Retinopathy of prematurity
Reading File
Finding Sources
Finding Sources
Searching Images
retinopathy of prematurity fundus staging
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information. Let me compile the full answer.
Retinopathy of Prematurity (ROP)
Definition & Pathophysiology
ROP is a proliferative vasculopathy affecting the developing retina of premature, low-birthweight infants and is one of the leading causes of childhood blindness worldwide.
The retina has no blood vessels until the 4th month of gestation; vascular complexes then grow from optic disc hyaloid vessels toward the periphery. The nasal retina is fully vascularized by ~8 months gestation, but the temporal periphery vascularizes at or up to 1 month after term delivery. Prematurity interrupts this process in two phases:
- Hyperoxic phase (supplemental O₂ in NICU): Retinal vessels undergo vasoconstriction and obliteration — vascular growth is arrested.
- Hypoxic/vasoproliferative phase: The growing, metabolically active avascular retina becomes hypoxic, triggering VEGF-driven abnormal neovascularization at the vascular–avascular junction.
— Kanski's Clinical Ophthalmology, 10e; Harriet Lane Handbook, 23e
Risk Factors
| Major | Additional |
|---|---|
| Gestational age ≤30–32 weeks | Supplemental oxygen use |
| Birth weight <1,500 g | Neonatal sepsis |
| Prematurity (degree correlated to risk) | Hypoxemia / hypercarbia |
| — | Anaemia, low vitamin E |
| — | Failure to thrive |
| — | Caucasian race, male sex |
Risk factors are additive when concurrent. — Wills Eye Manual; Kanski's
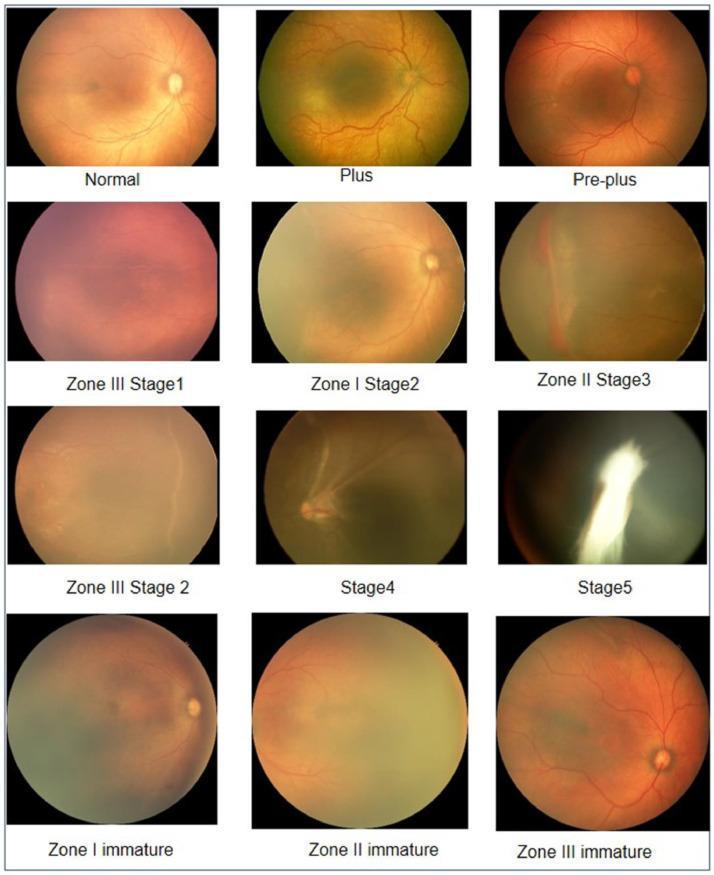
Classification (ICROP 3rd Edition, 2021)
Zones (centred on the optic disc)
- Zone I: Posterior pole — radius = 2× the disc-to-fovea distance. Worst prognosis.
- Zone II: From zone I edge to the nasal ora serrata.
- Zone III: Residual temporal crescent anterior to zone II.
The zone of the most posterior ROP lesion defines the zone. An incursion 1–2 clock hours into a more posterior zone = a "notch."
Stages
| Stage | Description |
|---|---|
| 1 | Thin flat grey-white demarcation line at vascular–avascular junction |
| 2 | Ridge — elevated, has height and width; small neovascular tufts may appear posterior to it |
| 3 | Extraretinal fibrovascular proliferation extending into vitreous from ridge (mild/moderate/severe); peaks ~35 weeks post-conceptual age |
| 4A | Partial retinal detachment — extrafoveal |
| 4B | Partial retinal detachment — involving fovea |
| 5 | Total retinal detachment |
"Plus" Disease
At least 2 quadrants of posterior pole venous engorgement and arterial tortuosity. Denoted with "+", e.g., Stage 3+. Advanced plus disease also shows iris vascular engorgement, poor pupil dilation, and vitreous haze.
Pre-plus disease: Intermediate vascular changes insufficient to diagnose plus disease.
Aggressive posterior ROP (AP-ROP): Rapidly progressive zone I disease with extensive plus disease; may skip stages and progress directly to stage 5. Hemorrhages at the vascular–avascular junction may be present.
Type Classification (Treatment Guidance)
| Type | Criteria | Action |
|---|---|---|
| Type 1 (high-risk, treat) | Zone I, any stage with plus; Zone I, stage 3 without plus; Zone II, stage 2 or 3 with plus | Treat within 48–72 hours |
| Type 2 (watch closely) | Zone I, stage 1–2 without plus; Zone II, stage 3 without plus | Close follow-up |
— Wills Eye Manual; Kanski's Clinical Ophthalmology
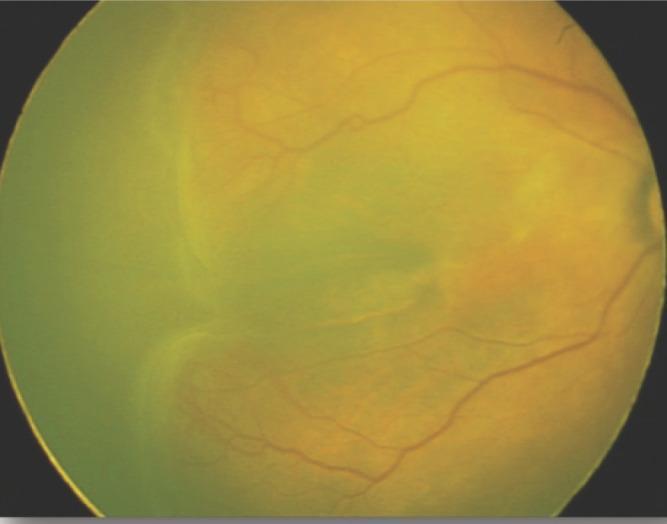
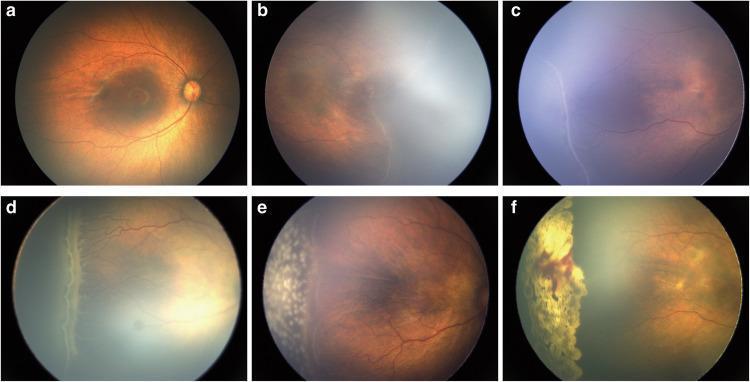
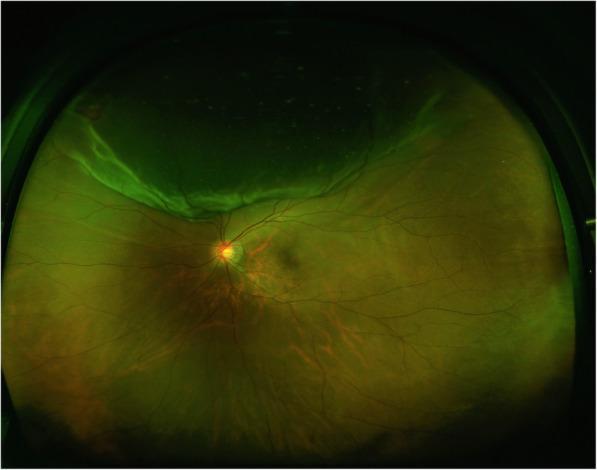
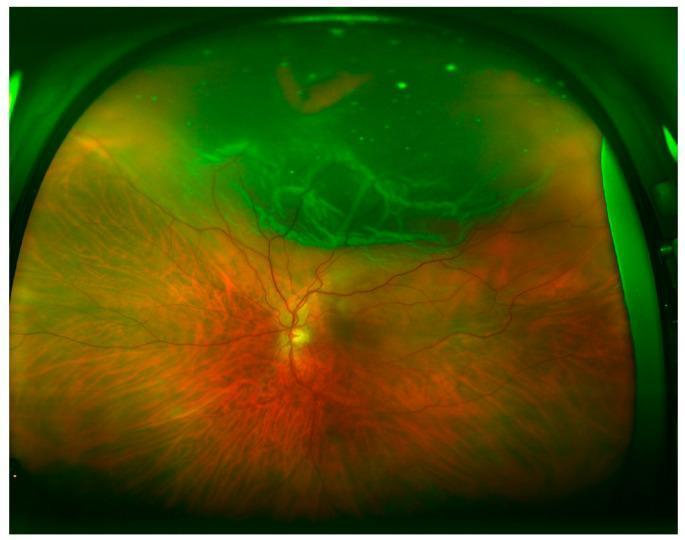
Fundus Images
Staging Reference
Stage 3 ROP — Ridge with Extraretinal Proliferation
Progression Stages 1–3 and Laser Treatment
Screening
| Criterion | Detail |
|---|---|
| Indication | All infants with birth weight ≤1,500 g or gestational age ≤30 weeks |
| Also screen | Infants >30 wks with unstable clinical course / cardiorespiratory support |
| First exam timing (≤27 wks GA) | At 31 weeks postmenstrual age (PMA) |
| First exam timing (≥28 wks GA) | At 4 weeks chronologic age |
| <25 wks GA | Consider at 6 weeks chronologic age (earlier if severe comorbidities) — to detect AP-ROP |
Examination is by dilated indirect ophthalmoscopy.
— Harriet Lane Handbook, 23e; Wills Eye Manual
Treatment
Type 1 ROP / Threshold Disease
Laser photocoagulation (preferred over cryotherapy) — near-confluent ablation of the avascular peripheral retina. Must be done within 48–72 hours of diagnosis.
Anti-VEGF Therapy
Intravitreal bevacizumab (0.625 mg / 0.025 mL) is an emerging option, particularly for:
- Zone I cases (very posterior disease)
- When laser is not available
Long-term systemic effects in preterm infants are not yet fully established. If anti-VEGF is used, extended follow-up is mandatory due to risk of recurrence after 65–70 weeks PMA if retinal vascularization remains incomplete.
Stages 4–5 (Retinal Detachment)
Surgical repair by vitrectomy.
— Wills Eye Manual; Kanski's Clinical Ophthalmology
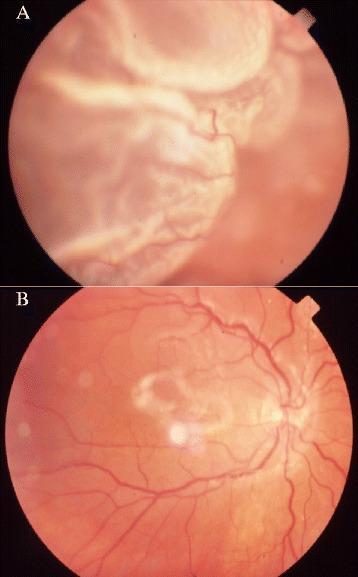
Cicatricial (Regressed) Disease
~20% of infants with active ROP develop cicatricial complications:
- Temporal vitreoretinal fibrosis
- Straightening of vascular arcades
- Macular dragging (disc and macula dragged temporally)
- Falciform retinal fold
- Retinal detachment / total detachment ("retrolental fibroplasia")
- Secondary angle-closure glaucoma (forward displacement of iris-lens diaphragm)
More posterior and more advanced active disease → worse cicatricial sequelae. — Kanski's Clinical Ophthalmology
Follow-Up Schedule
| Finding | Follow-up interval |
|---|---|
| Zone I, no ROP; zone I stage 1–2; zone II stage 3; AP-ROP concern | ≤1 week |
| Posterior zone II, immature; zone II stage 2; zone I regressing | 1–2 weeks |
| Zone II, no ROP; zone II stage 1; zone II regressing | 2 weeks |
| Zone III stage 1–2; zone III regressing | 2–3 weeks |
Discontinue acute screening when: Zone III vascularization attained without prior zone I/II ROP; PMA ≥50 weeks with no disease worse than zone II stage 3; or full vascularization to the ora serrata (for anti-VEGF–treated eyes).
Lifelong annual follow-up is indicated due to increased lifetime risk of myopia, strabismus, amblyopia, macular dragging, cataracts, glaucoma, and retinal detachment. — Wills Eye Manual
Differential Diagnosis
- FEVR (Familial Exudative Vitreoretinopathy): Hereditary, often asymmetric, no prematurity history
- Incontinentia pigmenti: X-linked dominant (girls); skin, CNS, dental anomalies
- Other causes of leukocoria (retinoblastoma, Coats disease, etc.)
Retinal detachment
Finding Sources
Searching Images
retinal detachment types rhegmatogenous tractional exudative fundus
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have a comprehensive dataset. Here is the full structured answer.
Retinal Detachment
Definition
Retinal detachment (RD) is separation of the neurosensory retina from the retinal pigment epithelium (RPE). It is broadly classified into rhegmatogenous (break-related) and non-rhegmatogenous (tractional and exudative) types based on the presence or absence of a retinal break.
— Robbins & Kumar Pathologic Basis of Disease
Types
1. Rhegmatogenous Retinal Detachment (RRD)
Most common type. Incidence ~1 in 10,000/year; both eyes eventually affected in ~10%.
Pathogenesis: A full-thickness retinal break (tear or hole) — in concert with vitreoretinal traction and at least partial vitreous liquefaction — allows liquefied vitreous to seep through the break into the subretinal space, separating the neurosensory retina from the RPE. Without liquefied vitreous and traction, RD almost never occurs even with a break present.
Causes of retinal breaks:
- Posterior vitreous detachment (PVD): vitreous collapses and exerts traction at points of strong retinal adhesion → horseshoe (flap) tears
- Lattice degeneration, snailtrack degeneration
- High myopia (>40% of RDs occur in myopic eyes): degeneration is more common; also at risk from macular holes
- Vitreous loss during cataract surgery or Nd:YAG laser capsulotomy
- Trauma
Distribution of breaks (~60% superotemporal, 15% superonasal, 15% inferotemporal, 10% inferonasal). ~50% of eyes with RD have more than one break, usually within 90° of each other.
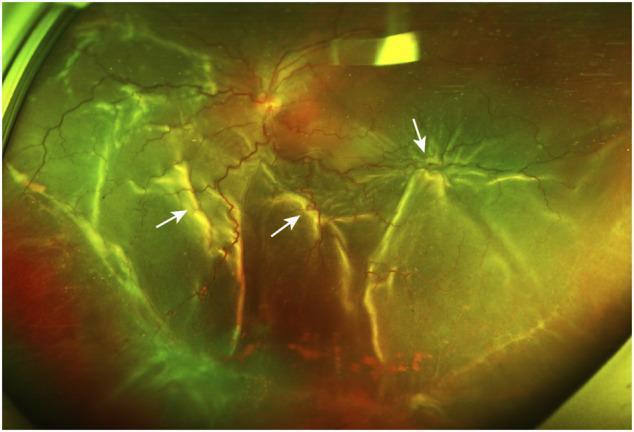
2. Tractional Retinal Detachment (TRD)
Pathogenesis: Progressive contraction of fibrovascular membranes over large areas of vitreoretinal adhesion pulls the retina off the RPE — without a retinal break. PVD in these eyes is gradual and incomplete (unlike the acute PVD in RRD).
Causes:
- Proliferative diabetic retinopathy (most common)
- Retinopathy of prematurity (ROP)
- Sickle cell retinopathy
- Penetrating posterior trauma
- Proliferative vitreoretinopathy (PVR)
- Toxocariasis, FEVR
Types of traction:
- Tangential: epiretinal membrane contraction → retinal puckering
- Anteroposterior: fibrovascular membranes from posterior retina to vitreous base
- Bridging: membranes between different retinal areas, pulling them together
3. Exudative (Serous) Retinal Detachment
Pathogenesis: Subretinal fluid accumulates without a break or traction — leakage overwhelms the RPE pumping mechanism. Fluid accumulates under the retina from choroidal or retinal vascular sources.
Causes:
| Category | Examples |
|---|---|
| Neoplastic | Choroidal melanoma, metastases, choroidal hemangioma, retinoblastoma |
| Inflammatory | Vogt-Koyanagi-Harada (VKH) syndrome, posterior scleritis, sympathetic ophthalmia |
| Vascular | Coats disease, CNV, malignant hypertension, preeclampsia |
| Congenital | Optic pit, morning glory, choroidal coloboma |
| Iatrogenic | Post RD surgery, panretinal photocoagulation |
| Idiopathic | Uveal effusion syndrome, central serous chorioretinopathy (bullous) |
Key pearl: An intraocular tumour should be considered the cause of an exudative RD until proved otherwise. — Kanski's Clinical Ophthalmology
Clinical Features
Symptoms (RRD)
| Symptom | Explanation |
|---|---|
| Flashing lights (photopsia) | Vitreoretinal traction with acute PVD |
| Floaters (vitreous haemorrhage or pigment) | "Tobacco dust" = pigment in vitreous after RPE disruption |
| Curtain/shadow in visual field | Accumulating SRF detaching peripheral retina |
| Central vision loss | Macular involvement by SRF |
- ~60% of RRD patients report premonitory photopsia and floaters
- A lower field defect (superior break) is noticed more quickly than upper defect
- Field defect may partially resolve in the morning (spontaneous overnight reabsorption of SRF), then return during the day
Tractional RD: Photopsia and floaters are typically absent (no acute PVD); visual field loss progresses slowly and may be stable for months–years.
Exudative RD: Photopsia absent (no vitreoretinal traction); floaters if associated vitritis; both eyes may be involved simultaneously (e.g., VKH).
Signs
Rhegmatogenous RD
- Convex, corrugated, opaque retinal surface (retinal oedema)
- Mobile retina with shifting SRF
- Loss of choroidal pattern beneath elevated retina
- Retinal break(s) identifiable on indirect ophthalmoscopy
- Tobacco dust (Shafer sign) — pigmented cells in anterior vitreous (pathognomonic for break/RD)
- Vitreous haemorrhage in ~10%
Tractional RD
- Concave configuration, smooth surface (no break)
- Severely reduced retinal mobility; no shifting fluid
- Fibrovascular/vitreous membranes visible exerting traction
- Detachment rarely extends to ora serrata
- May become convex (combined TRD/RRD) if a new break develops in the tractional retina
Exudative RD
- Convex, smooth (not corrugated) surface
- Shifting subretinal fluid — hallmark: upright position → SRF collects inferiorly; supine → fluid shifts posteriorly detaching superior retina
- No retinal break
- Detachment typically does not extend to ora serrata
- Underlying tumour or choroidal pathology may be visible
- "Leopard spots" of RPE clumping after resolution
Fundus Images
Bullous exudative RD with subretinal fluid

RRD with PVR — pre and post vitrectomy/scleral buckle
Lincoff's Rules (SRF Distribution → Predict Break Location)
| SRF pattern | Likely break location |
|---|---|
| Shallow inferior RD, SRF higher on temporal side | Inferior temporal break |
| Inferior RD with equal fluid levels | Break at 6 o'clock |
| Bullous inferior RD | Break above the horizontal meridian |
| Subtotal RD with superior wedge of attached retina | Peripheral break nearest the highest border |
| SRF crosses vertical midline superiorly | Break near 12 o'clock |
The quadrant of the visual field defect is in the opposite quadrant to the primary break.
Longstanding RD Features
- Retinal thinning (atrophy) — do not misdiagnose as retinoschisis
- Intraretinal cysts (after ~1 year; usually resolve post-surgery)
- Subretinal demarcation lines ("high water marks") — RPE proliferation at flat–detached junction; appear after ~3 months
Proliferative Vitreoretinopathy (PVR) — Major Complication
PVR = epiretinal and subretinal membrane formation by RPE cells and retinal glial cells → tangential retinal traction → fixed folds → funnel-shaped detachment.
| Grade | Features |
|---|---|
| A (Minimal) | Diffuse vitreous haze, tobacco dust, pigmented clumps |
| B (Moderate) | Wrinkling of inner retinal surface, rolled break edges |
| C (Severe) | Fixed retinal star folds, full-thickness folds, funnel RD |
PVR most commonly follows surgery for RRD or penetrating injury.
Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Degenerative retinoschisis | Bilateral, smooth, bullous, usually inferotemporal; no vitreous pigment or haemorrhage; inner/outer retinal holes may be present |
| X-linked retinoschisis | Stellate foveal petaloid changes; NFL separation; no RD initially |
| Choroidal detachment | Orange-brown, immobile, 4-lobed, extends anterior to ora serrata, low IOP, limited by vortex veins posteriorly |
| FEVR | Hereditary, asymmetric, no prematurity history |
Workup
- Dilated indirect ophthalmoscopy with scleral depression — both eyes (fellow eye ~10% risk)
- B-scan ultrasound — if media opacities prevent fundus view
- OCT — tractional membranes, macular involvement, retinoschisis vs RD
- IVFA — exudative RD: identify leakage source
- Systemic workup — if exudative RD (malignancy screen, inflammatory markers, BP)
Treatment
Rhegmatogenous RD
| Urgency | Situation | Action |
|---|---|---|
| Emergency | Macula-on (threatened) | Surgery ASAP |
| Urgent (within 72h) | Macula-off, recent onset | Better outcomes if within 72 hours |
| Semi-urgent (≤7 days) | Chronic macula-off | Within 1 week if possible |
Surgical options:
1. Pneumatic Retinopexy (outpatient, minimally invasive)
- Intravitreal gas bubble (SF₆ or longer-acting C₃F₈) + cryotherapy or laser
- Seals the break and tamponades the retina
- Reserved for uncomplicated RD with a small break or cluster of breaks <2 clock hours in the upper two-thirds of the peripheral retina
- Less invasive but lower success rates than scleral buckling
2. Scleral Buckling
- Silicone explant sutured to the sclera creates an inward indentation (buckle)
- Closes retinal breaks by apposing RPE to neurosensory retina and relieves vitreoretinal traction
- Configurations: radial, segmental, circumferential, or encircling
- Combined with cryotherapy to the break
- Preferred for post-traumatic dialysis detachments
3. Pars Plana Vitrectomy (PPV)
- Internal approach; removes vitreous, relieves traction
- Used for complex RRD, PVR, giant retinal tears, vitreous haemorrhage obscuring the break
- May use silicone oil or gas tamponade
- Also the primary approach for TRD (diabetic)
Tractional RD
- Depends on location (macular threat), etiology, and fellow eye status
- Surgical repair by vitrectomy with membrane peeling
Exudative RD
- Treat the underlying cause — detachment typically resolves
- Systemic corticosteroids for inflammatory causes (VKH, posterior scleritis)
- Anti-VEGF or laser for vascular causes (CNV, Coats)
- Radiation/surgical resection for choroidal tumours
Follow-Up
- All RRD patients require urgent referral to a retina specialist
- Post-op schedule: 1 day → 1 week → 1 month → 2–3 months → every 6–12 months
- Fellow eye must be examined and treated for predisposing lesions (lattice degeneration, tears)
- Serous and TRD follow-up depends on underlying etiology
— Kanski's Clinical Ophthalmology, 10e; Wills Eye Manual; Robbins & Kumar Pathologic Basis of Disease
Retinal detachment post graduate level
Finding Sources
Searching Images
rhegmatogenous retinal detachment fundus horseshoe tear break
Reading File
Reading File
Searching Images
proliferative vitreoretinopathy PVR fixed star folds retinal detachment surgery
Reading File
Reading File
Searching Images
scleral buckling surgery explant retinal detachment repair diagram
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive postgraduate-level detail. Let me compile the full answer.
Retinal Detachment — Postgraduate Level
1. Anatomy & Pathophysiological Basis
The neurosensory retina (NSR) and retinal pigment epithelium (RPE) are derived from the two layers of the optic cup and are not truly adherent — they are apposed within a potential subretinal space. Retinal attachment is maintained by:
- Active RPE fluid transport (pumping fluid from subretinal to choroidal space)
- Interdigitation of photoreceptor outer segments with RPE microvilli
- Interphotoreceptor matrix (IPCM) proteins
- Intraocular pressure maintaining apposition
- Vitreous face providing gentle support posteriorly
Any mechanism that overwhelms these forces — a retinal break + traction, fibrovascular traction, or RPE/choroidal fluid barrier failure — results in retinal detachment.
2. Classification
2.1 Rhegmatogenous Retinal Detachment (RRD)
Epidemiology: ~1 in 10,000/year. Fellow eye eventually affected in ~10%. >40% occur in myopic eyes.
Triad required for RRD:
- Full-thickness retinal break (tear or hole)
- Vitreous liquefaction (synchysis)
- Vitreoretinal traction
Without at least partial liquefaction and traction, a break almost never causes RD.
Types of Retinal Breaks
| Type | Mechanism | Risk of RD |
|---|---|---|
| Horseshoe (flap/U) tear | Acute PVD — vitreous traction avulses a flap | HIGH |
| Operculated hole | Flap fully avulsed; traction released | Moderate |
| Atrophic round hole | Focal retinal thinning; no acute PVD | Low (slow onset) |
| Dialysis | Circumferential tear at ora serrata; trauma or idiopathic | Variable |
| Giant retinal tear | Break ≥3 clock hours (90°); posterior flap inverts | Very high |
| Macular hole | Tangential traction on fovea; RD confined to posterior pole (especially high myopia) | Low except in myopia |
Predisposing Lesions
- Lattice degeneration — most important; peripheral atrophic thinning with overlying vitreous liquefaction and firm margin adhesion; atrophic holes within lattice + horseshoe tears at margin
- Snailtrack degeneration — silvery-white frost; atrophic holes more common than in lattice
- Retinoschisis — splitting within the retina; outer leaf holes + inner leaf holes → RD risk
- Pavingstone (cobblestone) degeneration — focal RPE/choroidal atrophy; very low RD risk
- Vitreous base avulsion — traumatic
- High myopia — thin retina, early PVD, large vitreous cavity
Subretinal Fluid (SRF) Dynamics — Modified Lincoff's Rules
SRF spread governed by: (a) gravity, (b) ora serrata/optic nerve as anatomical limits, (c) break location.
| SRF pattern | Predicted break location |
|---|---|
| Shallow inferior RD, SRF higher temporally | Inferior temporal break |
| Inferior RD, equal fluid levels | Break at 6 o'clock |
| Bullous inferior RD | Break above the horizontal meridian |
| Upper nasal break | SRF revolves around optic disc, rises temporally to the level of the break |
| Subtotal RD with superior wedge of attached retina | Break at periphery nearest the highest border |
| SRF crosses vertical midline superiorly | Break near 12 o'clock; lower RD edge = side of break |
The quadrant of the visual field defect is in the opposite quadrant to the primary break.
Break distribution in eyes with RRD: 60% superotemporal, 15% superonasal, 15% inferotemporal, 10% inferonasal. ~50% of eyes have >1 break, usually within 90° of each other.
2.2 Tractional Retinal Detachment (TRD)
Mechanism: Progressive contraction of fibrovascular epiretinal/subretinal membranes over large areas of vitreoretinal adhesion. PVD in TRD is gradual and incomplete (unlike the acute PVD of RRD) — plasma constituents leak from fibrovascular networks adherent to the posterior vitreous into the gel, which contracts.
Causes
- Proliferative diabetic retinopathy (PDR) — most common
- Retinopathy of prematurity (ROP)
- Sickle cell retinopathy
- Penetrating posterior trauma
- Proliferative vitreoretinopathy (PVR) post-surgery
- Toxocariasis, FEVR
Types of Traction in PDR
| Type | Description |
|---|---|
| Tangential | Epiretinal membrane contraction → retinal puckering, vessel distortion |
| Anteroposterior | Fibrovascular membranes from posterior retina to vitreous base |
| Bridging (trampoline) | Membranes between vascular arcades, pulling them together |
Key distinguishing signs
- Concave configuration (vs. convex in RRD/exudative)
- No retinal break
- Severely reduced retinal mobility; no shifting fluid
- Rarely extends to ora serrata
- If a tractional break develops → combined TRD/RRD (now convex, more urgent)
2.3 Exudative (Serous) Retinal Detachment
Mechanism: Fluid accumulates in the subretinal space without break or traction — RPE fluid transport overwhelmed by excess leakage from inflamed, neoplastic, or dysregulated choroidal/retinal vasculature.
Causes
| Category | Specific conditions |
|---|---|
| Neoplastic | Choroidal melanoma (commonest), metastases, choroidal hemangioma, retinoblastoma, multiple myeloma, retinal capillary hemangioblastoma |
| Inflammatory | Vogt-Koyanagi-Harada (VKH), posterior scleritis, sympathetic ophthalmia |
| Vascular | Coats disease, CNV, malignant hypertension, preeclampsia |
| Congenital | Optic pit, morning glory, choroidal coloboma |
| Iatrogenic | Post-RD surgery, panretinal photocoagulation |
| Idiopathic | Uveal effusion syndrome, bullous CSCR |
An intraocular tumour must be considered the cause of exudative RD until proved otherwise. — Kanski's Clinical Ophthalmology
Hallmark: Shifting subretinal fluid — SRF redistributes with gravity; inferior detachment in upright position, posterior/superior detachment in supine. Surface is smooth (not corrugated). Detachment does not extend to ora serrata.
3. Clinical Assessment
Symptoms
| Feature | RRD | TRD | Exudative |
|---|---|---|---|
| Photopsia | Present (~60%) | Absent | Absent |
| Floaters | Present | Absent | Present if vitritis |
| Curtain/field defect | Sudden onset, progresses | Slow, may be stable for months | Sudden to rapid |
| Morning improvement | Common (SRF reabsorbed overnight) | No | No |
| Bilateral | Rare | Uncommon | Common (VKH, hypertension) |
Signs
| Feature | RRD | TRD | Exudative |
|---|---|---|---|
| Retinal configuration | Convex, corrugated, opaque | Concave, smooth | Convex, smooth |
| Retinal mobility | Moderate | Severely reduced | Highly mobile |
| Shifting SRF | Present | Absent | Present (pathognomonic) |
| Retinal break | Present | Absent | Absent |
| Ora serrata extension | Extends to ora | Rarely reaches ora | Does not reach ora |
| Tobacco dust (Shafer sign) | Pathognomonic | Absent | Absent |
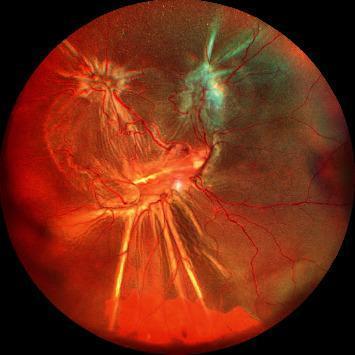
Fundus Images
Horseshoe retinal tear causing RRD

Macula-on RRD with superior horseshoe tear
Macula-off total RRD
4. Longstanding RD — Specific Features
- Retinal thinning (atrophy) — can mimic retinoschisis but has different mobility
- Intraretinal cysts — after ~1 year; tend to resolve post-surgery
- Demarcation lines ("high water marks") — RPE cell proliferation at junction of flat and detached retina; develop ~3 months after onset; represent increased adhesion but do not invariably limit SRF spread
- Macular pseudohole — impression of macular hole due to thin foveal retina when the posterior pole is detached; distinguish from true macular hole (important as macular holes cause RD in high myopia)
5. Proliferative Vitreoretinopathy (PVR) — The Major Complication
PVR is the principal cause of failed RD surgery and of late re-detachment. It results from epiretinal and subretinal membrane formation — by RPE cells, Müller cells, and fibrous astrocytes — that has migrated through retinal breaks and the vitreous, subsequently contracting to produce tangential retinal traction and fixed folds.
PVR Grading (Retina Society Classification)
| Grade | Features |
|---|---|
| A (Minimal) | Diffuse vitreous haze ("tobacco dust"), vitreous pigment clumps, pigmented clusters on inferior retina |
| B (Moderate) | Wrinkling of inner retinal surface; decreased vitreous gel mobility; rolled edges of retinal breaks; vascular tortuosity; retinal stiffness. Epiretinal membranes usually not clinically visible |
| C (Marked) | Rigid full-thickness retinal folds, often star-shaped; heavy vitreous condensation and strands. Divided into anterior (CA) and posterior (CP) based on equatorial location; extent expressed in clock hours |
| Advanced C | Gross reduction of retinal mobility; retinal shortening; funnel-shaped detachment |
PVR — Surgical Management
Goals: Release transvitreal traction (vitrectomy) + tangential surface traction (membrane dissection) → restore retinal mobility → allow break closure.
- Localized star folds: Remove central plaque of epiretinal membrane using picks or scissors; peel from retinal surface
- Internal limiting membrane (ILM) peeling in advanced PVR improves surgical success
- Relaxing retinotomy (peripheral or posterior) may be required for severe retinal shortening
- Perfluorocarbon liquid (PFCL) used intraoperatively to stabilize retina
- Replaced with long-acting gas (C₃F₈) or silicone oil for tamponade
PVR Fundus Images
6. Surgical Options for RRD
6.1 Pneumatic Retinopexy
Outpatient "office-based" procedure. Intravitreal gas bubble + cryotherapy or laser photocoagulation to seal the break.
Gases used:
- SF₆ (sulfur hexafluoride): doubles volume at 100%; lasts 10–14 days
- C₂F₆ (perfluoroethane): triples volume; lasts 30–35 days
- C₃F₈ (perfluoropropane): quadruples volume; lasts ~8 weeks (longest-acting)
Strict selection criteria:
- Single break or cluster of breaks spanning <2 clock hours
- Located in the upper two-thirds of the peripheral retina
- No significant PVR
Limitation: Lower anatomical success rates than scleral buckling.
Contraindication: Air travel until gas bubble fully absorbed (risk of acute IOP rise from gas expansion at altitude).
6.2 Scleral Buckling (External Surgery)
A silicone explant sutured to the external sclera creates an inward indentation (buckle) that:
- Closes retinal breaks by apposing RPE to NSR
- Reduces dynamic vitreoretinal traction at the break
- Relieves the vitreous base traction anteriorly
Explant types: Soft or hard silicone; sponge (segmental) or solid (encircling/circumferential)
Configuration choices: Radial, segmental, circumferential, or encircling — determined by break size, number, and configuration.
Technique steps: Peritomy → localization of breaks → cryoretinopexy → explant suturing → check buckle height → SRF drainage (if needed) → gas injection (if needed).
Always indicated for: Post-traumatic dialysis detachment.
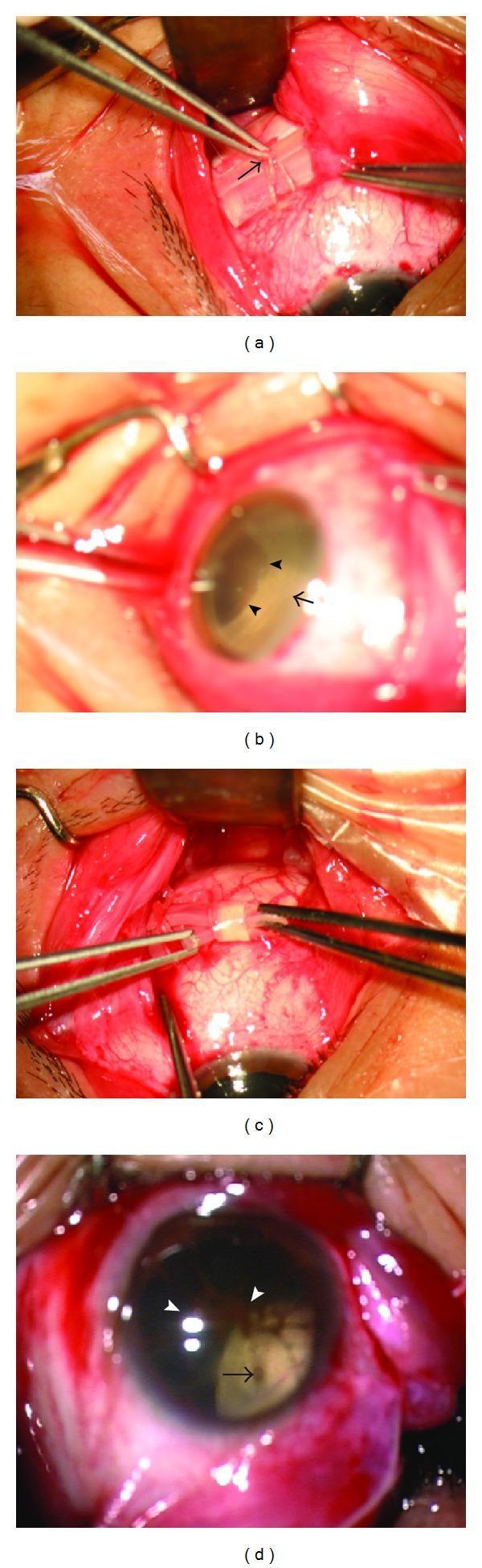
Scleral buckling intraoperative photographs:
Common complications:
- Buckle infection/exposure/extrusion
- Diplopia (extraocular muscle tethering)
- Choroidal effusion
- Anterior segment ischaemia (encircling buckle)
- Induced myopia (encircling buckle increases axial length)
- Fish-mouthing of large U-tears after buckling
- Refractive change
Causes of failure:
- PVR — most common cause of late failure
- Failure to close all breaks
- Development of new breaks
6.3 Pars Plana Vitrectomy (PPV) — Internal Surgery
Modern gauge systems:
- 20-gauge (0.9 mm) — conventional
- 23-gauge, 25-gauge, 27-gauge — sutureless transconjunctival microincision vitrectomy (MIVS); now standard of care; shorter operative time, less trauma, faster rehabilitation
Basic PPV steps (for RD):
- Three-port entry: infusion cannula (IOP maintenance), light pipe (illumination), cutter
- Core vitrectomy → posterior vitreous detachment (PVD) induction
- Triamcinolone acetonide to stain vitreous for complete removal
- SRF drainage (internal via break or external via needle)
- Endolaser photocoagulation around all breaks
- Fluid–air exchange → gas or silicone oil tamponade
- Postoperative positioning to apply tamponade against breaks
Tamponading agents:
| Agent | Properties | Duration | Indications |
|---|---|---|---|
| Air | Non-expanding | Days | Short tamponade |
| SF₆ | 2× expansion at 100% | 10–14 days | Simple superior RD |
| C₂F₆ | 3× expansion | 30–35 days | Complex RD |
| C₃F₈ | 4× expansion | ~8 weeks | PVR, inferior breaks |
| Silicone oil | Non-expanding, permanent until removed | Months–years (then removed) | PVR, inferior RD, monocular patients, inability to posture |
| Heavy silicone oil | Higher specific gravity than water | Permanent until removed | Inferior breaks, PVR with inferior predominance |
| PFCL (perfluorocarbon liquid) | Intraoperative use only; heavier than water; flattens posterior retina | Intraoperative | Stabilization during membrane peeling, giant tears |
PPV indications over scleral buckle:
- PVR (any grade C or worse)
- Giant retinal tear (≥3 clock hours / 90°)
- Large posterior breaks
- Vitreous haemorrhage obscuring the break
- Diabetic TRD
- Post-traumatic RD
- Aphakic/pseudophakic RD with multiple/posterior breaks
- Previous failed scleral buckle
PPV-specific complications:
- Silicone oil glaucoma: Early → pupillary block (prevented by inferior Ando iridectomy in aphakic eyes); Late → emulsified oil in trabecular meshwork
- Cataract: Gas-induced (transient feathering of posterior subcapsular lens); silicone oil-induced (almost universal in phakic eyes — develop in virtually all cases)
- Gas-related IOP rise: Overfill or air travel
- Band keratopathy: With extended silicone oil
- Endophthalmitis: Rare but potential; slightly higher concern with small-gauge
- Intraocular gas expansion: Risk with nitrous oxide anaesthesia (must be avoided)
7. Specific Surgical Scenarios
Post-Cataract Surgery RRD
RRD after uncomplicated phacoemulsification is uncommon. Pre-operative risk factors: lattice degeneration, retinal breaks, high myopia. Key intraoperative risk: vitreous loss. PPV is usually employed.
Giant Retinal Tear (GRT)
Break ≥90° (3 clock hours). The posterior retinal flap tends to invert (fold posteriorly), preventing self-sealing. PFCL used intraoperatively to unfold and stabilize the flap, then endolaser followed by gas or silicone oil tamponade.
Macular Hole RD (High Myopia)
Posterior staphyloma + foveal thinning → macular hole → shallow RD confined to posterior pole. Initial SRF around hole. PPV + ILM peeling + gas (C₃F₈) face-down positioning.
8. Visual Prognosis
| Factor | Better prognosis | Worse prognosis |
|---|---|---|
| Macular status | Macula-on | Macula-off |
| Timing (macula-off) | Operated within 72 hours | Chronic, >7–10 days |
| Break location | Inferior, peripheral | Posterior, zone I |
| PVR | Absent | Grade C or higher |
| Duration of detachment | Short | Long (>1 year → photoreceptor atrophy) |
| Fellow eye | Good vision (motivates early treatment) | — |
Urgent surgery is needed in an acute progressive RD if the macula is threatened. Even if the macula is off, results are better if surgery is done within 72 hours. — Kanski's Clinical Ophthalmology
Visual outcomes for macula-off detachments do not change significantly if surgery is performed within 7–10 days of onset — beyond that, outcomes deteriorate. — Wills Eye Manual
9. Investigative Workup
| Investigation | Indication |
|---|---|
| Dilated indirect ophthalmoscopy + scleral depression | All cases; both eyes examined |
| B-scan ultrasound | Media opacity (VH, cataract, corneal scar) preventing fundal view |
| OCT | Macular status (on/off, pseudohole vs true hole); tractional membranes; subretinal fluid confirmation |
| IVFA | Exudative RD — identify leakage point; CNV characterisation |
| Fundus drawing / wide-field photography | Documentation, surgical planning |
| Systemic workup | Exudative RD → malignancy screen, autoimmune markers (ANA, chest XR for sarcoid/TB), BP |
10. Three Laws of Failed RD Surgery
The three commonest causes of failed retinal detachment surgery are: proliferative vitreoretinopathy, failure to close all breaks, and the development of new breaks. — Kanski's Clinical Ophthalmology, 10e
Sources: Kanski's Clinical Ophthalmology, 10e; Wills Eye Manual, 8e; Robbins & Kumar Pathologic Basis of Disease, 10e
Minimally invasive glaucoma surgeries
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.