Adenomyosis
Reading File
Finding Sources
Finding Sources
Searching Images
adenomyosis histology uterus
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to provide a thorough answer on adenomyosis.
Adenomyosis
Definition
Adenomyosis is the presence of endometrial glands and/or stroma within the myometrium (uterine wall), with secondary smooth muscle hyperplasia. The ectopic tissue remains in continuity with the endometrium, representing presumed downward invasion of endometrial tissue between smooth muscle fascicles. This distinguishes it from endometriosis, where endometrial tissue is outside the uterus entirely.
— Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 929; Robbins & Kumar Basic Pathology, p. 689
Epidemiology
- Found in 10–88% of hysterectomy specimens (wide range due to variable diagnostic thresholds)
- Occurs in up to 20% of uteri on microscopic examination
- Prevalence ~30% in reproductive-age patients, rising in later reproductive years
- More common in multiparous women
- ~33% are asymptomatic — Grainger & Allison's Diagnostic Radiology, p. 898; Sabiston Textbook of Surgery
Pathogenesis
Not fully understood. Adenomyosis likely shares some pathophysiology with endometriosis. The leading hypothesis is invagination/downward growth of the basalis layer of the endometrium into the myometrium. It frequently coexists with uterine leiomyomata.
Pathology / Morphology
On microscopy: irregular nests of endometrial stroma with or without glands, arranged within the myometrium. The ectopic endometrial tissue induces reactive hypertrophy of the surrounding myometrium, resulting in:
- Enlarged, globular uterus
- Thickened uterine wall
The tissue may respond to hormonal cycling, causing localised haemorrhage.
— Robbins & Kumar Basic Pathology, p. 689
Clinical Features
| Feature | Detail |
|---|---|
| Dysmenorrhea | Secondary, colicky; worsens premenstrually |
| Menorrhagia / menometrorrhagia | Heavy and/or irregular menses |
| Dyspareunia | Pelvic pain with intercourse |
| Pelvic pain | Especially premenstrual |
| Uterine enlargement | Diffuse, globular — found on examination |
| Infertility | Associated but less primary than endometriosis |
Symptoms correlate with the extent and depth of myometrial involvement. Can coexist with endometriosis.
— Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 929
Diagnosis
Definitive diagnosis is histological — traditionally confirmed only after hysterectomy. However, imaging allows pre-operative diagnosis.
Transvaginal Ultrasound (TVUS)
Accuracy 68–86% for diffuse disease; lower accuracy when coexisting fibroids or focal adenomyosis are present.
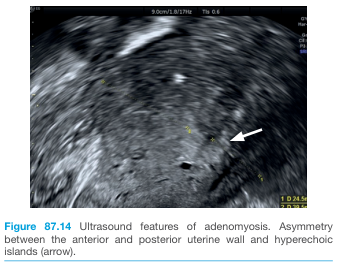
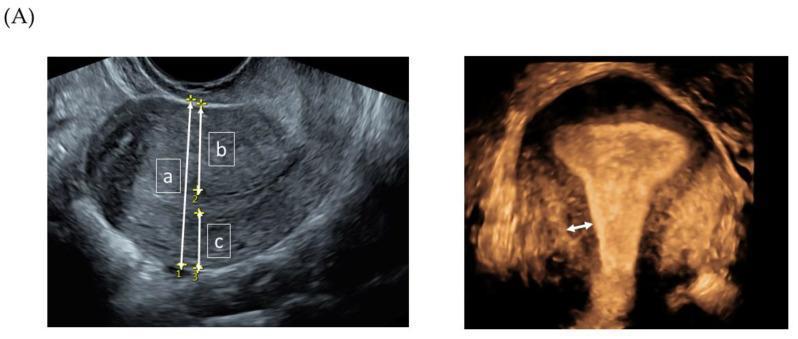
Ultrasound features:
- Enlarged uterus with globular configuration
- Asymmetry of anterior and posterior uterine walls
- Diffuse echogenic nodules and subendometrial echogenic linear striations
- 2–6 mm subendometrial cysts (haemorrhagic foci) in ~50%
- Poor definition of the endomyometrial interface
- "Rain shower" appearance — multiple fine areas of attenuation
- Colour Doppler: speckled pattern of increased vascularity
MRI
MRI is superior for distinguishing adenomyosis from fibroids — clinically important for management planning.
MRI features (T2-weighted):
- Ill-defined areas of low myometrial signal intensity — smooth muscle hyperplasia
- Focal or diffuse thickening of the junctional zone (JZ):
- JZ ≥ 12 mm → predicts adenomyosis with high accuracy
- JZ ≤ 8 mm → excludes adenomyosis with high accuracy
- JZ 8–12 mm → indeterminate; use ancillary criteria
- High T2 signal foci within low-signal myometrium = islands of ectopic endometrial tissue
- High T1 signal foci = punctate haemorrhage within ectopic tissue (95% positive predictive value)
- High T2 linear striations ("finger-like projections") extending from endometrium into myometrium
- Rarely: cystic adenomyosis with high T1 / intermediate-low T2 signal
MRI mimics: myometrial contractions, endometrial carcinoma, fibroids.
— Grainger & Allison's Diagnostic Radiology, p. 898
Management
Management is guided by age, severity of symptoms, and desire for future fertility.
| Approach | Options |
|---|---|
| Analgesia | NSAIDs |
| Hormonal suppression | Combined oral contraceptives, progestins (oral, IM injection, or LNG-IUS), GnRH agonists |
| Minimally invasive | Uterine artery embolization (effective) |
| Definitive | Hysterectomy — guarantees relief of dysmenorrhea; reserved for completed family or treatment failure |
Management follows the same protocol as endometriosis treatment. The levonorgestrel intrauterine system (LNG-IUS) is often first-line for those wishing to preserve the uterus.
— Berek & Novak's Gynecology, p. 581–582
Key Points
- Adenomyosis = endometrial tissue within the myometrium (vs. endometriosis = outside the uterus)
- Classic triad: dysmenorrhea, menorrhagia, enlarged globular uterus
- Histological confirmation remains the gold standard, but MRI with JZ ≥12 mm is highly predictive
- Often coexists with fibroids and endometriosis
- Definitive treatment is hysterectomy; hormonal therapies provide symptom control
This is a shared conversation. Sign in to Orris to start your own chat.