9, additional criteria required:
- 10-minute Apgar score ≤5 OR
- Need for assisted ventilation at birth for ≥10 minutes AND
- Evidence of moderate to severe encephalopathy on clinical exam (Sarnat)
Neonatal Resuscitation (NRP Algorithm)
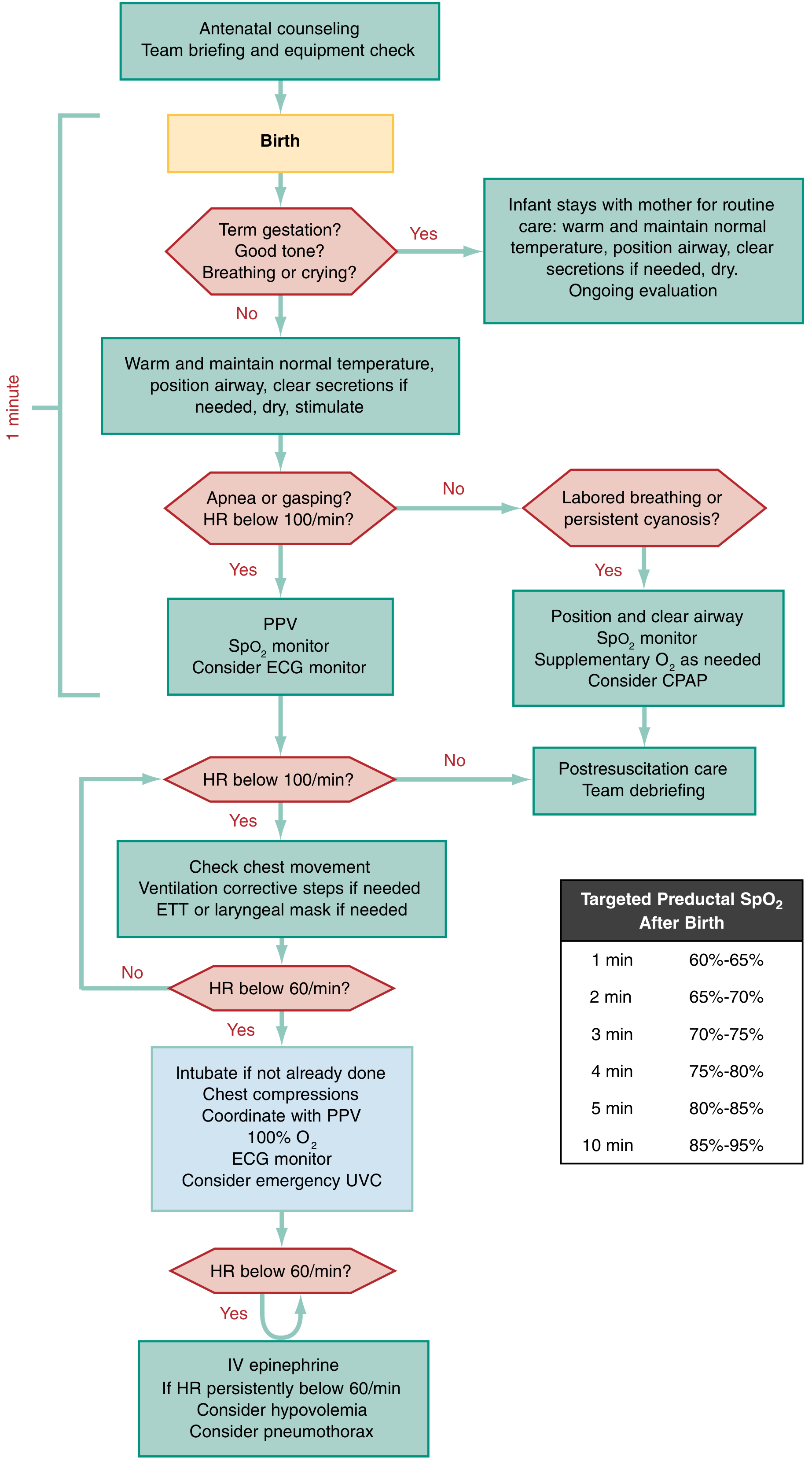
Key steps - all within the "Golden Minute":
- Warm, dry, stimulate (flick soles, rub back), position airway, clear secretions if needed
- If term gestation + good tone + breathing/crying → routine care with mother
- If apnea/gasping OR HR <100 bpm → PPV + SpO2 monitor + consider ECG
- If HR still <100 bpm → check chest movement, corrective ventilation steps, ETT or laryngeal mask
- If HR <60 bpm despite adequate ventilation → intubate, chest compressions (3:1 ratio), 100% O2, ECG monitor, emergency umbilical vein catheter (UVC)
- If HR persistently <60 bpm → IV epinephrine 0.01-0.03 mg/kg; consider hypovolemia (volume 10-20 mL/kg NS or PRBCs), consider pneumothorax
Targeted preductal SpO2 after birth (right hand/wrist):
| Time | Target SpO2 |
|---|---|
| 1 min | 60-65% |
| 2 min | 65-70% |
| 3 min | 70-75% |
| 4 min | 75-80% |
| 5 min | 80-85% |
| 10 min | 85-95% |
Important notes:
- Preterm resuscitation: start with blended 30% O2 (or room air), not 100% O2
- Avoid rapid volume infusion in preterm infants (risk of intraventricular hemorrhage)
- Skin color is a poor indicator of oxygenation in the first minutes of life - use pulse oximetry
Therapeutic Hypothermia (Cooling Therapy)
The only proven neuroprotective treatment for moderate-to-severe HIE.
- Target temperature: 33.5°C to 34.5°C (whole-body or selective head cooling)
- Must be initiated within 6 hours of birth (before secondary energy failure peaks)
- Duration: 72 hours, followed by slow rewarming over at least 4 hours
- Mechanism: reduces cerebral metabolic rate, limits excitotoxicity, free radical generation, and apoptosis during the latent phase
- Evidence: multiple RCTs (TOBY, CoolCap, NICHD, INFANT COOLING) confirm reduced mortality and improved neurologic outcome at 18 months
Risks of hypothermia: thrombocytopenia, hypotension, arrhythmia, coagulopathy
Infants not meeting criteria should not be cooled - passive cooling (avoid active warming) is appropriate until eligibility is confirmed. Transfer to a NICU with hypothermia capability is required.
Multi-organ Effects of Perinatal Asphyxia
Asphyxia is a systemic insult. Other organs affected:
| System | Manifestation |
|---|---|
| CNS | HIE, seizures, cerebral edema, IVH |
| Cardiovascular | Myocardial ischemia, tricuspid regurgitation, PPHN |
| Respiratory | PPHN, MAS, pulmonary hemorrhage |
| Renal | Acute tubular necrosis, oliguria (most common organ affected) |
| GI | NEC, hepatic injury |
| Metabolic | Hypoglycemia, hypocalcemia, hyponatremia, coagulopathy |
| Hematologic | Thrombocytopenia, DIC |
Long-term Sequelae
Survivors of moderate-to-severe HIE may develop:
- Cerebral palsy (spastic diplegia, spastic quadriplegia, extrapyramidal/athetoid forms)
- Epilepsy
- Cognitive delay and intellectual disability
- Hearing and visual impairment
- Microcephaly
MRI findings predictive of outcome:
- Periventricular leukomalacia (most common, 42%) - associated with spastic diplegia
- Basal ganglionic/thalamic injury (13%) - associated with extrapyramidal CP
- Cortical-subcortical lesions - associated with spastic quadriplegia
- Focal infarcts (7%) - associated with hemiplegia
Notably, the incidence of cerebral palsy in term infants has not decreased despite widespread fetal monitoring and increased cesarean rates - reinforcing that most CP has prenatal rather than intrapartum origins.
Recent Evidence
A 2025 systematic review (PMID 40319876) found dexmedetomidine to be a promising neuroprotective sedoanalgesic adjunct during therapeutic hypothermia. A 2025 review (PMID 39073530) highlighted emerging therapies targeting HIE pathways including melatonin, erythropoietin, and stem cell therapy, currently under investigation.
Sources: Adams and Victor's Principles of Neurology, 12th ed.; The Harriet Lane Handbook, 23rd ed. (Johns Hopkins); Rosen's Emergency Medicine, 9th ed.; Textbook of Family Medicine, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.