# Gross Anatomy of the Extrahepatic Biliary Apparatus ## OVERVIEW The extrahepatic biliary apparatus is the ductal system that conveys bile from the liver and gallbladder to the second part of the duodenum. It consists of: 1. **Right and Left Hepatic Ducts** 2. **Common Hepatic Duct (CHD)** 3. **Gallbladder** (with its cystic duct) 4. **Common Bile Duct (CBD) / Ductus Choledochus** 5. **Hepatopancreatic Ampulla (of Vater) and Major Duodenal Papilla** --- ## 1. RIGHT AND LEFT HEPATIC DUCTS ### Formation - The intrahepatic bile canaliculi converge to form segmental ducts, which unite to form the **right hepatic duct** and **left hepatic duct** within the liver substance. - They emerge at the **porta hepatis** (the transverse fissure on the visceral/inferior surface of the liver). ### Right Hepatic Duct - **Length:** Approximately 1–3 cm (shorter than the left) - Formed by the union of the **anterior sectoral duct** (draining segments V and VIII) and the **posterior sectoral duct** (draining segments VI and VII) - The anterior sectoral duct runs more vertically; the posterior sectoral duct runs more horizontally before joining - Lies within or very close to the liver substance before emerging at the porta hepatis - Receives the **cystic duct** in some anatomical variants (low union) ### Left Hepatic Duct - **Length:** Approximately 2–5 cm (longer than the right) - Formed by the union of ducts from segments II, III, and IV (and sometimes segment I/caudate lobe) - Has a longer extrahepatic course, making it more accessible for surgical anastomosis (e.g., hepaticojejunostomy in cases of hilar cholangiocarcinoma) - The **caudate lobe (segment I)** drains into both right and left hepatic ducts, or sometimes directly into their confluence ### **CLINICAL: Variant Ductal Anatomy** - In approximately **25–30%** of individuals, the right posterior sectoral duct drains into the left hepatic duct, the common hepatic duct, or even the cystic duct—an important consideration during cholecystectomy. - **Aberrant hepatic ducts** (ducts of Luschka) may drain directly from the liver bed into the gallbladder fossa. Injury during cholecystectomy can cause postoperative bile leaks. --- ## 2. COMMON HEPATIC DUCT (CHD) ### Formation - Formed by the union of the right and left hepatic ducts at the **porta hepatis** (hilum of the liver). - The point of confluence is called the **hepatic duct confluence** or **hepatic confluence (of the biliary system)**. ### Course - Descends within the **hepatoduodenal ligament** (the free edge of the lesser omentum). - Lies **anterior and to the right** of the portal vein. - Lies **to the left** of the proper hepatic artery and its right hepatic branch. ### Length - Approximately **3–4 cm** long. ### Diameter - Approximately **4–5 mm** (ultrasound normal: ≤6 mm; after cholecystectomy, up to 8–10 mm may be considered normal as the duct dilates to compensate for gallbladder loss). ### Termination - Joins the **cystic duct** (from the gallbladder) to form the **common bile duct (CBD)**. - The angle and level of this junction are variable. ### Relations within the Hepatoduodenal Ligament The hepatoduodenal ligament contains three key structures arranged as follows: - **CBD/CHD:** Anterolateral (right side) and to the right - **Proper hepatic artery:** Anterolateral (left side) and to the left - **Portal vein:** Posterior and between the two > **Mnemonic:** "**D**uct to the right, **A**rtery to the left, **V**ein behind" (DAV, from right to left) ### **CLINICAL: Pringle Maneuver** - The hepatoduodenal ligament can be compressed between the thumb and index finger (through the **epiploic foramen of Winslow**) to temporarily occlude the hepatic artery and portal vein, controlling hemorrhage from the liver. This is the **Pringle maneuver**. Safe clamping time is generally **15–20 minutes** before hepatic ischemia occurs. ### **CLINICAL: Hilar Cholangiocarcinoma (Klatskin Tumor)** - Tumors at the hepatic duct confluence are called **Klatskin tumors**. Classified by the **Bismuth-Corlette classification**: - Type I: Below the confluence - Type II: At the confluence - Type IIIa: Extends into right hepatic duct - Type IIIb: Extends into left hepatic duct - Type IV: Involves both right and left hepatic ducts (multicentric) - The longer extrahepatic course of the left hepatic duct makes left-sided hepaticojejunostomy technically easier. --- ## 3. GALLBLADDER ### Overview - A **pear-shaped** or piriform, hollow, musculomembranous sac. - Functions as a **reservoir** for bile, concentrating it 5–10 fold and releasing it during digestion. - **Capacity:** Approximately **30–50 mL** (can distend to hold up to 200–300 mL in pathological states like mucocele or empyema). - **Length:** 7–10 cm - **Width:** 2.5–3.5 cm ### Location - Lies in the **gallbladder fossa** on the **visceral (inferior) surface of the liver**, between the right lobe and the quadrate lobe. - The gallbladder fossa is one of the surface landmarks that helps define the **right sagittal fissure** of the liver. - Projects onto the anterior abdominal wall at the point where the **lateral border of the right rectus abdominis** meets the **right costal margin** (9th costal cartilage)—this is the approximate surface marking. - This corresponds to the tip of the 9th costal cartilage, or where the **transpyloric plane** (of Addison, at L1 level) intersects the right linea semilunaris. ### Parts of the Gallbladder The gallbladder is divided into four parts: #### a) Fundus - The **rounded, blind end** that projects beyond the inferior border of the liver. - It is completely covered by **peritoneum**. - It is in contact with the **anterior abdominal wall** (at the tip of the 9th costal cartilage) and the **transverse colon**. - Surface marking: Junction of the **right linea semilunaris** (lateral border of right rectus abdominis) and the **right costal margin** (transpyloric plane of Addison). - It is the part most commonly involved in **gangrene** during acute cholecystitis, because it is the most distal part and furthest from the cystic artery—the most vulnerable to ischemia. ##### **CLINICAL: Murphy's Sign** - During examination, the examiner places a hand at the right subcostal region (at the fundus location) and asks the patient to take a deep breath. If there is inflammation of the gallbladder (acute cholecystitis), the descending inflamed gallbladder comes into contact with the examining fingers, causing the patient to **catch their breath** (inspiratory arrest) due to pain. This is a **positive Murphy's sign**. - **Ultrasound Murphy's sign** (sonographic Murphy's sign) is considered more sensitive. #### b) Body - The main part, lying in the gallbladder fossa. - Related superiorly to the **visceral surface of the liver**. - Related inferiorly to the **transverse colon** and the **first or second part of the duodenum** (usually the superior/first part). - The body is covered by peritoneum on its inferior surface and sides, but the superior surface is attached to the liver by connective tissue (the **cystic plate**) — peritoneum does not intervene between the body of the gallbladder and the liver. ##### **CLINICAL: Gallstone Ileus** - When a large gallstone erodes through the body or fundus of the gallbladder into the adjacent duodenum or transverse colon (cholecystoduodenal or cholecystocolic fistula), it can enter the intestinal lumen and cause mechanical obstruction at the **ileocecal valve** (or less commonly at the duodenum—**Bouveret syndrome**). This is **gallstone ileus**. - Classic triad on imaging (Rigler's triad): **pneumobilia** (air in biliary tree), **bowel obstruction**, and **ectopic gallstone**. #### c) Neck - The **narrow, tapering end** that leads into the cystic duct. - Contains a mucosal fold called **Hartmann's pouch** (infundibulum)—a small saccular dilatation at the junction of the neck and body on the inferior surface. - The neck makes an **S-shaped curve** before continuing as the cystic duct. - Contains the **spiral valve of Heister** (actually in the cystic duct, but beginning at the neck-cystic duct junction). ##### **CLINICAL: Hartmann's Pouch** - **Gallstones frequently impact** in Hartmann's pouch. - An impacted stone in Hartmann's pouch can compress the adjacent common hepatic duct or common bile duct, causing obstructive jaundice. This is called **Mirizzi syndrome**. - **Type I:** External compression of the CHD/CBD by a stone in Hartmann's pouch or cystic duct. - **Type II:** Cholecystobiliary fistula with erosion of the stone into the CHD/CBD (involving <1/3 of the circumference). - **Type III:** Fistula involving up to 2/3 of the circumference. - **Type IV:** Fistula involving the entire circumference (complete destruction of the bile duct wall). #### d) Infundibulum - Some authors consider the infundibulum (Hartmann's pouch) as the transitional area between the body and neck. - It is not always present as a distinct anatomical structure but becomes prominent when distended with stones. ### Peritoneal Relations - The gallbladder is **not** completely covered by peritoneum. - The **fundus** is completely invested by peritoneum. - The **body** is covered by peritoneum on its inferior and lateral surfaces only (the superior surface is attached to the liver via the cystic plate—loose areolar tissue). - The gallbladder is therefore considered a **retroperitoneal** or, more accurately, a **secondarily retroperitoneal/subperitoneal** organ attached to the liver. #### **Variations in Peritoneal Covering:** - **Intrahepatic gallbladder:** Partially or completely embedded in the liver substance. More prone to difficulties during cholecystectomy. - **"Floating" or "Wandering" gallbladder:** Completely covered by peritoneum and suspended by a **mesentery** (mesentery of the gallbladder). This predisposes to **gallbladder torsion (volvulus)**. - **Left-sided gallbladder:** Rare anomaly; gallbladder located in the left hepatic fossa (associated with situs inversus or independently). - **Agenesis:** Rare congenital absence. - **Duplication:** Two separate gallbladders with two cystic ducts. - **Phrygian cap:** A fold in the fundus of the gallbladder—usually an incidental finding of no clinical significance. - **Multiseptate gallbladder:** Multiple septa within the gallbladder; may predispose to gallstone formation. - **Gallbladder diverticulum (Rokitansky-Aschoff sinuses):** Outpouchings of the mucosa through the muscular wall; seen in chronic cholecystitis and adenomyomatosis. ### Blood Supply #### Arterial Supply - **Cystic artery** — the principal arterial supply. - Usually a **single artery** arising from the **right hepatic artery** (in ~70% of cases). - The cystic artery typically passes **behind** the common hepatic duct (and sometimes behind the cystic duct) to reach the neck of the gallbladder. - It divides into a **superficial branch** (supplies the inferior/free peritoneal surface) and a **deep branch** (supplies the surface attached to the liver, runs between the gallbladder and the liver bed). - The cystic artery runs within the **cystohepatic triangle (Calot's triangle)** — see below. ##### **Variations in the Cystic Artery (Very Important Surgically):** - **Double cystic artery** (~15–20%): Two cystic arteries, one from the right hepatic artery and one from another source. - Origin from **left hepatic artery, proper hepatic artery, common hepatic artery, gastroduodenal artery, superior mesenteric artery**, or even **celiac trunk** (all rare but documented). - **Caterpillar turn/hump:** The right hepatic artery may be tortuous and form a loop (Moynihan's hump) that closely mimics the cystic artery, leading to inadvertent ligation during cholecystectomy. - An **accessory cystic artery** may be present. - The cystic artery may pass **anterior** to the common hepatic duct (in ~25% of cases) instead of posterior. ##### **CLINICAL: Cystic Artery Hemorrhage** - Injury to the cystic artery during cholecystectomy can cause significant hemorrhage. The critical view of safety (CVS) technique (see below) helps identify the cystic artery correctly. - If the right hepatic artery is mistakenly clipped instead of the cystic artery, it can cause **right hepatic lobe ischemia/necrosis**. #### Venous Drainage - Small veins (**cystic veins**) drain directly into the **liver** through the gallbladder bed (the venous drainage of the gallbladder bed goes directly into the hepatic sinusoids of segments IV and V—this is why gallbladder carcinoma tends to metastasize to the liver early). - A small cystic vein may also drain into the **right branch of the portal vein** or directly into the portal vein. ##### **CLINICAL: Gallbladder Carcinoma and Liver Metastasis** - Because of the direct venous drainage into the liver bed (segments IV and V), carcinoma of the gallbladder metastasizes early to these segments. Radical cholecystectomy for gallbladder cancer includes resection of the gallbladder bed (segments IVb and V) with regional lymphadenectomy. ### Lymphatic Drainage - **Cystic lymph node (node of Lund/Calot's node):** Located in the cystohepatic triangle (Calot's triangle), near the junction of the cystic duct and common hepatic duct. This is the **sentinel lymph node** of the gallbladder. - From the cystic node → **hepatic nodes** along the hepatic artery → **celiac nodes** → **cisterna chyli**. - Some lymphatics from the gallbladder also pass directly to **hepatic nodes** in the porta hepatis. - Lymphatics from the body and fundus may also drain through the liver bed into the **hepatic lymphatics**. ### Nerve Supply - **Sympathetic:** From the **celiac plexus** (T7–T9 spinal segments) via the hepatic plexus. Primarily vasomotor and conveys visceral pain. - **Parasympathetic:** From the **vagus nerve** (mainly the hepatic branch of the anterior vagal trunk). Stimulates contraction and secretion. - **Sensory/Pain:** Visceral afferents travel with the sympathetic fibers through the **greater splanchnic nerve** to spinal cord segments **T7–T9** (primarily the right side). ##### **CLINICAL: Referred Pain of Gallbladder Disease** - **Right hypochondrium/epigastrium:** Visceral pain from gallbladder distension or inflammation (T7–T9 dermatomes). - **Right shoulder tip/scapular region:** Referred pain via the **phrenic nerve (C3, C4, C5)**. This occurs when the inflamed gallbladder or subdiaphragmatic bile irritates the **diaphragmatic peritoneum** (supplied by the phrenic nerve). The pain is referred to the shoulder tip (supraclavicular region, C3–C5 dermatome)—known as **Kehr's sign** (more commonly used for splenic rupture but applicable to any diaphragmatic irritation). - **Boas' sign:** Hyperesthesia (increased sensitivity) in the area just below the right scapula, in acute cholecystitis—related to the T7–T9 dermatome. ### Histology (Brief, Relevant to Clinical Anatomy) - **Mucosa:** Columnar epithelium with extensive folds (rugae). No muscularis mucosae or submucosa (unlike the rest of the GI tract). This is why gallbladder carcinoma (which is usually adenocarcinoma) invades the muscular layer and serosa early—there's no submucosal barrier. - **Muscular layer:** Smooth muscle fibers in irregular bundles (not organized into distinct circular/longitudinal layers). - **Perimuscular connective tissue (subserosa)** - **Serosa (peritoneum):** Only on the free surface. ### Function - **Storage** of bile (between meals) - **Concentration** of bile (5–10 fold, by absorption of water, sodium, and chloride) - **Acidification** of bile - **Secretion of mucus** (mainly by the neck glands) - **Ejection of bile** into the duodenum in response to **cholecystokinin (CCK)**, released from I-cells of the duodenal and jejunal mucosa when fat and protein enter the duodenum. --- ## 4. CYSTIC DUCT ### Description - Connects the **neck of the gallbladder** to the **common hepatic duct** to form the **common bile duct**. - **Length:** Approximately 2–4 cm (highly variable—one of the most variable structures in the body). - **Diameter:** Approximately 1–3 mm. ### Course - Runs posteriorly, inferiorly, and to the left from the gallbladder neck. - Usually joins the **right side** of the common hepatic duct at an **acute angle**. - Runs within or along the **free edge** of the hepatoduodenal ligament. ### Spiral Valve of Heister - The cystic duct contains **mucosal folds** arranged in a **spiral pattern** (5–12 crescentic folds). - These are not true valves but rather **permanent mucosal ridges** that keep the lumen patent and regulate the flow of bile into and out of the gallbladder. - They prevent sudden distension or collapse of the cystic duct. - They make catheterization of the cystic duct difficult during **intraoperative cholangiography**. ### Variations in the Cystic Duct (Extremely Important Surgically) The cystic duct has **many variations**, making it one of the most dangerous structures during cholecystectomy: 1. **Angular junction (most common, ~75%):** Joins the right side of the CHD at an acute angle. 2. **Parallel (spiral) course:** The cystic duct runs parallel to the CHD for a variable distance before joining it (sometimes bound together by connective tissue). This can lead to misidentification of the CHD as the cystic duct. 3. **Low insertion:** Cystic duct joins the CHD very low, near the duodenum or even behind the pancreas. The parallel course variant may have a very low junction. 4. **High insertion:** Cystic duct joins the right hepatic duct (instead of the CHD). 5. **Medial insertion:** Cystic duct crosses anterior or posterior to the CHD and joins its left side. 6. **Absent cystic duct:** Gallbladder opens directly into the CHD (very rare, increases risk of bile duct injury). 7. **Very short cystic duct:** Functionally similar to absent cystic duct. 8. **Very long cystic duct:** May extend to the retroduodenal portion of the CBD. 9. **Double cystic duct:** Rare. 10. **Cystic duct joining the right hepatic duct or a segmental duct.** ##### **CLINICAL: Bile Duct Injury During Cholecystectomy** - The most common cause of bile duct injury during laparoscopic cholecystectomy is **misidentification of the CBD as the cystic duct**, especially when the cystic duct runs parallel to the CHD or when there is a short cystic duct. - The **"Critical View of Safety" (CVS)** (Strasberg's technique) is the gold standard method to prevent bile duct injury: - The hepatocystic triangle (Calot's triangle) is cleared of fat and fibrous tissue. - The lower end of the gallbladder is dissected off the liver bed (cystic plate). - **Two and only two structures** should be seen entering the gallbladder: the cystic duct and the cystic artery. - Only then should these structures be clipped and divided. - **Bile duct injuries** are classified by the **Strasberg classification (A–E)** or the **Bismuth classification** (for strictures): - Strasberg A: Leak from cystic duct stump or minor hepatic duct (duct of Luschka) - Strasberg B: Occlusion of an aberrant right hepatic duct - Strasberg C: Transection of an aberrant right hepatic duct - Strasberg D: Lateral injury to the CBD - Strasberg E: Further subdivided (E1–E5) corresponding to the Bismuth classification for strictures --- ## 5. CALOT'S TRIANGLE (CYSTOHEPATIC TRIANGLE / HEPATOBILIARY TRIANGLE) ### Definition - **Originally described by Jean-François Calot (1891):** The triangle bounded by: - **Cystic duct** (inferiorly) - **Common hepatic duct** (medially) - **Cystic artery** (superiorly) - **Modern/surgical definition (Hepatocystic triangle):** More commonly used today: - **Cystic duct** (inferiorly) - **Common hepatic duct** (medially) - **Inferior surface of the liver (visceral surface of segment V)** (superiorly) ### Contents of Calot's Triangle 1. **Cystic artery** (and its branches) 2. **Cystic lymph node (of Lund/Calot's node)** 3. **Connective tissue, fat, and lymphatics** 4. Occasionally: **Right hepatic artery** (if it takes an abnormal course), **accessory hepatic duct**, or an **aberrant right hepatic duct** ### **CLINICAL: Significance of Calot's Triangle** - This is the **primary area of dissection** during cholecystectomy. - All the dangerous structures that can be inadvertently injured are in or near this triangle. - The cystic artery usually crosses this triangle (in most cases posterior to the common hepatic duct, then crossing to the right toward the gallbladder). - The **right hepatic artery** frequently courses through or near the triangle—misidentification and ligation of this artery is a serious complication. - **Calot's node** is the first node to be involved in gallbladder malignancy and can be biopsied intraoperatively. --- ## 6. COMMON BILE DUCT (CBD) / DUCTUS CHOLEDOCHUS ### Formation - Formed by the **union of the common hepatic duct and the cystic duct**. - The junction typically occurs at the level of the **first part of the duodenum** or slightly above, but this is highly variable. ### Length - Approximately **7–8 cm** (range 5–15 cm, depending on where the cystic duct joins). ### Diameter - Approximately **6–8 mm**. - Normal ultrasound: **≤6 mm** (≤8 mm after cholecystectomy; increases with age: add 1 mm per decade after 60 years). - A CBD diameter **>8 mm** (or >10 mm post-cholecystectomy) is considered dilated and suggests obstruction. ### Course and Parts The CBD is divided into **four parts** based on its relations: #### a) Supraduodenal Part - **Length:** ~2–4 cm - Runs in the **free edge of the hepatoduodenal ligament (lesser omentum)**. - Lies to the **right and anterior** to the **portal vein**. - Lies to the **right** of the **proper hepatic artery**. - This is the most **accessible** part surgically. - This is where **choledochotomy** (surgical incision into the CBD) is performed for CBD exploration and stone extraction. - **Relations:** - Anterior: First part of duodenum (sometimes) - Posterior: Portal vein, epiploic foramen - Left: Proper hepatic artery - Right: Free edge of lesser omentum #### b) Retroduodenal Part - **Length:** ~1–2 cm - Passes **behind the first part of the duodenum** (superior/first part of the duodenum). - Still accompanied by the portal vein (posteriorly) and the gastroduodenal artery (to its left, which is now anterior to the portal vein). - The **gastroduodenal artery** crosses anterior to the CBD here. #### c) Infraduodenal (Pancreatic/Retropancreatic) Part - **Length:** ~3 cm - Runs **behind the head of the pancreas** or is **embedded within** the posterior aspect of the pancreatic head, in a groove on its posterior surface. - This is the longest part. - Closely related to the **main pancreatic duct (of Wirsung)**, which runs from left to right through the pancreas and approaches the CBD from the left. - The CBD and main pancreatic duct converge as they approach the duodenal wall. ##### **CLINICAL: Carcinoma of the Head of the Pancreas** - Tumors of the pancreatic head (most commonly ductal adenocarcinoma) compress or obstruct the intrapancreatic portion of the CBD, causing: - **Painless, progressive obstructive jaundice** (the classic presentation) - **Courvoisier's law/sign:** "In the presence of jaundice, a palpable gallbladder is unlikely to be due to gallstones." Rationale: In gallstone disease, the gallbladder wall is fibrosed from chronic inflammation and cannot distend. In malignant obstruction (pancreatic head tumor), the obstruction is gradual, and the gallbladder wall is normal, so it distends. - Exceptions to Courvoisier's law: Double impaction of stones (one in cystic duct, one in CBD), a stone in Hartmann's pouch with a separate stone in CBD, or mucocele of the gallbladder. - **Pale/clay-colored stools (acholic stools):** Due to absence of bile pigments in the gut. - **Dark urine (tea/cola-colored):** Due to conjugated bilirubin in urine. - **Steatorrhea:** Due to absence of bile salts in the gut (fat malabsorption). - **Pruritus:** Due to deposition of bile salts in the skin. - **Coagulopathy:** Due to malabsorption of fat-soluble vitamin K. #### d) Intraduodenal (Intramural) Part - **Length:** ~1.5–2 cm - The CBD passes **obliquely** through the **posteromedial wall** of the **second part (descending part) of the duodenum**. - Runs obliquely through the duodenal wall for ~2 cm—this oblique course creates a **valve-like mechanism** that prevents duodenal reflux into the biliary system. - Usually joins the **main pancreatic duct (of Wirsung)** to form the **hepatopancreatic ampulla (ampulla of Vater)**. - Opens at the **major duodenal papilla** on the posteromedial wall of the second part of the duodenum, approximately at the junction of the **middle and lower thirds** of the second part, about **8–10 cm distal** to the pylorus. --- ## 7. HEPATOPANCREATIC AMPULLA (AMPULLA OF VATER) AND SPHINCTER OF ODDI ### Hepatopancreatic Ampulla - The **dilated terminal portion** formed by the union of the CBD and the main pancreatic duct. - **Length:** Approximately 1–14 mm (variable). - Opens at the summit of the **major duodenal papilla**. ### Variations in CBD-Pancreatic Duct Junction The manner in which the CBD and main pancreatic duct terminate is highly variable: 1. **Type 1 (Most common, ~60–70%):** CBD and main pancreatic duct unite **before** entering the duodenal wall, forming a **common channel** (the ampulla of Vater). 2. **Type 2 (~20–30%):** CBD and main pancreatic duct enter the duodenum **separately** through **separate openings** on the major papilla, with no true ampulla. 3. **Type 3 (~5%):** CBD and main pancreatic duct unite **within the duodenal wall** with a very short common channel. ##### **CLINICAL: Anomalous Pancreaticobiliary Junction (APBJ)** - When the junction of the CBD and pancreatic duct occurs **outside the duodenal wall** (long common channel >15 mm), the sphincter of Oddi cannot regulate the reflux of pancreatic juice into the biliary system. - This leads to chronic reflux of pancreatic enzymes into the biliary tree, causing: - **Choledochal cysts** (especially Type I and Type IV) - Increased risk of **gallbladder carcinoma** and **bile duct carcinoma** - This is especially common in **Asian populations** and in children with choledochal cysts. ### Sphincter of Oddi (Sphincter of the Hepatopancreatic Ampulla) A complex arrangement of smooth muscle surrounding the terminal portions of the CBD, pancreatic duct, and the ampulla. It consists of: 1. **Sphincter choledochus (sphincter of the bile duct):** Surrounds the terminal intramural portion of the CBD. This is the **most important** sphincter—it controls bile flow. 2. **Sphincter pancreaticus:** Surrounds the terminal portion of the main pancreatic duct (weaker and less constant than the sphincter choledochus). 3. **Sphincter ampullae (of the hepatopancreatic ampulla):** Surrounds the common channel/ampulla itself. #### Functions of the Sphincter of Oddi - **Regulates bile flow** into the duodenum - **Prevents reflux** of duodenal contents into the biliary and pancreatic systems - **Prevents reflux** of pancreatic juice into the biliary system (and vice versa) - **Controls filling of the gallbladder:** When the sphincter is closed (between meals), bile backs up and fills the gallbladder via the cystic duct. - **Relaxation** is primarily mediated by **CCK** (cholecystokinin), which simultaneously causes gallbladder contraction and sphincter relaxation, allowing bile to flow into the duodenum. ##### **CLINICAL: Sphincter of Oddi Dysfunction (SOD)** - Functional disorder causing biliary-type pain, elevated liver enzymes, and/or recurrent pancreatitis without organic obstruction. - Classified into **Type I, II, and III** (Milwaukee classification) based on clinical, laboratory, and imaging criteria. - Diagnosed by **sphincter of Oddi manometry** (gold standard). - Treated by **endoscopic sphincterotomy**. ### Major Duodenal Papilla - The elevation on the **posteromedial wall** of the **second part of the duodenum** where the ampulla of Vater opens. - Located approximately **8–10 cm** from the pylorus. - A **mucosal fold** called the **plica longitudinalis duodeni** (longitudinal fold of the duodenum) extends vertically along the posteromedial wall of the duodenum, with the major papilla at its lower end. - A **hooded fold (plica)** may cover the papilla superiorly. ### Minor Duodenal Papilla - Located **approximately 2 cm proximal (superior)** to the major papilla. - This is where the **accessory pancreatic duct (of Santorini)** opens. - The minor papilla has a **separate, smaller sphincter** (sphincter of Helly). ##### **CLINICAL: ERCP (Endoscopic Retrograde Cholangiopancreatography)** - The major duodenal papilla is the target of ERCP, where an endoscope is passed through the mouth, esophagus, stomach, and into the second part of the duodenum. A catheter is then inserted into the papilla, and contrast is injected to visualize the biliary and pancreatic ducts. - **Endoscopic sphincterotomy:** The sphincter of Oddi is cut (usually at the 11–12 o'clock position to avoid the pancreatic duct, which lies at 4–5 o'clock) to facilitate stone extraction or stent placement. - **Complications of ERCP:** Post-ERCP pancreatitis (most common, 3–5%), hemorrhage, perforation, cholangitis. ##### **CLINICAL: Gallstone Impaction at the Ampulla** - Gallstones passing through the CBD can impact at the ampulla of Vater, causing: - **Obstructive jaundice** - **Acute pancreatitis** (gallstone pancreatitis—the most common cause of acute pancreatitis in many populations). The stone blocks the common channel, causing reflux of bile into the pancreatic duct, or it blocks the pancreatic duct outflow directly. - **Cholangitis** (Charcot's triad: fever with rigors, jaundice, right upper quadrant pain) - **Reynold's pentad:** Charcot's triad + hypotension + altered mental status (indicating septic/suppurative cholangitis—a surgical emergency requiring urgent biliary decompression) --- ## 8. ACCESSORY PANCREATIC DUCT (OF SANTORINI) - Opens at the **minor duodenal papilla**. - Drains the **uncinate process and part of the head of the pancreas**. - In approximately **10%** of people, it is the **dominant** (main) drainage pathway (this is called **pancreas divisum**). ##### **CLINICAL: Pancreas Divisum** - The most common congenital anomaly of the pancreas (~5–10% of the population). - The **dorsal** and **ventral pancreatic ducts fail to fuse** during embryological development. - The **majority** of the pancreas (body and tail from the dorsal bud) drains through the **minor papilla** via the accessory duct, while only the uncinate process (from the ventral bud) drains through the **major papilla** via the main duct. - May predispose to **recurrent pancreatitis** if the minor papilla orifice is too small to handle the increased flow. --- ## 9. ARTERIAL SUPPLY OF THE EXTRAHEPATIC BILIARY SYSTEM ### Overview The blood supply of the bile ducts is **predominantly axial** (running along the length of the ducts) and is derived from a complex network: ### Sources 1. **Cystic artery** → supplies the gallbladder and upper portion of the cystic duct. 2. **Right hepatic artery** → supplies the common hepatic duct and upper part of the CBD (supraduodenal part). 3. **Posterior superior pancreaticoduodenal artery** (branch of gastroduodenal artery) and **retroduodenal artery** → supply the retroduodenal and pancreatic portions of the CBD. 4. **Gastroduodenal artery** → contributes to the retroduodenal portion. ### Marginal Arteries (of the Bile Duct) - The bile ducts receive their blood supply from **two axial vessels** running along the bile duct: - **3 o'clock artery** (lateral marginal artery) - **9 o'clock artery** (medial marginal artery) - These are small arteries that run along the lateral (right) and medial (left) borders of the CBD/CHD. - They form a **periductal vascular plexus (epicholedochal plexus)** around the bile duct. ### Blood Supply Pattern - **60% of the blood supply** to the supraduodenal CBD comes from **below** (retroduodenal artery/gastroduodenal artery) and travels upward. - **38%** comes from **above** (right hepatic artery/cystic artery). - Only **2%** is from non-axial sources. ##### **CLINICAL: Bile Duct Ischemia and Stricture** - The supraduodenal CBD is particularly vulnerable to ischemia because it depends on axial blood supply from small marginal arteries. - Excessive dissection, cautery, or skeletonization of the bile duct during surgery can damage the **3 o'clock and 9 o'clock arteries**, leading to: - **Ischemic bile duct stricture** (a devastating complication) - **Bile duct necrosis and leak** - During **liver transplantation**, the blood supply to the donor bile duct is entirely dependent on axial vessels from below (the hepatic artery). If the hepatic artery thromboses, the bile duct becomes ischemic, leading to **ischemic-type biliary lesions (ITBL)** and anastomotic strictures. --- ## 10. VENOUS DRAINAGE OF THE EXTRAHEPATIC BILIARY SYSTEM - Veins from the bile ducts drain into the **portal venous system**: - Upper bile duct veins → **portal vein** branches - Lower bile duct veins → **posterior superior pancreaticoduodenal vein** → **portal vein** - **Gallbladder veins:** Drain directly into the liver bed (hepatic sinusoids of segments IV and V) or via small cystic veins into the portal vein. --- ## 11. LYMPHATIC DRAINAGE OF THE EXTRAHEPATIC BILIARY SYSTEM The lymphatic drainage follows a predictable pathway: 1. **Cystic lymph node (of Lund):** First node; lies in Calot's triangle. 2. **Pericholedochal nodes:** Along the CBD. 3. **Hilar nodes (hepatic nodes):** At the porta hepatis. 4. **Nodes along the common hepatic artery.** 5. **Retropancreatic and retroduodenal nodes.** 6. **Celiac nodes.** 7. **Para-aortic (interaortocaval) nodes.** 8. Ultimately → **Cisterna chyli** → **Thoracic duct.** ##### **CLINICAL: Nodal Staging in Gallbladder and Bile Duct Cancer** - Regional lymph node involvement significantly affects staging and prognosis. - For gallbladder carcinoma, N1 nodes include: cystic duct node, pericholedochal, hilar, periportal, and proper hepatic artery nodes. - N2 nodes include: celiac, periaortic, pericaval, and superior mesenteric artery nodes. --- ## 12. NERVE SUPPLY OF THE EXTRAHEPATIC BILIARY SYSTEM ### Sympathetic - From the **celiac plexus** (greater splanchnic nerve, T5–T9, primarily T7–T9). - Vasomotor function. - Conveys **visceral pain** afferents. ### Parasympathetic - From the **vagus nerve** (hepatic branch of the anterior vagal trunk). - Stimulates gallbladder contraction and bile secretion. - Relaxation of the sphincter of Oddi (although CCK is the primary regulator). ### Sensory/Pain Pathway - Visceral afferents travel with the **sympathetic fibers** (greater splanchnic nerve) to the spinal cord segments **T5–T9**. - **Dermatomes T7–T9:** Right hypochondrium, epigastrium. - **Referred pain:** Right shoulder tip (C3–C5, phrenic nerve) when the diaphragm is irritated by biliary pathology. ##### **CLINICAL: Biliary Colic** - The pain of biliary colic is visceral in nature: poorly localized, deep, and typically felt in the **epigastrium** or **right hypochondrium**. - It is caused by gallbladder contraction against an obstructed cystic duct (usually by a gallstone). - Despite the name "colic," the pain is usually **constant** (not true colicky/intermittent) and lasts 1–5 hours. - It is NOT worsened by movement (unlike peritonitis). - The pain may radiate to the **right scapular region** (referred pain via T7–T9 dermatomes) or the **right shoulder tip** (phrenic nerve involvement if there is diaphragmatic irritation). --- ## 13. EMBRYOLOGY (Brief, Clinically Relevant) - The extrahepatic biliary apparatus develops from the **hepatic diverticulum (liver bud)**, an outgrowth of the ventral wall of the foregut (future duodenum) during the **4th week** of development. - The hepatic diverticulum divides into: - **Cranial part (pars hepatica):** Gives rise to the liver parenchyma and intrahepatic bile ducts. - **Caudal part (pars cystica):** Gives rise to the **gallbladder and cystic duct**. - The stalk of the hepatic diverticulum becomes the **common bile duct**. - The connection to the duodenum (common hepatic duct) develops from the stalk above the cystic duct origin. ##### **CLINICAL: Biliary Atresia** - Failure of normal development or destruction of the extrahepatic bile ducts, either during fetal life or shortly after birth. - The most common cause of **neonatal obstructive jaundice** requiring surgery. - Presents with **conjugated (direct) hyperbilirubinemia**, pale stools, dark urine, and hepatomegaly in the neonate. - **Kasai procedure (hepatoportoenterostomy):** A Roux-en-Y loop of jejunum is anastomosed to the porta hepatis to allow bile drainage. Must be performed **before 8 weeks of age** for the best outcome. - If Kasai fails → **liver transplantation** (biliary atresia is the most common indication for pediatric liver transplantation). ##### **CLINICAL: Choledochal Cysts** - Congenital cystic dilatations of the biliary tree. - **Todani classification:** - **Type I (most common, ~50–80%):** Fusiform (Ia), focal (Ib), or diffuse (Ic) dilatation of the CBD. - **Type II:** True diverticulum of the CBD. - **Type III (Choledochocele):** Dilatation of the intraduodenal portion of the CBD. - **Type IV:** Multiple cysts: - **IVa (2nd most common):** Both intrahepatic and extrahepatic cysts. - **IVb:** Multiple extrahepatic cysts only. - **Type V (Caroli disease):** Multiple intrahepatic cysts (strictly not extrahepatic, but included in the classification). - Associated with **anomalous pancreaticobiliary junction (APBJ)** in up to 90% of cases. - Risk of **cholangiocarcinoma** (10–30% lifetime risk) if untreated. - Treatment: **Complete excision** of the cyst with **Roux-en-Y hepaticojejunostomy** (for Types I and IV). Type III (choledochocele) may be treated by endoscopic sphincterotomy. --- ## 14. APPLIED ANATOMY & ADDITIONAL CLINICAL CORRELATIONS ### Cholecystectomy (Surgical Removal of the Gallbladder) #### Laparoscopic Cholecystectomy (Gold Standard) - **Port placement:** Usually 4 ports (American technique) or 3 ports (French technique). - Dissection proceeds in Calot's triangle. - **Critical View of Safety (CVS):** As described above—the most important step to prevent bile duct injury. - **Intraoperative cholangiography (IOC):** A catheter is placed in the cystic duct, and contrast is injected under fluoroscopy to delineate the biliary anatomy and detect CBD stones. - **"Fundus first" or "Top-down" cholecystectomy:** Used when the anatomy in Calot's triangle is unclear (e.g., severe inflammation in acute cholecystitis). The gallbladder is dissected from the liver bed starting at the fundus, progressing toward the neck. - **Subtotal cholecystectomy:** In cases of severe inflammation where safe dissection of Calot's triangle is impossible, the fundus and body are removed, but the posterior wall of the gallbladder (attached to the liver) or the Hartmann's pouch area is left in situ with the cystic duct stump secured from inside (reconstituting technique) or left open with a drain (fenestrating technique). #### Open Cholecystectomy - Performed through a **right subcostal (Kocher's) incision** or a **right paramedian incision**. - May be necessary in cases of severe inflammation, suspected gallbladder cancer, or inability to complete laparoscopic surgery. ### Cholecystostomy - Percutaneous or surgical placement of a drain into the gallbladder for decompression. - Used in critically ill patients with acute cholecystitis who are unfit for cholecystectomy. - **Percutaneous cholecystostomy** is image-guided (ultrasound or CT). ### CBD Exploration - Performed when CBD stones are suspected or confirmed. - **Supraduodenal choledochotomy:** An incision is made in the anterior wall of the supraduodenal CBD (the most accessible part). Stones are extracted using forceps, balloon catheters, or choledochoscopy. - The choledochotomy may be closed primarily over a **T-tube** (to decompose and allow post-operative cholangiography) or closed primarily without a T-tube (if the duct is of adequate diameter and the papilla is patent). ### Choledochoduodenostomy and Choledochojejunostomy - **Choledochoduodenostomy:** Anastomosis between the CBD and the duodenum (for recurrent CBD stones, failed ERCP, or distal CBD obstruction). - **Choledochojejunostomy (Roux-en-Y hepaticojejunostomy):** Anastomosis between the CBD (or CHD or hepatic ducts) and a Roux-en-Y loop of jejunum. Used for benign and malignant bile duct strictures, bile duct injuries, choledochal cysts, and after Whipple's procedure (pancreaticoduodenectomy). ### Whipple's Procedure (Pancreaticoduodenectomy) - Performed for periampullary carcinoma (pancreatic head, ampulla of Vater, distal CBD, or duodenum). - Involves resection of the head of the pancreas, duodenum, distal CBD, gallbladder, and distal stomach (in classic Whipple) or pylorus preservation (in pylorus-preserving Whipple/PPPD). - Reconstruction involves: - **Pancreaticojejunostomy** (or pancreaticogastrostomy) - **Hepaticojejunostomy** (bile duct-jejunum anastomosis) - **Gastrojejunostomy** (or duodenojejunostomy in PPPD) ### Courvoisier's Gallbladder (Reiterated) - A **palpable, non-tender, distended gallbladder** in a jaundiced patient suggests **malignant obstruction** of the CBD (e.g., pancreatic head carcinoma, periampullary carcinoma, cholangiocarcinoma of the distal CBD). ### Charcot's Triad and Reynold's Pentad (Reiterated) - **Charcot's triad (acute cholangitis):** Fever + Jaundice + Right upper quadrant pain. - **Reynold's pentad (suppurative cholangitis):** Charcot's triad + Hypotension + Altered mental status. - Requires urgent biliary decompression (ERCP with sphincterotomy and stenting, or percutaneous transhepatic biliary drainage). ### Gallstone Types Although this is more pathological, it relates to the biliary apparatus: 1. **Cholesterol stones** (~80% in Western countries): Yellow-green, occur in supersaturated bile. 2. **Pigment stones:** - **Black pigment stones:** Associated with hemolytic conditions (e.g., sickle cell disease, hereditary spherocytosis), cirrhosis. Found in the gallbladder. - **Brown pigment stones:** Associated with biliary infections and stasis (especially in Asian populations). Found in the bile ducts (primary choledocholithiasis). 3. **Mixed stones:** Most common overall. ### Risk Factors for Gallstones ("6 F's") - **Female** - **Fat (obese)** - **Forty (age >40)** - **Fertile (multiparity)** - **Fair (Caucasian, Native American, Hispanic)** - **(Family history)** ### Additional: Porcelain Gallbladder - Calcification of the gallbladder wall. - Previously thought to have a very high risk of gallbladder carcinoma (historically quoted as ~25%), but recent studies suggest the risk may be lower (~5–7%). - Nevertheless, **prophylactic cholecystectomy** is generally recommended. ### Additional: Gallbladder Polyps - Polyps **>10 mm** have a higher risk of malignancy → cholecystectomy recommended. - Polyps **6–10 mm:** Follow-up with serial ultrasound. - Polyps **<6 mm:** Usually cholesterol polyps, benign. --- ## 15. SUMMARY OF KEY RELATIONSHIPS ### Hepatoduodenal Ligament Contents (Anterior to Posterior) | Position | Structure | |----------|-----------| | Right, anterior | CBD (above) / CHD (below the cystic duct junction) | | Left, anterior | Proper hepatic artery | | Posterior, central | Portal vein | Also contains: Hepatic nerve plexus, lymphatics, lymph nodes. ### Epiploic Foramen (of Winslow) - **Anterior boundary:** Free edge of the hepatoduodenal ligament (containing CBD, hepatic artery, portal vein). - **Posterior boundary:** IVC (covered by peritoneum). - **Superior boundary:** Caudate lobe of the liver (caudate process). - **Inferior boundary:** First part of the duodenum. - This foramen connects the **greater sac** with the **lesser sac (omental bursa)**. - **Pringle maneuver** is performed by compressing the contents of the hepatoduodenal ligament through the epiploic foramen. --- ## 16. IMAGING OF THE BILIARY SYSTEM ### Ultrasound (First-line) - Best initial investigation for gallstones, gallbladder wall thickening, bile duct dilatation. - Normal CBD ≤6 mm (≤8–10 mm post-cholecystectomy). - **Sonographic Murphy's sign:** Focal tenderness over the gallbladder when compressed by the ultrasound probe → acute cholecystitis. ### MRCP (Magnetic Resonance Cholangiopancreatography) - Non-invasive imaging of the biliary tree using heavily T2-weighted MRI sequences. - Excellent for detecting CBD stones, bile duct strictures, choledochal cysts, and biliary anatomy. ### ERCP (Endoscopic Retrograde Cholangiopancreatography) - Both diagnostic and therapeutic. - Gold standard for managing CBD stones (sphincterotomy + stone extraction). - Can place stents for malignant biliary obstruction. ### PTC (Percutaneous Transhepatic Cholangiography) - Needle puncture through the liver into a dilated intrahepatic bile duct, followed by contrast injection. - Used when ERCP fails or is not possible (e.g., altered surgical anatomy after Roux-en-Y). ### EUS (Endoscopic Ultrasound) - High-resolution imaging of the distal CBD, ampulla, and pancreatic head. - Excellent sensitivity for small CBD stones (<5 mm) and periampullary tumors. - Allows FNA (fine needle aspiration) of masses. ### HIDA Scan (Hepatobiliary Iminodiacetic Acid Scan) - Nuclear medicine study using technetium-99m-labeled IDA analogues. - The radiotracer is taken up by hepatocytes and excreted into the biliary system. - **Non-visualization of the gallbladder** within 60 minutes (or 4 hours with morphine augmentation) → **acute cholecystitis** (cystic duct obstruction). - Also useful for diagnosing bile leaks, biliary atresia (in neonates), and biliary dyskinesia (by calculating the gallbladder ejection fraction after CCK stimulation—normal >35%). --- ## CONCLUSION The extrahepatic biliary apparatus is a clinically critical anatomical region with **highly variable anatomy**, particularly regarding the cystic duct, cystic artery, and hepatic ductal variants. A thorough understanding of its anatomy—including the relationships within Calot's triangle, the blood supply of the bile ducts, the sphincter of Oddi mechanism, and the numerous anatomical variants—is essential for safe surgical practice, particularly during cholecystectomy, CBD exploration, and hepatopancreatobiliary surgery. The clinical correlations—from gallstone disease and obstructive jaundice to bile duct injury prevention and biliary malignancies—are among the most frequently tested and clinically encountered topics in surgery and gastroenterology. Rewrite the whole content as it is plus add maximum number of high yield images along the content
extrahepatic biliary apparatus anatomy diagram gallbladder bile duct Calot's triangle labeled image
hepatopancreatic ampulla sphincter of Oddi anatomy diagram labeled medical
Mirizzi syndrome Courvoisier gallbladder Klatskin tumor bismuth classification anatomy diagram
gallbladder parts fundus body neck cystic duct anatomy labeled diagram medical education
Gross Anatomy of the Extrahepatic Biliary Apparatus
OVERVIEW
- Right and Left Hepatic Ducts
- Common Hepatic Duct (CHD)
- Gallbladder (with its cystic duct)
- Common Bile Duct (CBD) / Ductus Choledochus
- Hepatopancreatic Ampulla (of Vater) and Major Duodenal Papilla
1. RIGHT AND LEFT HEPATIC DUCTS
Formation
- The intrahepatic bile canaliculi converge to form segmental ducts, which unite to form the right hepatic duct and left hepatic duct within the liver substance.
- They emerge at the porta hepatis (the transverse fissure on the visceral/inferior surface of the liver).
Right Hepatic Duct
- Length: Approximately 1-3 cm (shorter than the left)
- Formed by the union of the anterior sectoral duct (draining segments V and VIII) and the posterior sectoral duct (draining segments VI and VII)
- The anterior sectoral duct runs more vertically; the posterior sectoral duct runs more horizontally before joining
- Lies within or very close to the liver substance before emerging at the porta hepatis
- Receives the cystic duct in some anatomical variants (low union)
Left Hepatic Duct
- Length: Approximately 2-5 cm (longer than the right)
- Formed by the union of ducts from segments II, III, and IV (and sometimes segment I/caudate lobe)
- Has a longer extrahepatic course, making it more accessible for surgical anastomosis (e.g., hepaticojejunostomy in cases of hilar cholangiocarcinoma)
- The caudate lobe (segment I) drains into both right and left hepatic ducts, or sometimes directly into their confluence
CLINICAL: Variant Ductal Anatomy
- In approximately 25-30% of individuals, the right posterior sectoral duct drains into the left hepatic duct, the common hepatic duct, or even the cystic duct - an important consideration during cholecystectomy.
- Aberrant hepatic ducts (ducts of Luschka) may drain directly from the liver bed into the gallbladder fossa. Injury during cholecystectomy can cause postoperative bile leaks.
2. COMMON HEPATIC DUCT (CHD)
Formation
- Formed by the union of the right and left hepatic ducts at the porta hepatis (hilum of the liver).
- The point of confluence is called the hepatic duct confluence or hepatic confluence (of the biliary system).
Course
- Descends within the hepatoduodenal ligament (the free edge of the lesser omentum).
- Lies anterior and to the right of the portal vein.
- Lies to the left of the proper hepatic artery and its right hepatic branch.
Length
- Approximately 3-4 cm long.
Diameter
- Approximately 4-5 mm (ultrasound normal: ≤6 mm; after cholecystectomy, up to 8-10 mm may be considered normal as the duct dilates to compensate for gallbladder loss).
Termination
- Joins the cystic duct (from the gallbladder) to form the common bile duct (CBD).
- The angle and level of this junction are variable.
Relations within the Hepatoduodenal Ligament
- CBD/CHD: Anterolateral (right side) and to the right
- Proper hepatic artery: Anterolateral (left side) and to the left
- Portal vein: Posterior and between the two
Mnemonic: "Duct to the right, Artery to the left, Vein behind" (DAV, from right to left)
CLINICAL: Pringle Maneuver
- The hepatoduodenal ligament can be compressed between the thumb and index finger (through the epiploic foramen of Winslow) to temporarily occlude the hepatic artery and portal vein, controlling hemorrhage from the liver. This is the Pringle maneuver. Safe clamping time is generally 15-20 minutes before hepatic ischemia occurs.
CLINICAL: Hilar Cholangiocarcinoma (Klatskin Tumor)
- Tumors at the hepatic duct confluence are called Klatskin tumors. Classified by the Bismuth-Corlette classification:
- Type I: Below the confluence
- Type II: At the confluence
- Type IIIa: Extends into right hepatic duct
- Type IIIb: Extends into left hepatic duct
- Type IV: Involves both right and left hepatic ducts (multicentric)
- The longer extrahepatic course of the left hepatic duct makes left-sided hepaticojejunostomy technically easier.
3. GALLBLADDER
Overview
- A pear-shaped or piriform, hollow, musculomembranous sac.
- Functions as a reservoir for bile, concentrating it 5-10 fold and releasing it during digestion.
- Capacity: Approximately 30-50 mL (can distend to hold up to 200-300 mL in pathological states like mucocele or empyema).
- Length: 7-10 cm
- Width: 2.5-3.5 cm
Location
- Lies in the gallbladder fossa on the visceral (inferior) surface of the liver, between the right lobe and the quadrate lobe.
- The gallbladder fossa is one of the surface landmarks that helps define the right sagittal fissure of the liver.
- Projects onto the anterior abdominal wall at the point where the lateral border of the right rectus abdominis meets the right costal margin (9th costal cartilage) - this is the approximate surface marking.
- This corresponds to the tip of the 9th costal cartilage, or where the transpyloric plane (of Addison, at L1 level) intersects the right linea semilunaris.
Parts of the Gallbladder
a) Fundus
- The rounded, blind end that projects beyond the inferior border of the liver.
- It is completely covered by peritoneum.
- It is in contact with the anterior abdominal wall (at the tip of the 9th costal cartilage) and the transverse colon.
- Surface marking: Junction of the right linea semilunaris (lateral border of right rectus abdominis) and the right costal margin (transpyloric plane of Addison).
- It is the part most commonly involved in gangrene during acute cholecystitis, because it is the most distal part and furthest from the cystic artery - the most vulnerable to ischemia.
CLINICAL: Murphy's Sign
- During examination, the examiner places a hand at the right subcostal region (at the fundus location) and asks the patient to take a deep breath. If there is inflammation of the gallbladder (acute cholecystitis), the descending inflamed gallbladder comes into contact with the examining fingers, causing the patient to catch their breath (inspiratory arrest) due to pain. This is a positive Murphy's sign.
- Ultrasound Murphy's sign (sonographic Murphy's sign) is considered more sensitive.
b) Body
- The main part, lying in the gallbladder fossa.
- Related superiorly to the visceral surface of the liver.
- Related inferiorly to the transverse colon and the first or second part of the duodenum (usually the superior/first part).
- The body is covered by peritoneum on its inferior surface and sides, but the superior surface is attached to the liver by connective tissue (the cystic plate) - peritoneum does not intervene between the body of the gallbladder and the liver.
CLINICAL: Gallstone Ileus
- When a large gallstone erodes through the body or fundus of the gallbladder into the adjacent duodenum or transverse colon (cholecystoduodenal or cholecystocolic fistula), it can enter the intestinal lumen and cause mechanical obstruction at the ileocecal valve (or less commonly at the duodenum - Bouveret syndrome). This is gallstone ileus.
- Classic triad on imaging (Rigler's triad): pneumobilia (air in biliary tree), bowel obstruction, and ectopic gallstone.
c) Neck
- The narrow, tapering end that leads into the cystic duct.
- Contains a mucosal fold called Hartmann's pouch (infundibulum) - a small saccular dilatation at the junction of the neck and body on the inferior surface.
- The neck makes an S-shaped curve before continuing as the cystic duct.
- Contains the spiral valve of Heister (actually in the cystic duct, but beginning at the neck-cystic duct junction).
CLINICAL: Hartmann's Pouch
- Gallstones frequently impact in Hartmann's pouch.
- An impacted stone in Hartmann's pouch can compress the adjacent common hepatic duct or common bile duct, causing obstructive jaundice. This is called Mirizzi syndrome.
- Type I: External compression of the CHD/CBD by a stone in Hartmann's pouch or cystic duct.
- Type II: Cholecystobiliary fistula with erosion of the stone into the CHD/CBD (involving <1/3 of the circumference).
- Type III: Fistula involving up to 2/3 of the circumference.
- Type IV: Fistula involving the entire circumference (complete destruction of the bile duct wall).
d) Infundibulum
- Some authors consider the infundibulum (Hartmann's pouch) as the transitional area between the body and neck.
- It is not always present as a distinct anatomical structure but becomes prominent when distended with stones.
Peritoneal Relations
- The gallbladder is not completely covered by peritoneum.
- The fundus is completely invested by peritoneum.
- The body is covered by peritoneum on its inferior and lateral surfaces only (the superior surface is attached to the liver via the cystic plate - loose areolar tissue).
- The gallbladder is therefore considered a retroperitoneal or, more accurately, a secondarily retroperitoneal/subperitoneal organ attached to the liver.
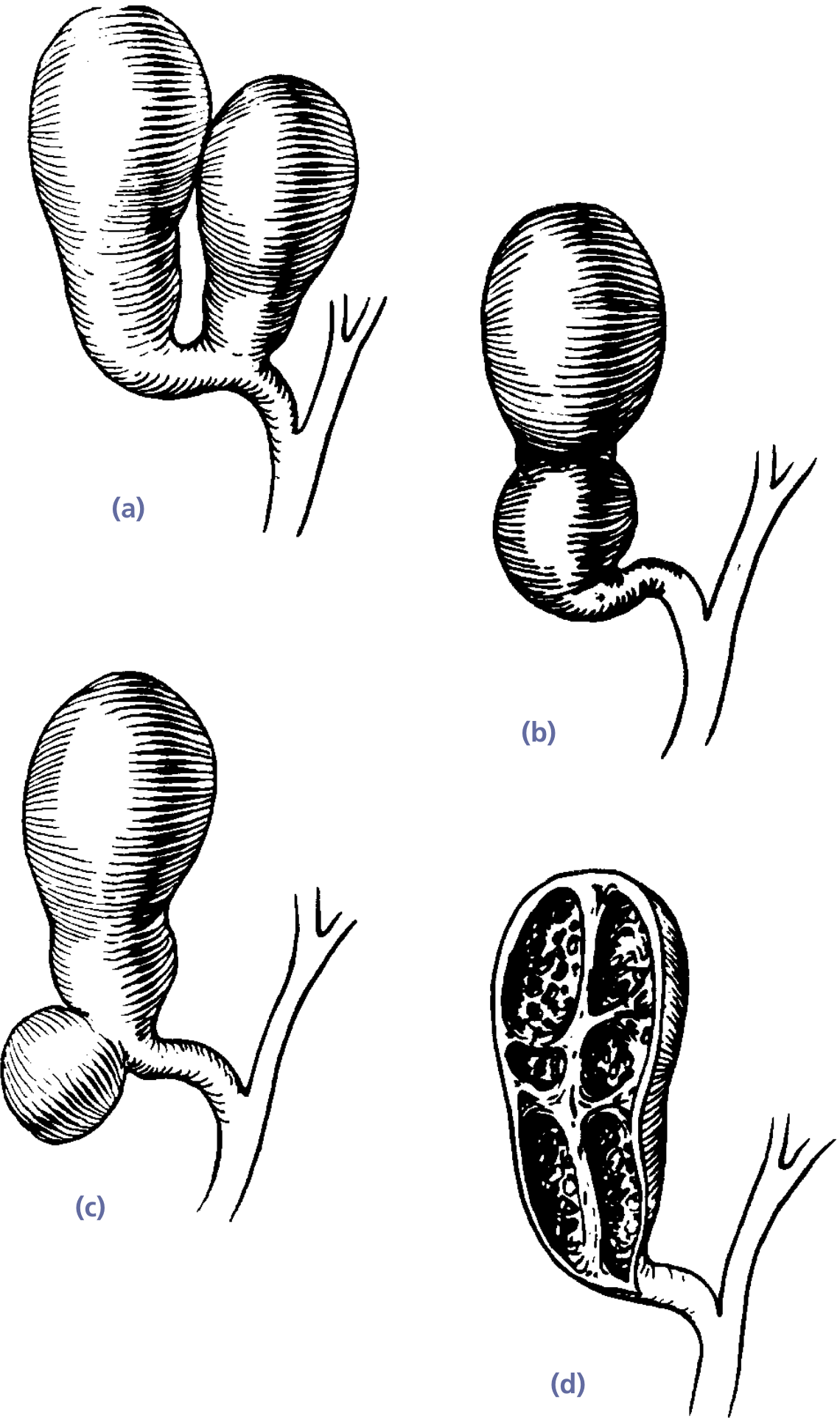
Variations in Peritoneal Covering and Congenital Anomalies:
- Intrahepatic gallbladder: Partially or completely embedded in the liver substance. More prone to difficulties during cholecystectomy.
- "Floating" or "Wandering" gallbladder: Completely covered by peritoneum and suspended by a mesentery (mesentery of the gallbladder). This predisposes to gallbladder torsion (volvulus).
- Left-sided gallbladder: Rare anomaly; gallbladder located in the left hepatic fossa (associated with situs inversus or independently).
- Agenesis: Rare congenital absence.
- Duplication: Two separate gallbladders with two cystic ducts.
- Phrygian cap: A fold in the fundus of the gallbladder - usually an incidental finding of no clinical significance.
- Multiseptate gallbladder: Multiple septa within the gallbladder; may predispose to gallstone formation.
- Gallbladder diverticulum (Rokitansky-Aschoff sinuses): Outpouchings of the mucosa through the muscular wall; seen in chronic cholecystitis and adenomyomatosis.
Blood Supply
Arterial Supply
- Cystic artery - the principal arterial supply.
- Usually a single artery arising from the right hepatic artery (in ~70% of cases).
- The cystic artery typically passes behind the common hepatic duct (and sometimes behind the cystic duct) to reach the neck of the gallbladder.
- It divides into a superficial branch (supplies the inferior/free peritoneal surface) and a deep branch (supplies the surface attached to the liver, runs between the gallbladder and the liver bed).
- The cystic artery runs within the cystohepatic triangle (Calot's triangle) - see below.
Variations in the Cystic Artery (Very Important Surgically):
- Double cystic artery (~15-20%): Two cystic arteries, one from the right hepatic artery and one from another source.
- Origin from left hepatic artery, proper hepatic artery, common hepatic artery, gastroduodenal artery, superior mesenteric artery, or even celiac trunk (all rare but documented).
- Caterpillar turn/hump: The right hepatic artery may be tortuous and form a loop (Moynihan's hump) that closely mimics the cystic artery, leading to inadvertent ligation during cholecystectomy.
- An accessory cystic artery may be present.
- The cystic artery may pass anterior to the common hepatic duct (in ~25% of cases) instead of posterior.
CLINICAL: Cystic Artery Hemorrhage
- Injury to the cystic artery during cholecystectomy can cause significant hemorrhage. The critical view of safety (CVS) technique (see below) helps identify the cystic artery correctly.
- If the right hepatic artery is mistakenly clipped instead of the cystic artery, it can cause right hepatic lobe ischemia/necrosis.
Venous Drainage
- Small veins (cystic veins) drain directly into the liver through the gallbladder bed (the venous drainage of the gallbladder bed goes directly into the hepatic sinusoids of segments IV and V - this is why gallbladder carcinoma tends to metastasize to the liver early).
- A small cystic vein may also drain into the right branch of the portal vein or directly into the portal vein.
CLINICAL: Gallbladder Carcinoma and Liver Metastasis
- Because of the direct venous drainage into the liver bed (segments IV and V), carcinoma of the gallbladder metastasizes early to these segments. Radical cholecystectomy for gallbladder cancer includes resection of the gallbladder bed (segments IVb and V) with regional lymphadenectomy.
Lymphatic Drainage
- Cystic lymph node (node of Lund/Calot's node): Located in the cystohepatic triangle (Calot's triangle), near the junction of the cystic duct and common hepatic duct. This is the sentinel lymph node of the gallbladder.
- From the cystic node → hepatic nodes along the hepatic artery → celiac nodes → cisterna chyli.
- Some lymphatics from the gallbladder also pass directly to hepatic nodes in the porta hepatis.
- Lymphatics from the body and fundus may also drain through the liver bed into the hepatic lymphatics.
Nerve Supply
- Sympathetic: From the celiac plexus (T7-T9 spinal segments) via the hepatic plexus. Primarily vasomotor and conveys visceral pain.
- Parasympathetic: From the vagus nerve (mainly the hepatic branch of the anterior vagal trunk). Stimulates contraction and secretion.
- Sensory/Pain: Visceral afferents travel with the sympathetic fibers through the greater splanchnic nerve to spinal cord segments T7-T9 (primarily the right side).
CLINICAL: Referred Pain of Gallbladder Disease
- Right hypochondrium/epigastrium: Visceral pain from gallbladder distension or inflammation (T7-T9 dermatomes).
- Right shoulder tip/scapular region: Referred pain via the phrenic nerve (C3, C4, C5). This occurs when the inflamed gallbladder or subdiaphragmatic bile irritates the diaphragmatic peritoneum (supplied by the phrenic nerve). The pain is referred to the shoulder tip (supraclavicular region, C3-C5 dermatome) - known as Kehr's sign (more commonly used for splenic rupture but applicable to any diaphragmatic irritation).
- Boas' sign: Hyperesthesia (increased sensitivity) in the area just below the right scapula, in acute cholecystitis - related to the T7-T9 dermatome.
Histology (Brief, Relevant to Clinical Anatomy)
- Mucosa: Columnar epithelium with extensive folds (rugae). No muscularis mucosae or submucosa (unlike the rest of the GI tract). This is why gallbladder carcinoma (which is usually adenocarcinoma) invades the muscular layer and serosa early - there's no submucosal barrier.
- Muscular layer: Smooth muscle fibers in irregular bundles (not organized into distinct circular/longitudinal layers).
- Perimuscular connective tissue (subserosa)
- Serosa (peritoneum): Only on the free surface.
Function
- Storage of bile (between meals)
- Concentration of bile (5-10 fold, by absorption of water, sodium, and chloride)
- Acidification of bile
- Secretion of mucus (mainly by the neck glands)
- Ejection of bile into the duodenum in response to cholecystokinin (CCK), released from I-cells of the duodenal and jejunal mucosa when fat and protein enter the duodenum.
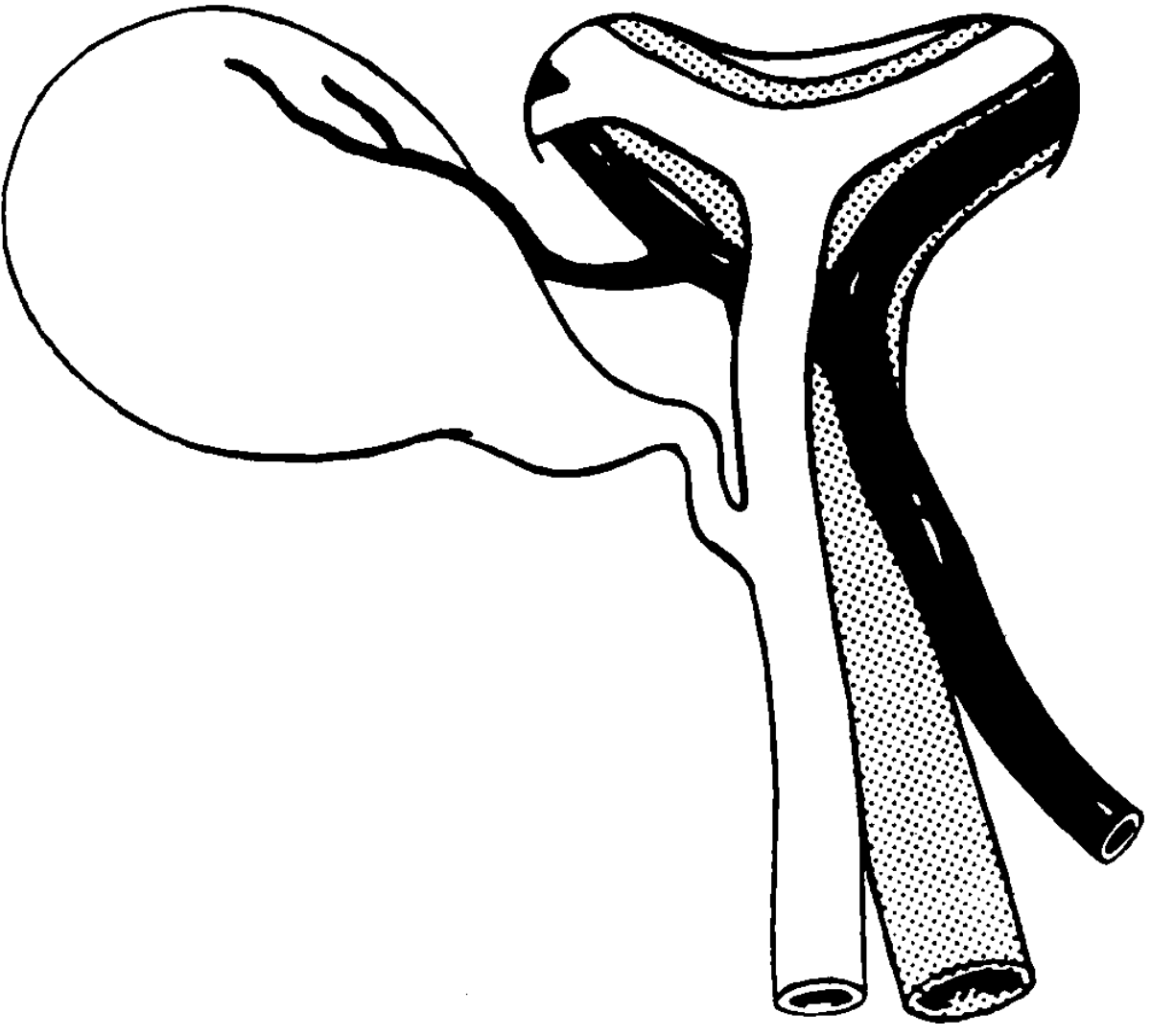
4. CYSTIC DUCT
Description
- Connects the neck of the gallbladder to the common hepatic duct to form the common bile duct.
- Length: Approximately 2-4 cm (highly variable - one of the most variable structures in the body).
- Diameter: Approximately 1-3 mm.
Course
- Runs posteriorly, inferiorly, and to the left from the gallbladder neck.
- Usually joins the right side of the common hepatic duct at an acute angle.
- Runs within or along the free edge of the hepatoduodenal ligament.
Spiral Valve of Heister
- The cystic duct contains mucosal folds arranged in a spiral pattern (5-12 crescentic folds).
- These are not true valves but rather permanent mucosal ridges that keep the lumen patent and regulate the flow of bile into and out of the gallbladder.
- They prevent sudden distension or collapse of the cystic duct.
- They make catheterization of the cystic duct difficult during intraoperative cholangiography.
Variations in the Cystic Duct (Extremely Important Surgically)
- Angular junction (most common, ~75%): Joins the right side of the CHD at an acute angle.
- Parallel (spiral) course: The cystic duct runs parallel to the CHD for a variable distance before joining it (sometimes bound together by connective tissue). This can lead to misidentification of the CHD as the cystic duct.
- Low insertion: Cystic duct joins the CHD very low, near the duodenum or even behind the pancreas. The parallel course variant may have a very low junction.
- High insertion: Cystic duct joins the right hepatic duct (instead of the CHD).
- Medial insertion: Cystic duct crosses anterior or posterior to the CHD and joins its left side.
- Absent cystic duct: Gallbladder opens directly into the CHD (very rare, increases risk of bile duct injury).
- Very short cystic duct: Functionally similar to absent cystic duct.
- Very long cystic duct: May extend to the retroduodenal portion of the CBD.
- Double cystic duct: Rare.
- Cystic duct joining the right hepatic duct or a segmental duct.
CLINICAL: Bile Duct Injury During Cholecystectomy
- The most common cause of bile duct injury during laparoscopic cholecystectomy is misidentification of the CBD as the cystic duct, especially when the cystic duct runs parallel to the CHD or when there is a short cystic duct.
- The "Critical View of Safety" (CVS) (Strasberg's technique) is the gold standard method to prevent bile duct injury:
- The hepatocystic triangle (Calot's triangle) is cleared of fat and fibrous tissue.
- The lower end of the gallbladder is dissected off the liver bed (cystic plate).
- Two and only two structures should be seen entering the gallbladder: the cystic duct and the cystic artery.
- Only then should these structures be clipped and divided.
- Bile duct injuries are classified by the Strasberg classification (A-E) or the Bismuth classification (for strictures):
- Strasberg A: Leak from cystic duct stump or minor hepatic duct (duct of Luschka)
- Strasberg B: Occlusion of an aberrant right hepatic duct
- Strasberg C: Transection of an aberrant right hepatic duct
- Strasberg D: Lateral injury to the CBD
- Strasberg E: Further subdivided (E1-E5) corresponding to the Bismuth classification for strictures
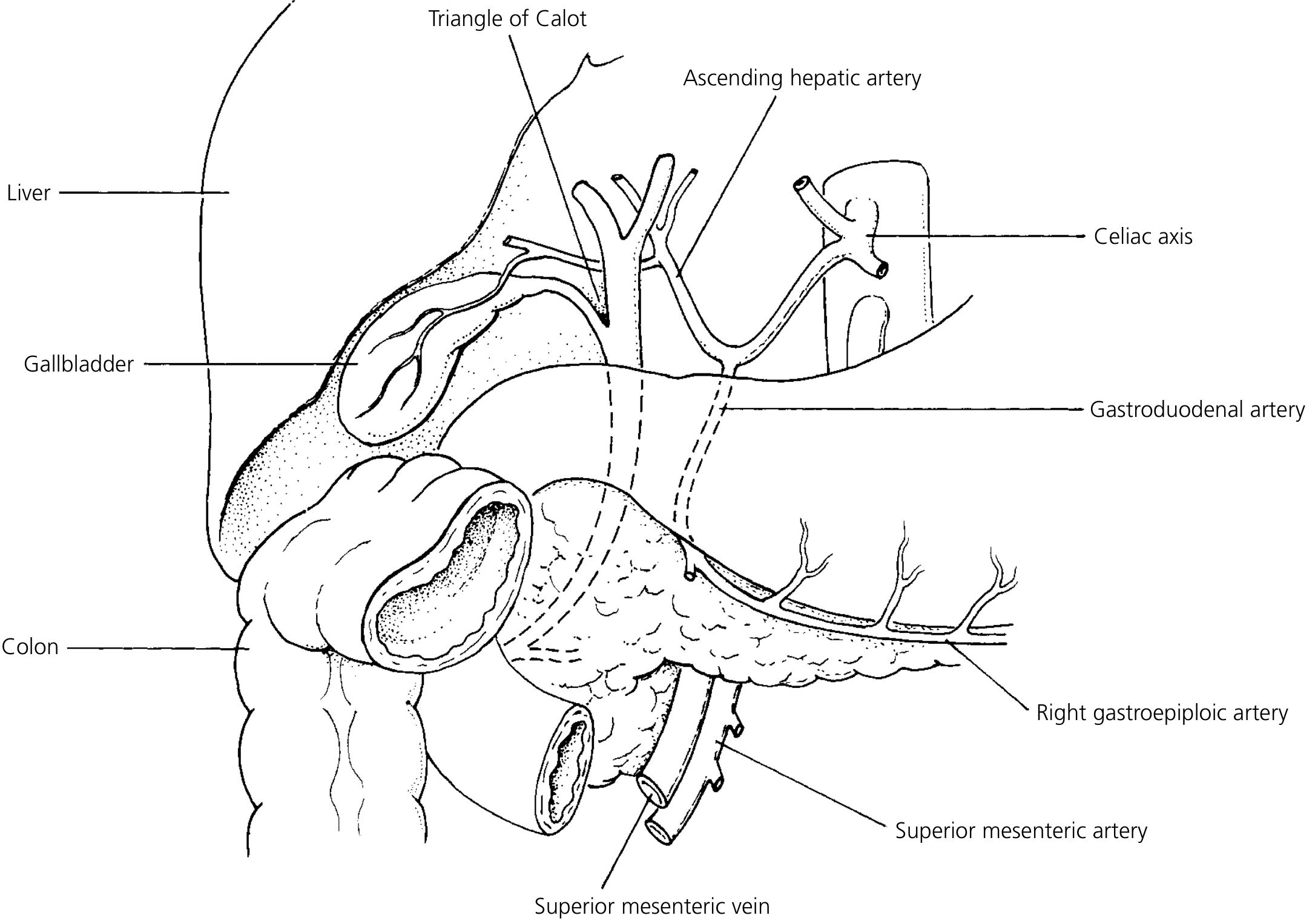
5. CALOT'S TRIANGLE (CYSTOHEPATIC TRIANGLE / HEPATOBILIARY TRIANGLE)
Definition
-
Originally described by Jean-François Calot (1891): The triangle bounded by:
- Cystic duct (inferiorly)
- Common hepatic duct (medially)
- Cystic artery (superiorly)
-
Modern/surgical definition (Hepatocystic triangle): More commonly used today:
- Cystic duct (inferiorly)
- Common hepatic duct (medially)
- Inferior surface of the liver (visceral surface of segment V) (superiorly)
Contents of Calot's Triangle
- Cystic artery (and its branches)
- Cystic lymph node (of Lund/Calot's node)
- Connective tissue, fat, and lymphatics
- Occasionally: Right hepatic artery (if it takes an abnormal course), accessory hepatic duct, or an aberrant right hepatic duct
CLINICAL: Significance of Calot's Triangle
- This is the primary area of dissection during cholecystectomy.
- All the dangerous structures that can be inadvertently injured are in or near this triangle.
- The cystic artery usually crosses this triangle (in most cases posterior to the common hepatic duct, then crossing to the right toward the gallbladder).
- The right hepatic artery frequently courses through or near the triangle - misidentification and ligation of this artery is a serious complication.
- Calot's node is the first node to be involved in gallbladder malignancy and can be biopsied intraoperatively.
6. COMMON BILE DUCT (CBD) / DUCTUS CHOLEDOCHUS
Formation
- Formed by the union of the common hepatic duct and the cystic duct.
- The junction typically occurs at the level of the first part of the duodenum or slightly above, but this is highly variable.
Length
- Approximately 7-8 cm (range 5-15 cm, depending on where the cystic duct joins).
Diameter
- Approximately 6-8 mm.
- Normal ultrasound: ≤6 mm (≤8 mm after cholecystectomy; increases with age: add 1 mm per decade after 60 years).
- A CBD diameter >8 mm (or >10 mm post-cholecystectomy) is considered dilated and suggests obstruction.
Course and Parts
a) Supraduodenal Part
- Length: ~2-4 cm
- Runs in the free edge of the hepatoduodenal ligament (lesser omentum).
- Lies to the right and anterior to the portal vein.
- Lies to the right of the proper hepatic artery.
- This is the most accessible part surgically.
- This is where choledochotomy (surgical incision into the CBD) is performed for CBD exploration and stone extraction.
b) Retroduodenal Part
- Length: ~1-2 cm
- Passes behind the first part of the duodenum (superior/first part of the duodenum).
- Still accompanied by the portal vein (posteriorly) and the gastroduodenal artery (to its left, which is now anterior to the portal vein).
- The gastroduodenal artery crosses anterior to the CBD here.
c) Infraduodenal (Pancreatic/Retropancreatic) Part
- Length: ~3 cm
- Runs behind the head of the pancreas or is embedded within the posterior aspect of the pancreatic head, in a groove on its posterior surface.
- This is the longest part.
- Closely related to the main pancreatic duct (of Wirsung), which runs from left to right through the pancreas and approaches the CBD from the left.
- The CBD and main pancreatic duct converge as they approach the duodenal wall.
CLINICAL: Carcinoma of the Head of the Pancreas
- Tumors of the pancreatic head (most commonly ductal adenocarcinoma) compress or obstruct the intrapancreatic portion of the CBD, causing:
- Painless, progressive obstructive jaundice (the classic presentation)
- Courvoisier's law/sign: "In the presence of jaundice, a palpable gallbladder is unlikely to be due to gallstones." Rationale: In gallstone disease, the gallbladder wall is fibrosed from chronic inflammation and cannot distend. In malignant obstruction (pancreatic head tumor), the obstruction is gradual, and the gallbladder wall is normal, so it distends.
- Exceptions to Courvoisier's law: Double impaction of stones (one in cystic duct, one in CBD), a stone in Hartmann's pouch with a separate stone in CBD, or mucocele of the gallbladder.
- Pale/clay-colored stools (acholic stools): Due to absence of bile pigments in the gut.
- Dark urine (tea/cola-colored): Due to conjugated bilirubin in urine.
- Steatorrhea: Due to absence of bile salts in the gut (fat malabsorption).
- Pruritus: Due to deposition of bile salts in the skin.
- Coagulopathy: Due to malabsorption of fat-soluble vitamin K.
d) Intraduodenal (Intramural) Part
- Length: ~1.5-2 cm
- The CBD passes obliquely through the posteromedial wall of the second part (descending part) of the duodenum.
- Runs obliquely through the duodenal wall for ~2 cm - this oblique course creates a valve-like mechanism that prevents duodenal reflux into the biliary system.
- Usually joins the main pancreatic duct (of Wirsung) to form the hepatopancreatic ampulla (ampulla of Vater).
- Opens at the major duodenal papilla on the posteromedial wall of the second part of the duodenum, approximately at the junction of the middle and lower thirds of the second part, about 8-10 cm distal to the pylorus.
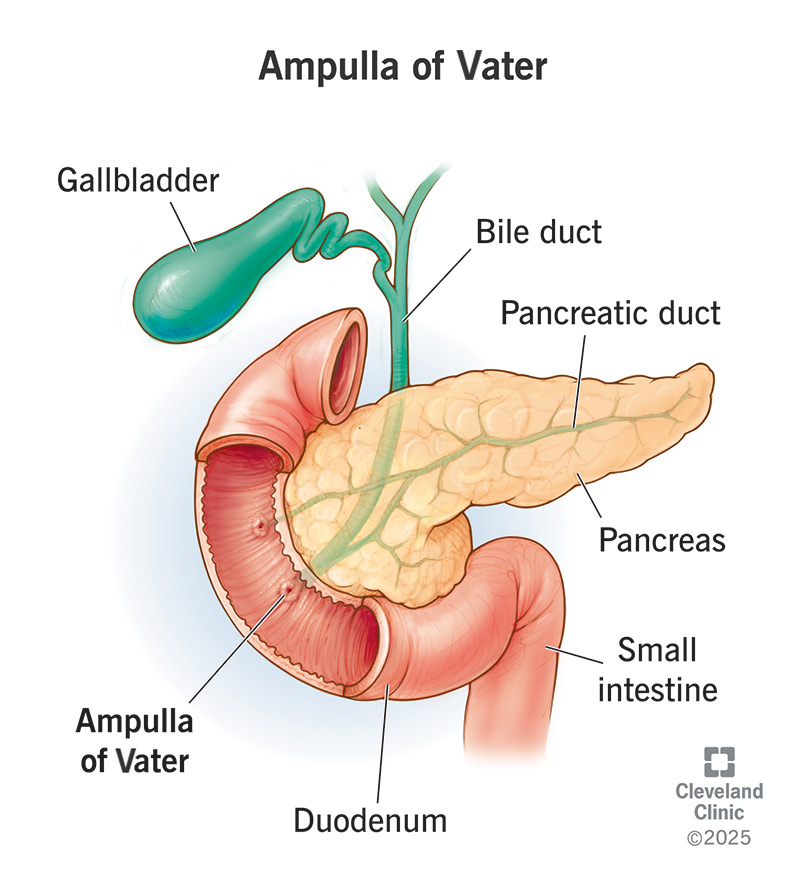
7. HEPATOPANCREATIC AMPULLA (AMPULLA OF VATER) AND SPHINCTER OF ODDI
Hepatopancreatic Ampulla
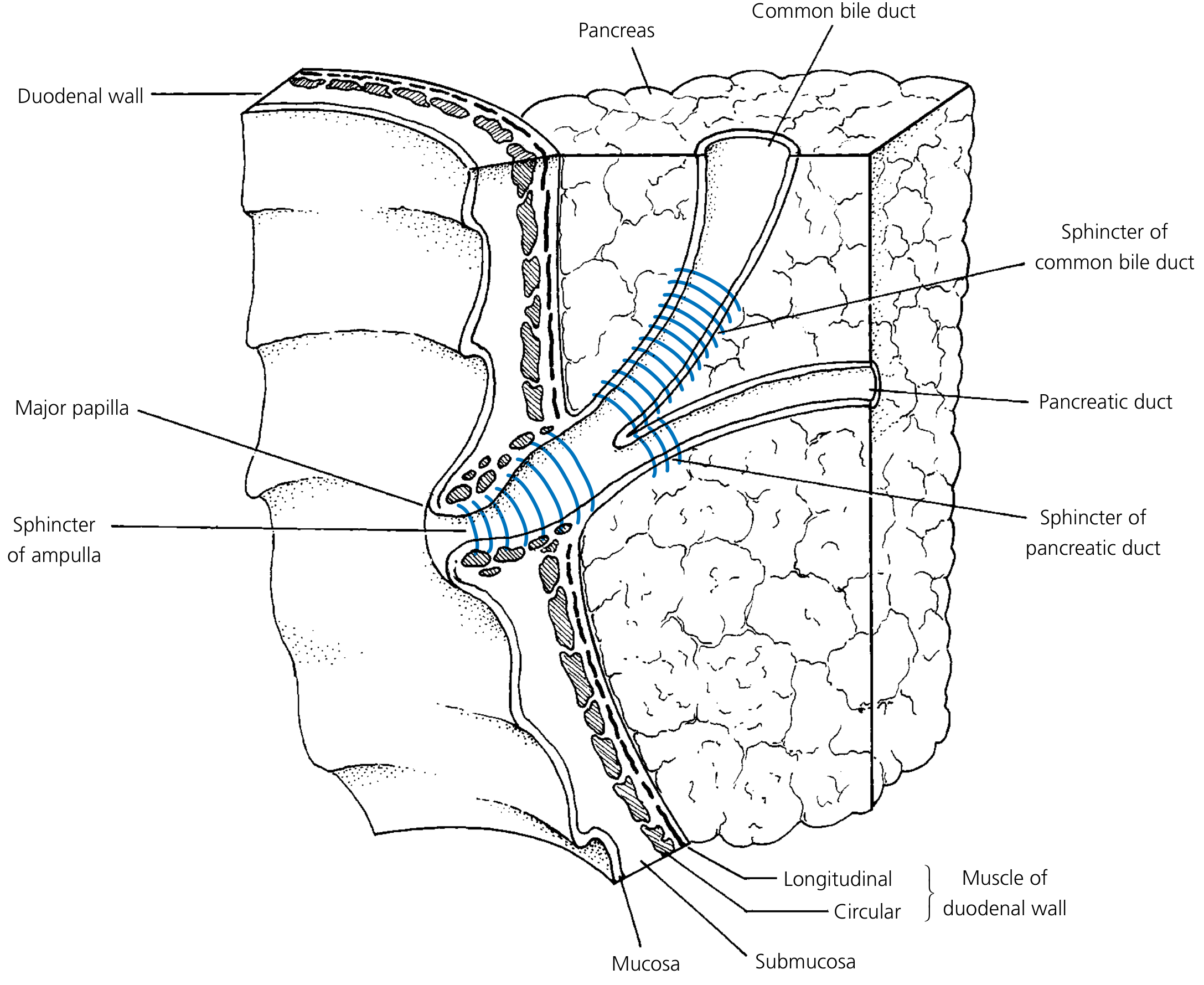
- The dilated terminal portion formed by the union of the CBD and the main pancreatic duct.
- Length: Approximately 1-14 mm (variable).
- Opens at the summit of the major duodenal papilla.
Variations in CBD-Pancreatic Duct Junction
- Type 1 (Most common, ~60-70%): CBD and main pancreatic duct unite before entering the duodenal wall, forming a common channel (the ampulla of Vater).
- Type 2 (~20-30%): CBD and main pancreatic duct enter the duodenum separately through separate openings on the major papilla, with no true ampulla.
- Type 3 (~5%): CBD and main pancreatic duct unite within the duodenal wall with a very short common channel.
CLINICAL: Anomalous Pancreaticobiliary Junction (APBJ)
- When the junction of the CBD and pancreatic duct occurs outside the duodenal wall (long common channel >15 mm), the sphincter of Oddi cannot regulate the reflux of pancreatic juice into the biliary system.
- This leads to chronic reflux of pancreatic enzymes into the biliary tree, causing:
- Choledochal cysts (especially Type I and Type IV)
- Increased risk of gallbladder carcinoma and bile duct carcinoma
- This is especially common in Asian populations and in children with choledochal cysts.
Sphincter of Oddi (Sphincter of the Hepatopancreatic Ampulla)
- Sphincter choledochus (sphincter of the bile duct): Surrounds the terminal intramural portion of the CBD. This is the most important sphincter - it controls bile flow.
- Sphincter pancreaticus: Surrounds the terminal portion of the main pancreatic duct (weaker and less constant than the sphincter choledochus).
- Sphincter ampullae (of the hepatopancreatic ampulla): Surrounds the common channel/ampulla itself.
Functions of the Sphincter of Oddi
- Regulates bile flow into the duodenum
- Prevents reflux of duodenal contents into the biliary and pancreatic systems
- Prevents reflux of pancreatic juice into the biliary system (and vice versa)
- Controls filling of the gallbladder: When the sphincter is closed (between meals), bile backs up and fills the gallbladder via the cystic duct.
- Relaxation is primarily mediated by CCK (cholecystokinin), which simultaneously causes gallbladder contraction and sphincter relaxation, allowing bile to flow into the duodenum.
CLINICAL: Sphincter of Oddi Dysfunction (SOD)
- Functional disorder causing biliary-type pain, elevated liver enzymes, and/or recurrent pancreatitis without organic obstruction.
- Classified into Type I, II, and III (Milwaukee classification) based on clinical, laboratory, and imaging criteria.
- Diagnosed by sphincter of Oddi manometry (gold standard).
- Treated by endoscopic sphincterotomy.
Major Duodenal Papilla
- The elevation on the posteromedial wall of the second part of the duodenum where the ampulla of Vater opens.
- Located approximately 8-10 cm from the pylorus.
- A mucosal fold called the plica longitudinalis duodeni (longitudinal fold of the duodenum) extends vertically along the posteromedial wall of the duodenum, with the major papilla at its lower end.
- A hooded fold (plica) may cover the papilla superiorly.
Minor Duodenal Papilla
- Located approximately 2 cm proximal (superior) to the major papilla.
- This is where the accessory pancreatic duct (of Santorini) opens.
- The minor papilla has a separate, smaller sphincter (sphincter of Helly).
CLINICAL: ERCP (Endoscopic Retrograde Cholangiopancreatography)
- The major duodenal papilla is the target of ERCP, where an endoscope is passed through the mouth, esophagus, stomach, and into the second part of the duodenum. A catheter is then inserted into the papilla, and contrast is injected to visualize the biliary and pancreatic ducts.
- Endoscopic sphincterotomy: The sphincter of Oddi is cut (usually at the 11-12 o'clock position to avoid the pancreatic duct, which lies at 4-5 o'clock) to facilitate stone extraction or stent placement.
- Complications of ERCP: Post-ERCP pancreatitis (most common, 3-5%), hemorrhage, perforation, cholangitis.
CLINICAL: Gallstone Impaction at the Ampulla
- Gallstones passing through the CBD can impact at the ampulla of Vater, causing:
- Obstructive jaundice
- Acute pancreatitis (gallstone pancreatitis - the most common cause of acute pancreatitis in many populations). The stone blocks the common channel, causing reflux of bile into the pancreatic duct, or it blocks the pancreatic duct outflow directly.
- Cholangitis (Charcot's triad: fever with rigors, jaundice, right upper quadrant pain)
- Reynold's pentad: Charcot's triad + hypotension + altered mental status (indicating septic/suppurative cholangitis - a surgical emergency requiring urgent biliary decompression)
8. ACCESSORY PANCREATIC DUCT (OF SANTORINI)
- Opens at the minor duodenal papilla.
- Drains the uncinate process and part of the head of the pancreas.
- In approximately 10% of people, it is the dominant (main) drainage pathway (this is called pancreas divisum).
CLINICAL: Pancreas Divisum
- The most common congenital anomaly of the pancreas (~5-10% of the population).
- The dorsal and ventral pancreatic ducts fail to fuse during embryological development.
- The majority of the pancreas (body and tail from the dorsal bud) drains through the minor papilla via the accessory duct, while only the uncinate process (from the ventral bud) drains through the major papilla via the main duct.
- May predispose to recurrent pancreatitis if the minor papilla orifice is too small to handle the increased flow.
9. ARTERIAL SUPPLY OF THE EXTRAHEPATIC BILIARY SYSTEM
Overview
Sources
- Cystic artery → supplies the gallbladder and upper portion of the cystic duct.
- Right hepatic artery → supplies the common hepatic duct and upper part of the CBD (supraduodenal part).
- Posterior superior pancreaticoduodenal artery (branch of gastroduodenal artery) and retroduodenal artery → supply the retroduodenal and pancreatic portions of the CBD.
- Gastroduodenal artery → contributes to the retroduodenal portion.
Marginal Arteries (of the Bile Duct)
- The bile ducts receive their blood supply from two axial vessels running along the bile duct:
- 3 o'clock artery (lateral marginal artery)
- 9 o'clock artery (medial marginal artery)
- These are small arteries that run along the lateral (right) and medial (left) borders of the CBD/CHD.
- They form a periductal vascular plexus (epicholedochal plexus) around the bile duct.
Blood Supply Pattern
- 60% of the blood supply to the supraduodenal CBD comes from below (retroduodenal artery/gastroduodenal artery) and travels upward.
- 38% comes from above (right hepatic artery/cystic artery).
- Only 2% is from non-axial sources.
CLINICAL: Bile Duct Ischemia and Stricture
- The supraduodenal CBD is particularly vulnerable to ischemia because it depends on axial blood supply from small marginal arteries.
- Excessive dissection, cautery, or skeletonization of the bile duct during surgery can damage the 3 o'clock and 9 o'clock arteries, leading to:
- Ischemic bile duct stricture (a devastating complication)
- Bile duct necrosis and leak
- During liver transplantation, the blood supply to the donor bile duct is entirely dependent on axial vessels from below (the hepatic artery). If the hepatic artery thromboses, the bile duct becomes ischemic, leading to ischemic-type biliary lesions (ITBL) and anastomotic strictures.
10. VENOUS DRAINAGE OF THE EXTRAHEPATIC BILIARY SYSTEM
- Veins from the bile ducts drain into the portal venous system:
- Upper bile duct veins → portal vein branches
- Lower bile duct veins → posterior superior pancreaticoduodenal vein → portal vein
- Gallbladder veins: Drain directly into the liver bed (hepatic sinusoids of segments IV and V) or via small cystic veins into the portal vein.
11. LYMPHATIC DRAINAGE OF THE EXTRAHEPATIC BILIARY SYSTEM
- Cystic lymph node (of Lund): First node; lies in Calot's triangle.
- Pericholedochal nodes: Along the CBD.
- Hilar nodes (hepatic nodes): At the porta hepatis.
- Nodes along the common hepatic artery.
- Retropancreatic and retroduodenal nodes.
- Celiac nodes.
- Para-aortic (interaortocaval) nodes.
- Ultimately → Cisterna chyli → Thoracic duct.
CLINICAL: Nodal Staging in Gallbladder and Bile Duct Cancer
- Regional lymph node involvement significantly affects staging and prognosis.
- For gallbladder carcinoma, N1 nodes include: cystic duct node, pericholedochal, hilar, periportal, and proper hepatic artery nodes.
- N2 nodes include: celiac, periaortic, pericaval, and superior mesenteric artery nodes.
12. NERVE SUPPLY OF THE EXTRAHEPATIC BILIARY SYSTEM
Sympathetic
- From the celiac plexus (greater splanchnic nerve, T5-T9, primarily T7-T9).
- Vasomotor function.
- Conveys visceral pain afferents.
Parasympathetic
- From the vagus nerve (hepatic branch of the anterior vagal trunk).
- Stimulates gallbladder contraction and bile secretion.
- Relaxation of the sphincter of Oddi (although CCK is the primary regulator).
Sensory/Pain Pathway
- Visceral afferents travel with the sympathetic fibers (greater splanchnic nerve) to the spinal cord segments T5-T9.
- Dermatomes T7-T9: Right hypochondrium, epigastrium.
- Referred pain: Right shoulder tip (C3-C5, phrenic nerve) when the diaphragm is irritated by biliary pathology.
CLINICAL: Biliary Colic
- The pain of biliary colic is visceral in nature: poorly localized, deep, and typically felt in the epigastrium or right hypochondrium.
- It is caused by gallbladder contraction against an obstructed cystic duct (usually by a gallstone).
- Despite the name "colic," the pain is usually constant (not true colicky/intermittent) and lasts 1-5 hours.
- It is NOT worsened by movement (unlike peritonitis).
- The pain may radiate to the right scapular region (referred pain via T7-T9 dermatomes) or the right shoulder tip (phrenic nerve involvement if there is diaphragmatic irritation).
13. EMBRYOLOGY (Brief, Clinically Relevant)
- The extrahepatic biliary apparatus develops from the hepatic diverticulum (liver bud), an outgrowth of the ventral wall of the foregut (future duodenum) during the 4th week of development.
- The hepatic diverticulum divides into:
- Cranial part (pars hepatica): Gives rise to the liver parenchyma and intrahepatic bile ducts.
- Caudal part (pars cystica): Gives rise to the gallbladder and cystic duct.
- The stalk of the hepatic diverticulum becomes the common bile duct.
- The connection to the duodenum (common hepatic duct) develops from the stalk above the cystic duct origin.
CLINICAL: Biliary Atresia
- Failure of normal development or destruction of the extrahepatic bile ducts, either during fetal life or shortly after birth.
- The most common cause of neonatal obstructive jaundice requiring surgery.
- Presents with conjugated (direct) hyperbilirubinemia, pale stools, dark urine, and hepatomegaly in the neonate.
- Kasai procedure (hepatoportoenterostomy): A Roux-en-Y loop of jejunum is anastomosed to the porta hepatis to allow bile drainage. Must be performed before 8 weeks of age for the best outcome.
- If Kasai fails → liver transplantation (biliary atresia is the most common indication for pediatric liver transplantation).
CLINICAL: Choledochal Cysts
- Congenital cystic dilatations of the biliary tree.
- Todani classification:
- Type I (most common, ~50-80%): Fusiform (Ia), focal (Ib), or diffuse (Ic) dilatation of the CBD.
- Type II: True diverticulum of the CBD.
- Type III (Choledochocele): Dilatation of the intraduodenal portion of the CBD.
- Type IV: Multiple cysts:
- IVa (2nd most common): Both intrahepatic and extrahepatic cysts.
- IVb: Multiple extrahepatic cysts only.
- Type V (Caroli disease): Multiple intrahepatic cysts (strictly not extrahepatic, but included in the classification).
- Associated with anomalous pancreaticobiliary junction (APBJ) in up to 90% of cases.
- Risk of cholangiocarcinoma (10-30% lifetime risk) if untreated.
- Treatment: Complete excision of the cyst with Roux-en-Y hepaticojejunostomy (for Types I and IV). Type III (choledochocele) may be treated by endoscopic sphincterotomy.
14. APPLIED ANATOMY & ADDITIONAL CLINICAL CORRELATIONS
Cholecystectomy (Surgical Removal of the Gallbladder)
Laparoscopic Cholecystectomy (Gold Standard)
- Port placement: Usually 4 ports (American technique) or 3 ports (French technique).
- Dissection proceeds in Calot's triangle.
- Critical View of Safety (CVS): As described above - the most important step to prevent bile duct injury.
- Intraoperative cholangiography (IOC): A catheter is placed in the cystic duct, and contrast is injected under fluoroscopy to delineate the biliary anatomy and detect CBD stones.
- "Fundus first" or "Top-down" cholecystectomy: Used when the anatomy in Calot's triangle is unclear (e.g., severe inflammation in acute cholecystitis). The gallbladder is dissected from the liver bed starting at the fundus, progressing toward the neck.
- Subtotal cholecystectomy: In cases of severe inflammation where safe dissection of Calot's triangle is impossible, the fundus and body are removed, but the posterior wall of the gallbladder (attached to the liver) or the Hartmann's pouch area is left in situ with the cystic duct stump secured from inside (reconstituting technique) or left open with a drain (fenestrating technique).
Open Cholecystectomy
- Performed through a right subcostal (Kocher's) incision or a right paramedian incision.
- May be necessary in cases of severe inflammation, suspected gallbladder cancer, or inability to complete laparoscopic surgery.
Cholecystostomy
- Percutaneous or surgical placement of a drain into the gallbladder for decompression.
- Used in critically ill patients with acute cholecystitis who are unfit for cholecystectomy.
- Percutaneous cholecystostomy is image-guided (ultrasound or CT).
CBD Exploration
- Performed when CBD stones are suspected or confirmed.
- Supraduodenal choledochotomy: An incision is made in the anterior wall of the supraduodenal CBD (the most accessible part). Stones are extracted using forceps, balloon catheters, or choledochoscopy.
- The choledochotomy may be closed primarily over a T-tube (to decompose and allow post-operative cholangiography) or closed primarily without a T-tube (if the duct is of adequate diameter and the papilla is patent).
Choledochoduodenostomy and Choledochojejunostomy
- Choledochoduodenostomy: Anastomosis between the CBD and the duodenum (for recurrent CBD stones, failed ERCP, or distal CBD obstruction).
- Choledochojejunostomy (Roux-en-Y hepaticojejunostomy): Anastomosis between the CBD (or CHD or hepatic ducts) and a Roux-en-Y loop of jejunum. Used for benign and malignant bile duct strictures, bile duct injuries, choledochal cysts, and after Whipple's procedure (pancreaticoduodenectomy).
Whipple's Procedure (Pancreaticoduodenectomy)
- Performed for periampullary carcinoma (pancreatic head, ampulla of Vater, distal CBD, or duodenum).
- Involves resection of the head of the pancreas, duodenum, distal CBD, gallbladder, and distal stomach (in classic Whipple) or pylorus preservation (in pylorus-preserving Whipple/PPPD).
- Reconstruction involves:
- Pancreaticojejunostomy (or pancreaticogastrostomy)
- Hepaticojejunostomy (bile duct-jejunum anastomosis)
- Gastrojejunostomy (or duodenojejunostomy in PPPD)
Courvoisier's Gallbladder (Reiterated)
- A palpable, non-tender, distended gallbladder in a jaundiced patient suggests malignant obstruction of the CBD (e.g., pancreatic head carcinoma, periampullary carcinoma, cholangiocarcinoma of the distal CBD).
Charcot's Triad and Reynold's Pentad (Reiterated)
- Charcot's triad (acute cholangitis): Fever + Jaundice + Right upper quadrant pain.
- Reynold's pentad (suppurative cholangitis): Charcot's triad + Hypotension + Altered mental status.
- Requires urgent biliary decompression (ERCP with sphincterotomy and stenting, or percutaneous transhepatic biliary drainage).
Gallstone Types
- Cholesterol stones (~80% in Western countries): Yellow-green, occur in supersaturated bile.
- Pigment stones:
- Black pigment stones: Associated with hemolytic conditions (e.g., sickle cell disease, hereditary spherocytosis), cirrhosis. Found in the gallbladder.
- Brown pigment stones: Associated with biliary infections and stasis (especially in Asian populations). Found in the bile ducts (primary choledocholithiasis).
- Mixed stones: Most common overall.
Risk Factors for Gallstones ("6 F's")
- Female
- Fat (obese)
- Forty (age >40)
- Fertile (multiparity)
- Fair (Caucasian, Native American, Hispanic)
- (Family history)
Additional: Porcelain Gallbladder
- Calcification of the gallbladder wall.
- Previously thought to have a very high risk of gallbladder carcinoma (historically quoted as ~25%), but recent studies suggest the risk may be lower (~5-7%).
- Nevertheless, prophylactic cholecystectomy is generally recommended.
Additional: Gallbladder Polyps
- Polyps >10 mm have a higher risk of malignancy → cholecystectomy recommended.
- Polyps 6-10 mm: Follow-up with serial ultrasound.
- Polyps <6 mm: Usually cholesterol polyps, benign.
15. SUMMARY OF KEY RELATIONSHIPS
Hepatoduodenal Ligament Contents (Anterior to Posterior)
| Position | Structure |
|---|---|
| Right, anterior | CBD (above) / CHD (below the cystic duct junction) |
| Left, anterior | Proper hepatic artery |
| Posterior, central | Portal vein |
Epiploic Foramen (of Winslow)
- Anterior boundary: Free edge of the hepatoduodenal ligament (containing CBD, hepatic artery, portal vein).
- Posterior boundary: IVC (covered by peritoneum).
- Superior boundary: Caudate lobe of the liver (caudate process).
- Inferior boundary: First part of the duodenum.
- This foramen connects the greater sac with the lesser sac (omental bursa).
- Pringle maneuver is performed by compressing the contents of the hepatoduodenal ligament through the epiploic foramen.
16. IMAGING OF THE BILIARY SYSTEM
Ultrasound (First-line)
- Best initial investigation for gallstones, gallbladder wall thickening, bile duct dilatation.
- Normal CBD ≤6 mm (≤8-10 mm post-cholecystectomy).
- Sonographic Murphy's sign: Focal tenderness over the gallbladder when compressed by the ultrasound probe → acute cholecystitis.
MRCP (Magnetic Resonance Cholangiopancreatography)
- Non-invasive imaging of the biliary tree using heavily T2-weighted MRI sequences.
- Excellent for detecting CBD stones, bile duct strictures, choledochal cysts, and biliary anatomy.
ERCP (Endoscopic Retrograde Cholangiopancreatography)
- Both diagnostic and therapeutic.
- Gold standard for managing CBD stones (sphincterotomy + stone extraction).
- Can place stents for malignant biliary obstruction.
PTC (Percutaneous Transhepatic Cholangiography)
- Needle puncture through the liver into a dilated intrahepatic bile duct, followed by contrast injection.
- Used when ERCP fails or is not possible (e.g., altered surgical anatomy after Roux-en-Y).
EUS (Endoscopic Ultrasound)
- High-resolution imaging of the distal CBD, ampulla, and pancreatic head.
- Excellent sensitivity for small CBD stones (<5 mm) and periampullary tumors.
- Allows FNA (fine needle aspiration) of masses.
HIDA Scan (Hepatobiliary Iminodiacetic Acid Scan)
- Nuclear medicine study using technetium-99m-labeled IDA analogues.
- The radiotracer is taken up by hepatocytes and excreted into the biliary system.
- Non-visualization of the gallbladder within 60 minutes (or 4 hours with morphine augmentation) → acute cholecystitis (cystic duct obstruction).
- Also useful for diagnosing bile leaks, biliary atresia (in neonates), and biliary dyskinesia (by calculating the gallbladder ejection fraction after CCK stimulation - normal >35%).
QUICK REFERENCE: IMAGE GALLERY SUMMARY
| Image | What It Shows | Location in Notes |
|---|---|---|
| Overview: gallbladder, bile duct, pancreatic duct, ampulla of Vater, duodenum | Section Overview |
| Gallbladder + biliary tract relations, Calot's triangle, vascular anatomy | Section 3 (Gallbladder) |
| Hilar anatomy: hepatic duct confluence, Triangle of Calot | Section 2 (CHD) + Section 5 |
| Congenital gallbladder anomalies (double, bilobed, diverticulum, septated) | Section 3 (Peritoneal variants) |
| Sphincter of Oddi apparatus: sphincter choledochus, pancreatic sphincter, sphincter ampullae, major papilla | Section 7 (Ampulla) |