Make me understand Carpal tunnel syndrome
"carpal tunnel syndrome"[MeSH Terms] AND treatment
carpal tunnel syndrome pathophysiology diagnosis treatment 2025
Carpal Tunnel Syndrome (CTS) - A Complete Overview
What Is It?
Anatomy of the Carpal Tunnel
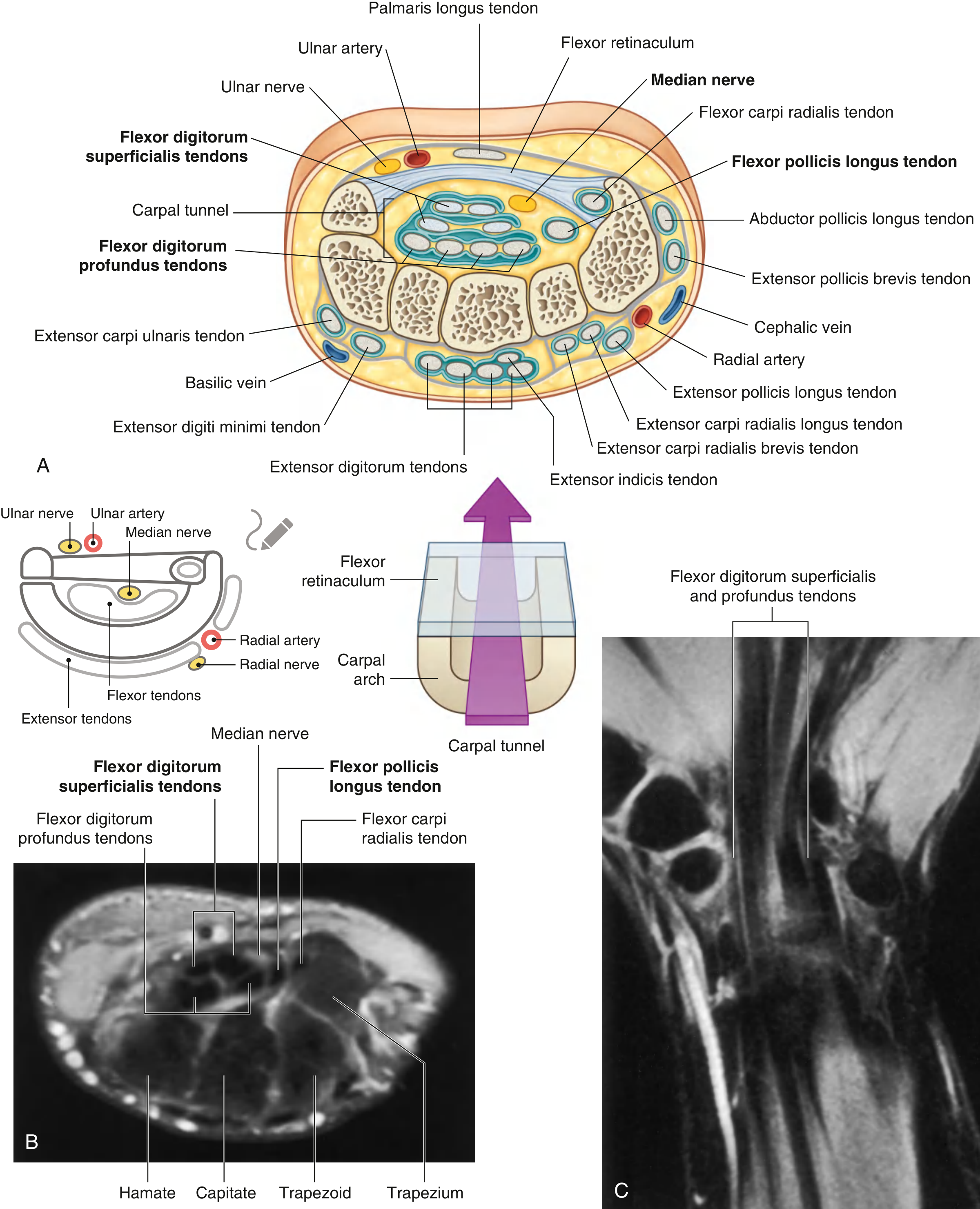
- Floor and walls: Carpal bones (scaphoid, trapezium laterally; hamate, pisiform medially) form a dorsal arch
- Roof: The flexor retinaculum (transverse carpal ligament - TCL)
- Contents: The median nerve (lying most palmarly/superficially) + 9 flexor tendons (4 from flexor digitorum superficialis, 4 from flexor digitorum profundus, and 1 flexor pollicis longus)
Gray's Anatomy for Students, p. 920
Pathophysiology
- Tunnel pressures exceeding 20-30 mmHg impede epineurial blood flow
- This causes venous congestion → nerve edema and anoxic damage to capillary endothelium
- Sustained compression leads to progressive demyelination, then axonal damage
- Most cases are idiopathic (no clear cause can be found), but many risk factors are known
Campbell's Operative Orthopaedics 15th Ed, p. 4502; Gray's Anatomy for Students, p. 920
Risk Factors and Causes
| Category | Examples |
|---|---|
| Patient factors | Female sex, obesity, physical inactivity, smoking |
| Decreased tunnel size | Bony abnormalities, acromegaly, wrist flexion/extension |
| Increased tunnel contents | Colles fracture, scaphoid fracture, lunate dislocation |
| Synovial/soft tissue | Rheumatoid arthritis, tenosynovitis, synovial cysts |
| Metabolic/systemic | Hypothyroidism (myxedema), diabetes, amyloidosis, gout |
| Fluid retention | Pregnancy (usually resolves post-delivery), congestive heart failure |
| Occupational | Repetitive wrist/finger motion (controversial - difficult to substantiate directly) |
Campbell's Operative Orthopaedics 15th Ed (Box 82.1); Goldman-Cecil Medicine; Firestein & Kelley's Rheumatology
Clinical Features
Symptoms (in order of typical progression):
- Nocturnal paresthesias - the hallmark symptom. Tingling, burning, or "pins and needles" in the first 3 fingers, classically waking the patient at night
- Daytime symptoms - provoked by sustained wrist positions (driving, reading, phone use)
- "Flick sign" - patients shake or flick the hand to relieve symptoms
- Pain - may radiate up the forearm to the elbow and even shoulder (poorly localized, aching)
- Weakness and clumsiness - difficulty with fine motor tasks, grip weakness
- Objective sensory loss - numbness in the thumb, index, middle, and radial half of ring finger (median nerve distribution)
- Thenar atrophy - wasting of the thenar eminence (abductor pollicis brevis); a late sign indicating severe compression
Firestein & Kelley's Rheumatology, p. 6719; Goldman-Cecil Medicine
Diagnosis
Clinical Diagnosis
- Nocturnal paresthesias in median nerve territory
- Paresthesias/hypoesthesia of thumb, index, and middle fingers
- Weakness/clumsiness of hand
Physical Examination - Provocative Tests
| Test | How performed | Finding | Sensitivity / Specificity |
|---|---|---|---|
| Phalen's test | Sustained wrist flexion for 60 seconds | Reproduction of tingling | Most sensitive |
| Tinel's sign | Gentle percussion over flexor retinaculum at wrist | Radiating paresthesia in median distribution | Most specific, least sensitive |
| Durkan test (Carpal Compression Test) | Direct thumb/manometer pressure over tunnel for 30 seconds | Symptom reproduction | ~87% sensitive, 90% specific - better than both above |
| CTS-6 Score | Combined history + exam scoring tool | Score ≥12 = high probability | 95% sensitive, 91% specific |
Electrodiagnostic Studies (Nerve Conduction Studies / EMG)
- Prolonged distal sensory latency >3.5 ms - most sensitive early finding
- Prolonged distal motor latency >4.5 ms
- EMG may show fibrillations, positive sharp waves, reduced motor recruitment
- NCS: ~90% sensitive, ~60% specific
- Note: studies can be normal even with clear CTS symptoms, and abnormal in asymptomatic patients
Campbell's Operative Orthopaedics 15th Ed, p. 4503
Ultrasound
Differential Diagnosis
- Cervical disc disease / radiculopathy (C6-C7) - check for neck pain, reflexes
- Thoracic outlet syndrome - proximal compression
- Pronator teres syndrome - more proximal median nerve entrapment (no nocturnal symptoms)
- Peripheral neuropathy (diabetic, alcoholic) - bilateral, stocking-glove pattern
- De Quervain tenosynovitis - radial-sided pain, no paresthesias
- Raynaud's phenomenon - color changes, cold triggers
Treatment
Conservative (Non-Surgical)

- Short-term effectiveness is good
- Long-term efficacy is mixed
- Risk of permanent median nerve injury if performed incorrectly
- Best reserved for: temporary conditions (pregnancy), patients unfit for surgery, or bridging until surgery
Firestein & Kelley's Rheumatology, p. 6771; Goldman-Cecil Medicine
Surgical Treatment
- Failure of conservative treatment after adequate trial
- Late findings: objective sensory loss or thenar atrophy (these should prompt early surgery)
- Severe or rapidly progressive symptoms
| Approach | Description | Advantages |
|---|---|---|
| Open CTR | Direct visualization through palmar incision | Gold standard; reliable |
| Endoscopic CTR | Camera-guided release through smaller portal | Faster return to work, less scar tenderness - generally preferred per Goldman-Cecil |
Campbell's Operative Orthopaedics 15th Ed; Firestein & Kelley's Rheumatology, p. 6785-6787
Special Populations
- Pregnancy: CTS is common due to fluid retention; usually resolves after delivery. Corticosteroid injection can bridge until delivery if needed.
- Children: Very rare; consider congenital bone abnormalities, hypothyroidism, or lysosomal storage disease.
- Rheumatoid arthritis: Tenosynovitis is a common cause; treat the underlying condition alongside local CTS therapy.
- Diabetes: Peripheral neuropathy can overlap; electrodiagnostics are particularly important here.
Summary Flow
Nocturnal hand tingling / paresthesias
↓
Clinical exam: Phalen's, Tinel's, Durkan's tests
↓
Mild-moderate? → Conservative: Splint + NSAIDs ± steroid injection
↓
No improvement or severe / thenar atrophy?
↓
Nerve Conduction Studies (confirm + grade severity)
↓
Carpal Tunnel Release (open or endoscopic)
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 4502-4503 (Box 82.1, 82.2)
- Firestein & Kelley's Textbook of Rheumatology, p. 6719-6787
- Goldman-Cecil Medicine, p. 4088
- Gray's Anatomy for Students, p. 920
- Recent evidence: PMID 39894044 (hydrodissection, 2025); PMID 40315975 (conservative treatments NMA, 2025)
My one friend is female her age 21 wt 42 kg , height 5.5
My one friend is female her age 21 wt 42 kg , height 5.5 I want to give her suggestions for betterment of her health so that she can be healthy.
underweight young woman BMI 15 health risks nutrition recommendations 2024
https://my.clevelandclinic.org/health/diseases/underweight
Health Assessment & Suggestions for Your Friend
Her Numbers at a Glance
| Parameter | Value |
|---|---|
| Age | 21 years |
| Sex | Female |
| Height | 5.5 ft = 167.6 cm |
| Weight | 42 kg |
| BMI | 42 ÷ (1.676)² = ~15.0 |
| BMI Category | 🔴 Severely Underweight |
| Range | Category |
|---|---|
| Below 16 | Severely underweight |
| 16 - 18.4 | Underweight |
| 18.5 - 24.9 | Normal / Healthy |
| 25 - 29.9 | Overweight |
⚠️ Why This Matters - Health Risks of Being This Underweight
1. Bone Problems
- Low bone mineral density and risk of early osteoporosis - 24% of underweight women have low BMD vs. only 9% in normal-weight women
- Stress fractures from minor injuries
2. Hormonal & Reproductive Issues
- Missed or irregular periods (amenorrhea) - very common at this weight
- Lack of ovulation (anovulatory cycles), which can affect future fertility
- Low estrogen levels
3. Immune System Weakness
- Gets sick more often, takes longer to recover
- Poor wound healing
4. Nutritional Deficiencies
- Iron deficiency anemia - fatigue, pale skin, breathlessness
- Vitamin D & Calcium deficiency - weakens bones
- B12 and folate deficiency - affects brain and nerves
- Protein deficiency - causes muscle loss and hair thinning
5. Physical Symptoms She May Already Notice
- Constant tiredness / low energy
- Hair thinning or hair fall
- Dry skin
- Dizziness on standing up
- Feeling cold easily
- Difficulty concentrating
6. Mental Health Connection
- Irritability, mood changes, depression can accompany low body weight
- Important to gently check if disordered eating or body image issues are involved
What Should She Do? - Practical Suggestions
Step 1: See a Doctor First
- Check for an underlying cause (thyroid issues, digestive problems, chronic illness)
- Run blood tests: CBC, iron, B12, Vitamin D, thyroid function, calcium
- Rule out eating disorders
Step 2: Gradual, Healthy Weight Gain Through Diet
| Food Group | Examples | Why |
|---|---|---|
| Protein | Eggs, paneer, dal, chicken, fish, milk, curd | Builds muscle, repairs tissue |
| Healthy fats | Nuts, peanut butter, ghee, avocado, seeds | Calorie-dense, good for hormones |
| Complex carbs | Rice, roti, oats, banana, sweet potato | Sustained energy |
| Dairy | Milk (whole), yogurt, cheese | Calcium + protein + calories |
| Fruits & vegetables | All types, especially iron-rich spinach | Micronutrients, immunity |
- Eat 5-6 small meals per day instead of 3 large ones (easier to eat more)
- Add a calorie-dense snack before bed (e.g., banana with peanut butter, a glass of whole milk)
- Never skip breakfast
- Avoid filling up on water/tea right before meals
Step 3: Supplements to Consider (After Doctor Advice)
| Supplement | Reason |
|---|---|
| Iron + Vitamin C | If anemia is found |
| Vitamin D3 (1000-2000 IU/day) | Bone health - very commonly deficient |
| Calcium (500-1000 mg/day) | Bone density |
| B-complex | Energy, nerve health |
| Multivitamin | General nutritional support |
Do not self-prescribe supplements - a simple blood test will show exactly what is deficient.
Step 4: Light Exercise - Build Muscle, Not Just Fat
- Strength / resistance training 2-3 times per week - builds lean muscle mass which is healthy weight gain
- Avoid excessive cardio (running, cycling for long durations) as it burns precious calories
- Yoga is good for stress, flexibility, and body awareness
Step 5: Sleep & Stress
- Aim for 7-9 hours of sleep - growth hormone is released during sleep and is key for weight gain
- Chronic stress elevates cortisol which suppresses appetite and causes weight loss
- Relaxation practices (deep breathing, light yoga, walks in nature) can help
Step 6: Be a Good Friend
- Do NOT comment repeatedly on her weight or appearance - this can increase anxiety
- Encourage her to see a doctor by framing it as "getting a routine checkup"
- If you suspect she may be restricting food intentionally (disordered eating), approach with kindness and suggest professional help - a counselor or doctor
Summary
Your friend's BMI of ~15 is in the severely underweight range and needs attention. The good news is that with proper nutrition, rest, light exercise, and medical support, this is very manageable. The goal is gradual, sustainable weight gain through whole foods, not crash diets or supplements alone.
My one friend is female her age 21 wt 42 kg , height 5.5My one friend is female her age 21 wt 42 kg , height 5.5 I want to give her suggestions for betterment of her health so that she can be healthy. Her urine output increases when she drinks tea but no sugar no kidney issue just normal .. I want to make her impress so that she have some feelings by my intense care for her
About the Urine Output When She Drinks Tea
- Regular tea / green tea / black tea
- Coffee
- Energy drinks
- Even some sodas
About Impressing Her With Your Care 😊
Health-Focused Care Gestures
- Share a healthy homemade meal or snack with her (peanut butter banana, dry fruits, nuts)
- Gently suggest a morning walk together - fresh air + company goes a long way
- If she complains of tiredness or hair fall, you can now knowledgeably say "you should get your iron and Vitamin D checked" - that shows real attentiveness
- Remind her to drink water, not just tea
Emotional Gestures That Actually Work
- Listen more than you advise - people feel cared for when they feel heard
- Remember small things she tells you and bring them up later
- Be consistent - show up, check in, be reliable
- Be genuine - people sense when concern is real vs. performed
One Honest Note
How to suggest her as her BMI is less
How to Suggest Her About Low BMI - The Right Way
❌ What NOT to Say
- "You're too thin / you look weak"
- "You need to eat more, you're underweight"
- "Your BMI is only 15, that's dangerous"
- "Why don't you eat properly?"
✅ The Right Approach - Step by Step
"I've noticed you seem a bit tired lately - are you sleeping okay? Eating well?"
"I read something interesting about energy levels and nutrition - it made me think of you."
"I've been trying to eat better lately - more protein, iron-rich foods. Want to try something healthy together sometime?"
"I calculated my BMI out of curiosity - what's yours? Mine came out at X..."
"I read that many young women have low Vitamin D and iron without even knowing - it causes hair fall and tiredness. Maybe we should both get a basic blood test done?"
- Bring her healthy, calorie-rich snacks casually - "I made too many nuts and dry fruits, want some?"
- Suggest eating together - "Let's try that new place, I heard they have amazing food"
- Cook or share something nourishing - banana shake, peanut butter toast, almond milk
"You know, I was reading about this - it could be iron or Vitamin D deficiency. At your height and weight, your body might need more fuel. A doctor visit + simple blood test could tell everything. I can come with you if you want."
The Golden Script (If You Want One)
"Hey, I genuinely care about you and I've been a little worried. You sometimes look tired and I just want to make sure you're doing okay. Not about looks at all - just health and energy. Would you be open to getting a basic health checkup together? I'll go with you."
Summary Table
| Situation | What to Say |
|---|---|
| She's always tired | "You seem low on energy lately - are you eating enough?" |
| Hair fall mentioned | "That can be iron or Vitamin D - a blood test will tell" |
| Casual conversation | "I calculated my BMI, what's yours?" |
| Offering food | "Here, I got too many dry fruits, have some!" |
| Direct moment | "I care about you - let's get a checkup together" |
Make her feel cared for, not criticized. Invite her into the conversation, don't push her into it.
Generate a healthy meal plan for gradual weight gain
Her Daily Calorie Target
| Current estimated intake | ~1,200 - 1,400 kcal (typical for underweight) |
|---|---|
| Target intake | 2,000 - 2,200 kcal/day |
| Protein goal | 60 - 70 g/day |
| Meal frequency | 5 - 6 times/day |
🗓️ Full Week Meal Plan
📅 DAY 1 (Monday)
| Time | Meal | Items | ~Kcal |
|---|---|---|---|
| 7:30 AM | Breakfast | 2 boiled eggs + 2 whole wheat toast + 1 banana + 1 glass whole milk | 520 |
| 10:30 AM | Mid-Morning Snack | Handful of mixed nuts (almonds, walnuts, cashews) + 1 apple | 220 |
| 1:00 PM | Lunch | 2 rotis + dal tadka (1 bowl) + sabzi + 1 cup curd | 550 |
| 4:00 PM | Evening Snack | Peanut butter on 1 toast + 1 glass banana shake (milk + banana) | 300 |
| 7:30 PM | Dinner | Rice (1.5 cup cooked) + rajma / chole + salad + 1 glass milk | 550 |
| Total | ~2,140 kcal |
📅 DAY 2 (Tuesday)
| Time | Meal | Items | ~Kcal |
|---|---|---|---|
| 7:30 AM | Breakfast | Oats porridge with milk + 1 tbsp honey + 10 almonds + 1 banana | 510 |
| 10:30 AM | Mid-Morning Snack | 1 cup whole milk yogurt with 1 tbsp chia seeds + mango / any fruit | 210 |
| 1:00 PM | Lunch | 2 parathas with ghee + paneer bhurji + cucumber raita | 580 |
| 4:00 PM | Evening Snack | Cheese sandwich (2 slices) + 1 glass fresh juice | 290 |
| 7:30 PM | Dinner | Chicken curry / palak paneer + 2 rotis + dal + curd | 550 |
| Total | ~2,140 kcal |
📅 DAY 3 (Wednesday)
| Time | Meal | Items | ~Kcal |
|---|---|---|---|
| 7:30 AM | Breakfast | Vegetable poha + 2 boiled eggs / paneer cubes + 1 glass milk | 490 |
| 10:30 AM | Mid-Morning Snack | Date + walnut energy balls (4-5 pieces) | 240 |
| 1:00 PM | Lunch | Egg rice / jeera rice + chana masala + salad + curd | 560 |
| 4:00 PM | Evening Snack | Avocado / peanut butter on toast + 1 glass milk | 310 |
| 7:30 PM | Dinner | Dal makhani + 2 rotis + sabzi + 1 cup warm milk with turmeric | 530 |
| Total | ~2,130 kcal |
📅 DAY 4 (Thursday)
| Time | Meal | Items | ~Kcal |
|---|---|---|---|
| 7:30 AM | Breakfast | 2 idli / dosa + sambar + coconut chutney + 1 glass milk | 500 |
| 10:30 AM | Mid-Morning Snack | Roasted chana + 1 glass buttermilk | 200 |
| 1:00 PM | Lunch | Chicken biryani (home style) / paneer pulao + raita + salad | 600 |
| 4:00 PM | Evening Snack | Fruit salad with 2 tbsp cream / honey + handful of dry fruits | 280 |
| 7:30 PM | Dinner | Fish curry / tofu curry + 1.5 cup rice + dal + salad | 550 |
| Total | ~2,130 kcal |
📅 DAY 5 (Friday)
| Time | Meal | Items | ~Kcal |
|---|---|---|---|
| 7:30 AM | Breakfast | Whole wheat upma + 2 eggs scrambled + 1 glass banana milkshake | 530 |
| 10:30 AM | Mid-Morning Snack | Greek yogurt + 1 tbsp peanut butter + berries | 220 |
| 1:00 PM | Lunch | Rajma rice + aloo sabzi + curd + salad | 560 |
| 4:00 PM | Evening Snack | Whole wheat crackers + cheese + 1 glass milk | 300 |
| 7:30 PM | Dinner | Paneer tikka / grilled chicken + 2 rotis + dal + sabzi | 550 |
| Total | ~2,160 kcal |
📅 DAY 6 (Saturday)
| Time | Meal | Items | ~Kcal |
|---|---|---|---|
| 7:30 AM | Breakfast | Aloo paratha (2) with curd + 1 glass milk + 1 fruit | 560 |
| 10:30 AM | Mid-Morning Snack | Peanuts + raisins + 1 banana | 230 |
| 1:00 PM | Lunch | Chole bhature (1 serving) + onion salad + lassi | 580 |
| 4:00 PM | Evening Snack | Homemade energy bar (oats + honey + nuts) + 1 glass milk | 300 |
| 7:30 PM | Dinner | Dal fry + 2 rotis + mixed vegetable sabzi + curd | 520 |
| Total | ~2,190 kcal |
📅 DAY 7 (Sunday)
| Time | Meal | Items | ~Kcal |
|---|---|---|---|
| 8:00 AM | Brunch | Pancakes (2-3) with honey + 2 boiled eggs + 1 glass milk | 560 |
| 11:30 AM | Mid-Morning Snack | Smoothie: milk + banana + peanut butter + oats (blended) | 350 |
| 2:00 PM | Lunch | Mutton curry / soya chunks curry + rice + dal + raita | 600 |
| 5:00 PM | Evening Snack | Dry fruits ladoo (2 pieces) + 1 glass warm milk | 280 |
| 8:00 PM | Dinner | Soup + grilled paneer/chicken + 2 rotis + salad | 500 |
| Total | ~2,290 kcal |
🥤 Power Drinks to Add Daily
| Drink | Recipe | Kcal |
|---|---|---|
| Banana Milkshake | 1 banana + 1 glass full-fat milk + 1 tsp honey | ~280 |
| Peanut Butter Shake | 1 tbsp PB + 1 banana + milk | ~320 |
| Mango Lassi | Mango + curd + milk + honey | ~260 |
| Dry Fruit Milk | Warm milk + 5 almonds + 2 dates + pinch cardamom | ~200 |
| Avocado Smoothie | 1/2 avocado + milk + honey | ~300 |
🌿 Key Nutrients to Focus On
| Nutrient | Why | Best Sources |
|---|---|---|
| Protein | Muscle building | Eggs, milk, dal, paneer, chicken, fish |
| Iron | Prevents anemia, energy | Spinach, dal, chicken, raisins, jaggery |
| Calcium | Bone density | Milk, curd, paneer, ragi, sesame seeds |
| Vitamin D | Bone + immunity | Sunlight (15 min/day), eggs, fortified milk |
| Healthy Fats | Calorie density + hormones | Ghee, nuts, peanut butter, coconut |
| Complex Carbs | Sustained energy | Rice, oats, roti, sweet potato, banana |
✅ Simple Daily Rules
- Never skip breakfast - it sets the metabolism for the day
- Eat every 2.5 to 3 hours - small meals are easier to manage
- Add ghee to rotis and rice - a teaspoon adds healthy calories
- Drink water between meals, not during (so meals don't feel heavy)
- Bedtime snack always - warm milk + 2 dates or 5 almonds before sleep
- Limit plain tea - replace 1-2 cups with milk-based drinks
📈 Expected Progress
| Week | Expected Gain |
|---|---|
| Week 1-2 | Body adjusts, appetite increases |
| Week 3-4 | ~0.25 to 0.5 kg gain |
| Month 2-3 | ~1 to 1.5 kg gain |
| 6 months | ~3 to 4 kg - noticeable improvement in energy and appearance |
Slow gain = quality gain (muscle + healthy fat, not just water weight). Rushing it with junk food causes fat gain without health benefits.
⚕️ Final Reminder
- A basic blood test to check iron, Vitamin D, B12, thyroid
- Supplements if any deficiency is found
- Light strength exercises 2-3x/week (builds muscle mass)
- 7-9 hours of sleep every night