easy ans format can form flow chart for easy understanding Describe the etiology and risk factors of Renal cell carcinoma Explain the histopathological features of renal cell carcinoma Discuss the clinical presentation of renal cell carcinoma Outline the diagnostic modalities used in Renal cell carcinom Evaluate the treatment options for renal cell carcinoma Discuss the prognosis and long-term outcome of Renal cell carcinoma
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have rich, comprehensive content from authoritative textbooks. Let me compile this into a detailed, well-organized flowchart-style response covering all six topics.
🔵 RENAL CELL CARCINOMA (RCC) - Complete Overview
Sources: Campbell-Walsh-Wein Urology (9780323546423), Robbins & Kumar Basic Pathology (9780323790185), NKF Primer on Kidney Diseases (9780323791229)
📌 MASTER FLOWCHART
╔══════════════════════════════════════════════════════════════════╗
║ RENAL CELL CARCINOMA (RCC) ║
╚══════════════════════════════════════════════════════════════════╝
│
├──► 1. ETIOLOGY & RISK FACTORS
│
├──► 2. HISTOPATHOLOGICAL FEATURES
│
├──► 3. CLINICAL PRESENTATION
│
├──► 4. DIAGNOSTIC MODALITIES
│
├──► 5. TREATMENT OPTIONS
│
└──► 6. PROGNOSIS & LONG-TERM OUTCOMES
🔴 1. ETIOLOGY & RISK FACTORS
RISK FACTORS FOR RCC
│
├── MODIFIABLE
│ ├── Cigarette Smoking ──────► Doubles risk; dose-dependent
│ ├── Obesity (BMI > 30) ─────► Increases risk (adipokines, sex hormones)
│ ├── Hypertension ───────────► Independent risk factor
│ ├── Cadmium/asbestos exposure (occupational)
│ └── Dialysis-associated polycystic kidney disease ──► 30× increased risk
│
├── NON-MODIFIABLE
│ ├── Age: Peak 55-75 years
│ ├── Sex: Male:Female = 1.9:1
│ ├── Race: Higher in African-Americans (+5-10%); lower in Asians (-50%)
│ └── Familial/Hereditary (4-6% of cases)
│
└── HEREDITARY SYNDROMES
├── Von Hippel-Lindau (VHL) disease ──► Bilateral clear cell RCC in 40-60%
│ └── Autosomal dominant; VHL gene mutation on chromosome 3p25
├── Hereditary Papillary RCC ──────────► MET gene mutation (chr 7q)
├── Birt-Hogg-Dubé syndrome ───────────► FLCN gene; chromophobe RCC
└── Hereditary Leiomyomatosis RCC ─────► FH gene mutation
Key Molecular Mechanism:
- VHL gene loss → HIF accumulates → VEGF overexpression → tumor angiogenesis
- This is the main driver of clear cell RCC (most common subtype)
- Campbell-Walsh-Wein Urology, p. 2846-2848; Robbins & Kumar Basic Pathology, p. 531
🟠 2. HISTOPATHOLOGICAL FEATURES
RCC SUBTYPES (Based on WHO Classification)
│
├── CLEAR CELL RCC ──────────────────────────────── 65% of cases
│ ├── Origin: Proximal convoluted tubule
│ ├── Molecular: VHL gene loss (chr 3p25); HIF pathway activation
│ ├── Macro: Golden-yellow tumor (lipid-rich cells); hemorrhage & necrosis
│ ├── Micro: Cells with CLEAR cytoplasm (glycogen + lipid)
│ │ Arranged in nests/alveoli; delicate vascular network
│ ├── Grading: Fuhrman/ISUP nuclear grade I-IV
│ └── Behavior: Most aggressive; metastasizes to lung, liver, bone, brain
│
├── PAPILLARY RCC ───────────────────────────────── 10-15% of cases
│ ├── Origin: Distal tubule
│ ├── Molecular: MET gene activation (chr 7q); trisomy 7 and 17
│ ├── Macro: Bilateral/multifocal; yellow-orange; hemorrhage/necrosis
│ ├── Micro: Papillary structures with fibrovascular cores
│ │ Type 1 (low grade): small cells, pale cytoplasm
│ │ Type 2 (high grade): large cells, eosinophilic cytoplasm
│ └── Behavior: Better prognosis than clear cell
│
├── CHROMOPHOBE RCC ─────────────────────────────── 5% of cases
│ ├── Origin: Cortical collecting duct
│ ├── Molecular: Loss of multiple chromosomes (1,2,6,10,13,17,21)
│ ├── Macro: Well-circumscribed; pale tan/beige
│ ├── Micro: Large cells with PALE, fine-reticular cytoplasm
│ │ "Plant cell" appearance; prominent cell membranes
│ │ Hale's colloidal iron stain POSITIVE
│ └── Behavior: Best prognosis among all subtypes
│
├── COLLECTING DUCT (BELLINI) RCC ──────────────── <1% of cases
│ └── Very aggressive; tubular/papillary pattern; desmoplastic stroma
│
└── UNCLASSIFIED RCC ──────────────────────────── 1-5%
└── Aggressive; often sarcomatoid differentiation; poor prognosis
Sarcomatoid Differentiation:
- Can occur in ANY subtype
- Indicates high-grade transformation
- Associated with very poor prognosis
- Robbins & Kumar Basic Pathology, p. 531-532; Campbell-Walsh-Wein Urology, p. 2856-2860
🟡 3. CLINICAL PRESENTATION
CLINICAL PRESENTATION OF RCC
│
├── INCIDENTAL (>60% today)
│ └── Found on CT/US done for unrelated reason
│ ├── Usually organ-confined
│ └── Better prognosis
│
├── CLASSIC TRIAD ("Too Late Triad") ── now seen in <10%
│ ├── Flank pain
│ ├── Gross hematuria
│ └── Palpable abdominal mass
│ → Almost always indicates ADVANCED disease
│
├── SIGNS OF LOCAL/REGIONAL DISEASE
│ ├── Hematuria (most common symptom)
│ ├── Flank pain (hemorrhage into tumor or clot obstruction)
│ ├── Non-reducing varicocele (esp. right-sided) ── venous invasion
│ ├── Bilateral lower limb edema ─── IVC obstruction
│ └── Perinephric hematoma (spontaneous)
│
├── SIGNS OF SYSTEMIC/METASTATIC DISEASE
│ ├── Bone pain (skeletal metastases)
│ ├── Persistent cough (pulmonary metastases - most common site)
│ ├── Cervical lymphadenopathy
│ └── Constitutional: weight loss, fever, night sweats
│
└── PARANEOPLASTIC SYNDROMES (unique to RCC)
├── Stauffer syndrome ─── Non-metastatic hepatic dysfunction
├── Hypercalcemia ──────── PTHrP secretion (~10-20%)
├── Polycythemia ──────────Ectopic EPO secretion
├── Hypertension ──────────Ectopic renin production
├── Cushing syndrome ──────Ectopic ACTH
└── Anemia of chronic disease
- Campbell-Walsh-Wein Urology, p. 2863-2864
🟢 4. DIAGNOSTIC MODALITIES
DIAGNOSIS OF RCC
│
├── STEP 1: INITIAL WORKUP
│ ├── Urinalysis (hematuria)
│ ├── CBC, BMP, LFTs, Serum calcium
│ ├── LDH, alkaline phosphatase, ESR, CRP
│ └── Urine cytology (if urothelial Ca suspected)
│
├── STEP 2: IMAGING
│ │
│ ├── ULTRASOUND (First-line screening)
│ │ ├── Distinguishes solid vs cystic mass
│ │ ├── Low sensitivity for small tumors
│ │ └── CEUS: avid early enhancement + early washout in clear cell
│ │
│ ├── CT SCAN (Gold Standard)
│ │ ├── Multiphasic contrast CT (corticomedullary + nephrographic phases)
│ │ ├── Clear cell: avid enhancement in corticomedullary phase
│ │ │ then hypoenhancing in nephrographic phase
│ │ ├── Papillary: hypoenhancing on ALL phases; hypointense on T2
│ │ ├── Chromophobe: avid enhancement (less than clear cell)
│ │ └── Also evaluates vascular extension, lymph nodes, staging
│ │
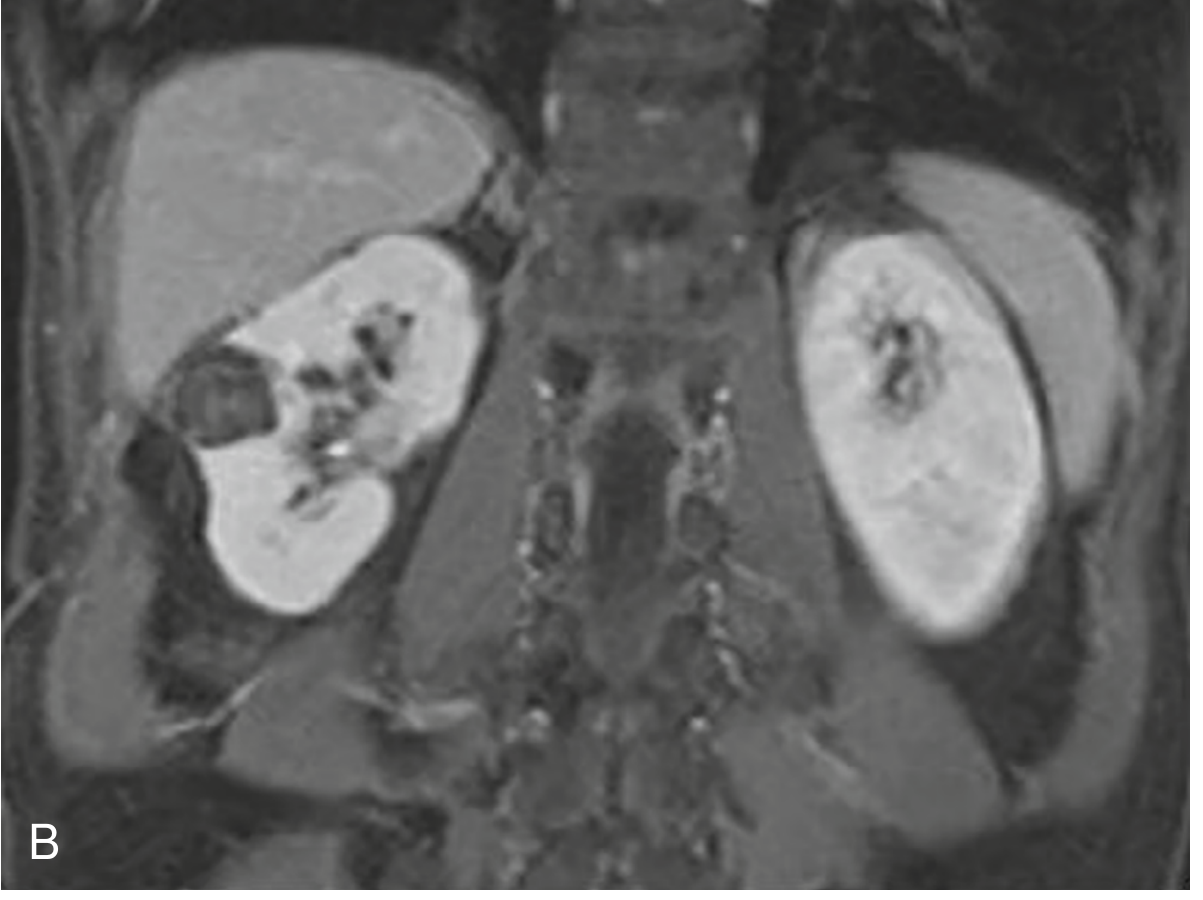
│ ├── MRI
│ │ ├── Equivalent to CT for characterization
│ │ ├── Superior for: IVC thrombus extent, cystic masses
│ │ ├── Better detection of complex cyst features (subtraction imaging)
│ │ └── Preferred if contrast allergy or renal impairment
│ │
│ └── BOSNIAK CLASSIFICATION (Cystic masses)
│ ├── Category I/II → Benign (follow-up only)
│ ├── Category IIF → Follow-up with repeat imaging
│ ├── Category III → Indeterminate; surgical excision recommended
│ └── Category IV → Clearly malignant → Surgery
│
├── STEP 3: BIOPSY (Selected cases)
│ ├── CT/US-guided renal mass biopsy
│ ├── Indicated when: ablative therapy planned, metastatic workup,
│ │ lymphoma/mets suspected, small indeterminate masses
│ └── NOT mandatory before surgical resection in classic cases
│
└── STEP 4: STAGING WORKUP
├── CT chest/abdomen/pelvis (for metastases)
├── Bone scan (only if bone pain or elevated ALP)
├── Brain MRI (only if neurologic symptoms)
└── TNM STAGING (AJCC 8th Ed)
├── T1a: ≤4 cm, confined to kidney
├── T1b: 4-7 cm, confined to kidney
├── T2a: 7-10 cm, confined to kidney
├── T2b: >10 cm, confined to kidney
├── T3a: Renal vein/perinephric fat invasion
├── T3b: IVC below diaphragm
├── T3c: IVC above diaphragm / pericardium
├── T4: Beyond Gerota's fascia / adrenal invasion
├── N1: Regional lymph node metastasis
└── M1: Distant metastasis
- NKF Primer on Kidney Diseases, p. 78; Campbell-Walsh-Wein Urology, p. 2864-2868
🔵 5. TREATMENT OPTIONS
TREATMENT OF RCC
│
├── LOCALIZED DISEASE (T1-T2, N0, M0)
│ │
│ ├── ACTIVE SURVEILLANCE
│ │ └── Small masses (<2 cm), elderly/comorbid patients
│ │ Growth rate ~0.3 cm/year; low metastatic potential if small
│ │
│ ├── SURGICAL (Preferred for fit patients)
│ │ │
│ │ ├── PARTIAL NEPHRECTOMY (PN) ── PREFERRED for T1
│ │ │ ├── Nephron-sparing; equivalent cancer control to radical
│ │ │ ├── Open / Laparoscopic / Robot-assisted
│ │ │ └── Absolute indications: bilateral RCC, solitary kidney
│ │ │ Elective indication: <4 cm tumor, normal contralateral kidney
│ │ │
│ │ └── RADICAL NEPHRECTOMY (RN)
│ │ ├── Removal of kidney + Gerota's fascia ± adrenal ± LN
│ │ ├── Laparoscopic RN = Gold standard for T2 tumors
│ │ └── Indicated: large tumors, central location, not amenable to PN
│ │
│ └── ABLATIVE THERAPIES
│ ├── Radiofrequency Ablation (RFA) ── <3 cm masses
│ ├── Cryoablation ─── <3 cm masses; percutaneous or laparoscopic
│ └── Suitable for elderly/high-surgical-risk patients
│
├── LOCALLY ADVANCED DISEASE (T3-T4 or N1)
│ ├── Radical nephrectomy + IVC thrombectomy (T3b/c)
│ ├── Lymphadenectomy (therapeutic + staging)
│ └── Adjuvant pembrolizumab ── After nephrectomy (high-risk clear cell)
│
└── METASTATIC RCC (mRCC)
│
├── CYTOREDUCTIVE NEPHRECTOMY
│ └── Selected patients with good PS + limited mets
│
├── TARGETED THERAPY (VEGF/mTOR pathway)
│ ├── VEGF-TKIs (first-line):
│ │ ├── Sunitinib
│ │ ├── Pazopanib
│ │ ├── Cabozantinib (also inhibits MET + AXL)
│ │ └── Axitinib (2nd line)
│ ├── mTOR inhibitors:
│ │ ├── Temsirolimus (poor-risk)
│ │ └── Everolimus (2nd line)
│ └── Bevacizumab + IFN-α (anti-VEGF monoclonal antibody)
│
└── IMMUNOTHERAPY (Checkpoint Inhibitors)
├── Nivolumab (anti-PD-1) ─── 2nd line
├── Nivolumab + Ipilimumab ── 1st line (intermediate/poor-risk)
├── Pembrolizumab + Axitinib ─ 1st line
└── Avelumab + Axitinib ────── 1st line (favorable-risk)
MECHANISM OF CHECKPOINT INHIBITORS:
APC ──► MHC/Antigen ──► TCR → T-cell ACTIVATED
B7 ──────────────────► CD28 → Co-stimulation
B7 ──────────────────► CTLA-4 → INHIBITS T-cell (tumor escape)
PD-L1 (on tumor) ────► PD-1 → INHIBITS T-cell (tumor escape)
Nivolumab blocks PD-1; Ipilimumab blocks CTLA-4 → Restores anti-tumor immunity
- Campbell-Walsh-Wein Urology, p. 2854, 2874-2878
🟣 6. PROGNOSIS & LONG-TERM OUTCOMES
PROGNOSTIC FACTORS IN RCC
│
├── GOOD PROGNOSIS INDICATORS
│ ├── Organ-confined disease (T1/T2)
│ ├── Small tumor size
│ ├── Low nuclear grade (Fuhrman/ISUP Grade 1-2)
│ ├── Chromophobe or papillary subtype
│ ├── Incidental detection
│ └── Complete surgical resection (negative margins)
│
└── POOR PROGNOSIS INDICATORS
├── CLINICAL: Poor PS, systemic symptoms, anemia, hypercalcemia,
│ elevated LDH/ESR/CRP/ALP, thrombocytosis
├── ANATOMIC: Large tumor, venous invasion, organ extension,
│ lymph node metastases, distant metastases (M1)
└── HISTOLOGIC: High nuclear grade, sarcomatoid features,
tumor necrosis, vascular invasion,
perinephric/renal sinus fat invasion,
positive surgical margins
5-YEAR SURVIVAL BY STAGE:
┌────────────────────────────────────────────┐
│ Stage I (T1, N0, M0) ──────► ~95% │
│ Stage II (T2, N0, M0) ──────► ~75-80% │
│ Stage III (T3 or N1) ──────► ~50-60% │
│ Stage IV (T4 or M1) ──────► ~10-20% │
└────────────────────────────────────────────┘
LONG-TERM CONSIDERATIONS:
│
├── SURVEILLANCE AFTER TREATMENT
│ ├── Physical exam + history (every visit)
│ ├── Labs: BUN/Cr, eGFR, urinalysis, CBC, LDH, LFTs, Ca
│ ├── CT chest/abdomen/pelvis (interval depends on stage)
│ └── Bone scan: only if symptoms or elevated ALP
│
├── RENAL FUNCTION MONITORING
│ └── Partial nephrectomy preferred to preserve nephrons
│ PN = equal cancer control + better long-term renal function
│
├── METASTATIC DISEASE OUTCOMES
│ ├── Median OS with modern immunotherapy: ~28-38 months
│ ├── Complete responses possible with IO combinations (~10-16%)
│ └── Selected patients achieve long-term remission
│
└── INTEGRATED PROGNOSTIC MODELS
├── MOTZER (MSKCC) Risk Score
│ Factors: KPS <80%, Hgb <LLN, Ca >ULN, LDH >1.5×ULN,
│ no prior nephrectomy
│ → Favorable / Intermediate / Poor risk groups
└── SSIGN Score (Mayo Clinic)
Factors: Stage, Size, Grade, Necrosis
→ Predicts cancer-specific survival
📋 QUICK SUMMARY TABLE
| Topic | Key Points |
|---|---|
| Etiology | Smoking, obesity, HTN, VHL disease, dialysis |
| Most Common Type | Clear cell RCC (65%); VHL/HIF/VEGF pathway |
| Classic Triad | Hematuria + Flank pain + Mass (= "Too Late Triad") |
| Incidental detection | >60% cases today (CT/US) |
| Gold Standard Imaging | Multiphasic contrast CT |
| Localized Treatment | Partial or radical nephrectomy |
| Metastatic 1st line | Nivo + Ipi OR Pembrolizumab + Axitinib |
| Best prognosis subtype | Chromophobe > Papillary > Clear cell |
| Stage I 5-yr survival | ~95% |
| Stage IV 5-yr survival | ~10-20% |
Sources:
- Campbell-Walsh-Wein Urology 3-Volume Set, pp. 2846-2890
- Robbins & Kumar Basic Pathology, pp. 531-533
- NKF Primer on Kidney Diseases, 8th ed., p. 78
This is a shared conversation. Sign in to Orris to start your own chat.